Entrapment of the Impella device by the guiding catheter: a cautionary pitfall of Impella-protected percutaneous coronary intervention
Hiroyuki Yamamoto, Nobuhiro Watanabe, Koki Matsuo, Tomofumi Takaya

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
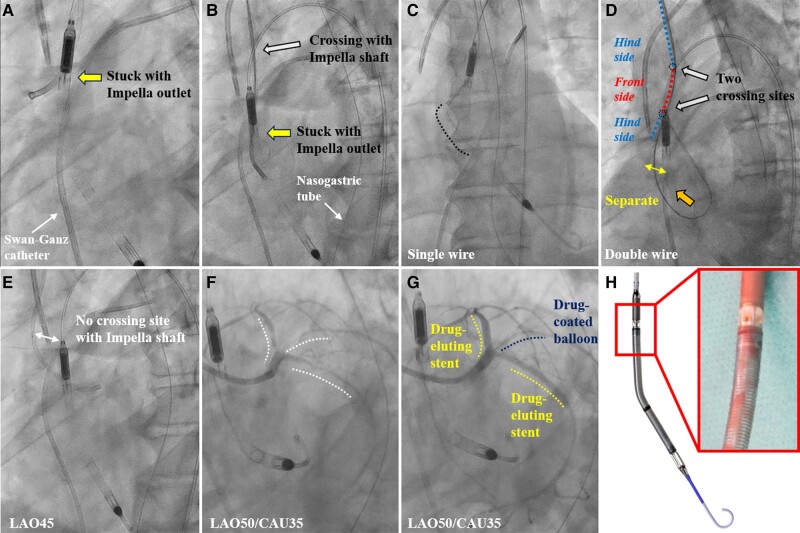 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCoronary Interventions and Diagnostics · Cardiac Imaging and Diagnostics · Vascular Procedures and Complications
Case description
A 67-year-old man presented with acute decompensated heart failure and cardiogenic shock. Transthoracic echocardiography revealed severe global left ventricular hypokinesis with a left ventricular ejection fraction of 25%. Emergency coronary angiography revealed multiple stenoses without obstruction. Therefore, transfemoral left ventricular assist (Impella CP, Abiomed, USA) support was performed to increase coronary flow through diastolic augmentation. However, low cardiac output syndrome made removing the Impella device difficult, requiring percutaneous coronary revascularization. Although a backup guiding catheter (GC; Hyperion SPB3.5, Asahi Intecc, Japan) was initially used via the right radial artery, cannulating the coronary artery was difficult. After manipulating the GC clockwise, the Impella device moved upwards with the GC motion, suggesting entrapment of the GC with the Impella outlet (Figure 1A and B; Supplementary material online, Video S1). We pushed the GC to the cardiac side and attempted to extract the GC using a single 0.035 inch conventional wire; however, it was difficult because of the interaction. Next, manually adjusting the Impella shaft’s position via the femoral artery while pushing the 0.035 inch Amplatz Extra-Stiff guidewire (Cook, USA) inserted into the GC as double wires against the aortic cusp disengaged the entrapment (Figure 1C and D). Subsequent percutaneous coronary intervention (PCI) using a non-backup type GC (Hyperion JL3.5, Asahi Intecc, Japan) was successfully performed without interaction with the Impella, and the patient recovered from low cardiac output syndrome (Figure 1E–G).
(A, B) Angiograms showing the positional relationship between the guiding catheter and the Impella. The Impella device moves upward and downward with the guiding catheter motion, suggesting entrapment of the guiding catheter with the Impella outlet. (C) The interaction between the guiding catheter and Impella outlet is not improved using a single wire. (D) The guiding catheter separates from the Impella outlet when double wires are pushed onto the aortic cusp. (E) No interaction between the Impella device and Judkins left guiding catheter. (F) Before and (G) after percutaneous coronary intervention. White dotted line shows stenosis. (H) Magnified view showing the windows of the Impella outlet.
Impella effectively stabilizes haemodynamics in patients with cardiogenic shock and complex high-risk PCI.^1^ Impella outlet comprises five windows that could interact with other devices (Figure 1H).^2^ The positional relationship between the Impella outlet and GC should be considered when manipulating GC in the ascending aorta. To avoid entrapment of the GC and Impella device, we suggest inserting the GC from a coronary access route not crossing the Impella device and avoiding manipulation of the GC without turning it drastically. This case demonstrated that PCI via the right upper limb may result in the GC crossing the Impella, potentially causing device interference and Impella dislocation.
Supplementary Material
ytae096_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Fujimoto Y, Sakakura K, Fujita H. Complex and high-risk intervention in indicated patients (CHIP) in contemporary clinical practice. Cardiovasc Interv Ther 2023;38:269–274.36971962 10.1007/s 12928-023-00930-1 · doi ↗ · pubmed ↗
- 2Sharma A, Bertog S, Mbai M. Impella placement across transcatheter aortic valves: a potential for device-device interaction. JACC Cardiovasc Interv 2020;13:2574–2575.32861634 10.1016/j.jcin.2020.05.047 · doi ↗ · pubmed ↗