Tricuspid stenosis due to pectus excavatum in a paediatric patient with trisomy 21
Yuya Fujita, Ayako Chida-Nagai, Atsuhito Takeda

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
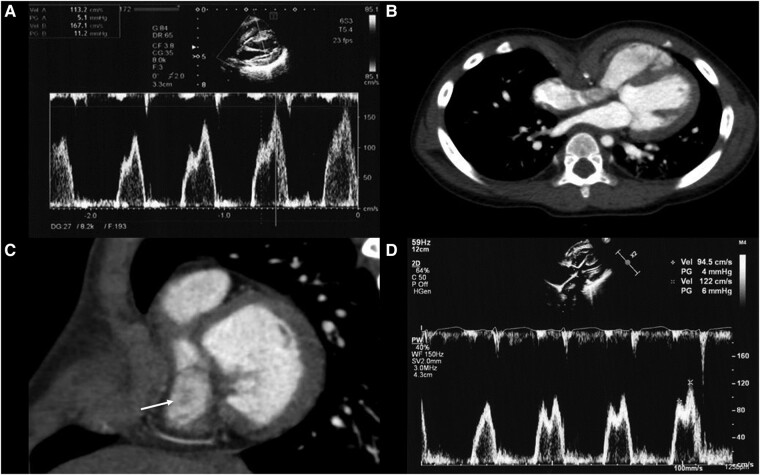 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPectus Deformity Diagnosis and Treatment · Congenital limb and hand anomalies
A male infant was diagnosed with trisomy 21 (T21) and complete atrioventricular septal defect at birth. Pulmonary artery banding was performed at 3 months, followed by intracardiac repair at 5 months. Transthoracic echocardiography (TTE) after the second surgery noted a tricuspid valve (TV) annulus diameter of 12.2 mm [105% of normal TV (%N)], with a monophasic TV inflow of 120 cm/s.
Throughout the outpatient follow-up, the pectus excavatum (PE)-related chest deformity progressed. At 3 years old, TTE revealed mild tricuspid stenosis (TS) with a mean transvalvular pressure gradient of 4.5 mmHg. The maximum TV inflow exhibited an E-wave of 113 cm/s and an A-wave of 167 cm/s (Panel A, Supplementary material online, Video S1), indicating right ventricular diastolic dysfunction. Tricuspid valve diameter was 8.8 mm (52%N). Contrast-enhanced chest computed tomography displayed cardiac displacement and right heart compression due to PE (Panel B). The Haller index (calculated by dividing the transverse diameter of the chest by the anteroposterior diameter) was markedly elevated, measuring 6.1. In Panel C, narrowing of the TV can be observed (arrow), as indicated. Concerning the worsening chest deformity and TS progression, PE surgery was performed. Post-operative TTE displayed a mean transvalvular pressure gradient of 2 mmHg, E-wave of 95 cm/s, and A-wave of 122 cm/s (Panel D, Supplementary material online, Video S2). The annulus diameter measured 17.0 mm (99%N), suggesting TS improvement.
A previous report documented instances of right ventricular obstruction resulting from PE, but our report represents the first case of pure TS due to PE in a paediatric patient with T21 after congenital heart disease surgery. We postulate severe PE development from T21-related joint hypermobility compounded by cardiac surgery. In cases of worsening PE, thorough cardiovascular evaluation, including TTE and chest computed tomography, is vital. In conditions such as T21-associated joint hypermobility, remaining vigilant for the possible development or worsening of PE following cardiac surgery is imperative.
Supplementary Material
ytae104_Supplementary_Data