Multiple Ulcers in the Ileum and Lymphadenopathy Following the Usage of Methotrexate in a Patient With Rheumatoid Arthritis: A Case Report
Ryuichi Ohta, Tsuyoshi Mishiro, Yuta Horinishi, Chiaki Sano

TL;DR
An elderly rheumatoid arthritis patient developed severe anemia and intestinal ulcers after methotrexate treatment, highlighting the need for careful monitoring of drug side effects in older adults.
Contribution
This case report documents a rare, non-painful presentation of methotrexate-induced ileal damage and lymphadenopathy in elderly rheumatoid arthritis patients.
Findings
The patient showed multiple ileal ulcers and lymphadenopathy without active bleeding or pain.
Methotrexate cessation and anemia management led to clinical improvement.
Methotrexate-induced lymphoma was ruled out through laboratory and biopsy findings.
Abstract
This case report aims to highlight a rare occurrence of severe anemia and lymphadenopathy secondary to methotrexate (MTX)-induced ileal mucosa damage in a patient with elderly onset rheumatoid arthritis (EORA). We present the case of a 72-year-old female with a history of EORA, treated with MTX, who exhibited hematochezia without accompanying pain, diarrhea, or known infectious contacts. Diagnostic investigations included imaging and endoscopic procedures. The patient's presentation of severe anemia was atypical, given the absence of significant pain or discomfort associated with EORA. The lack of active bleeding observed during endoscopy, coupled with multiple ileal ulcers, suggested a chronic progression of mucosal damage. Laboratory findings, including normal lactate dehydrogenase, soluble interleukin-2 receptor levels, and the absence of malignancy in mucosal biopsies, ruled out…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
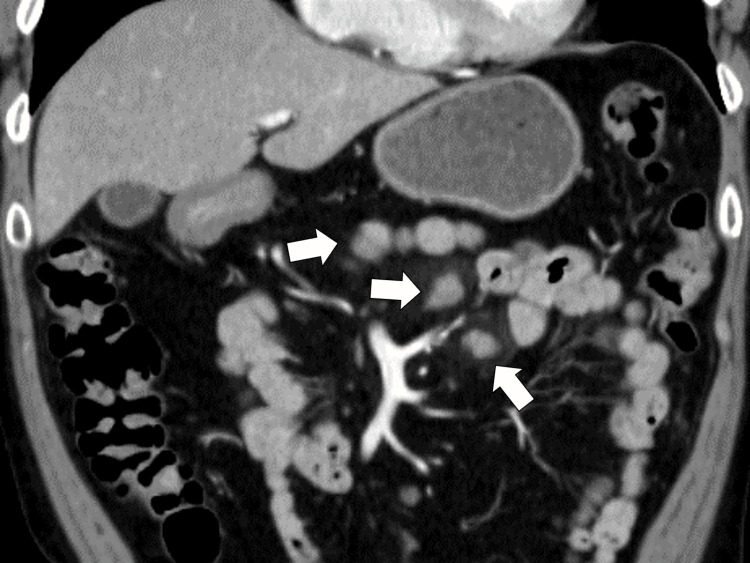 Figure 1
Figure 1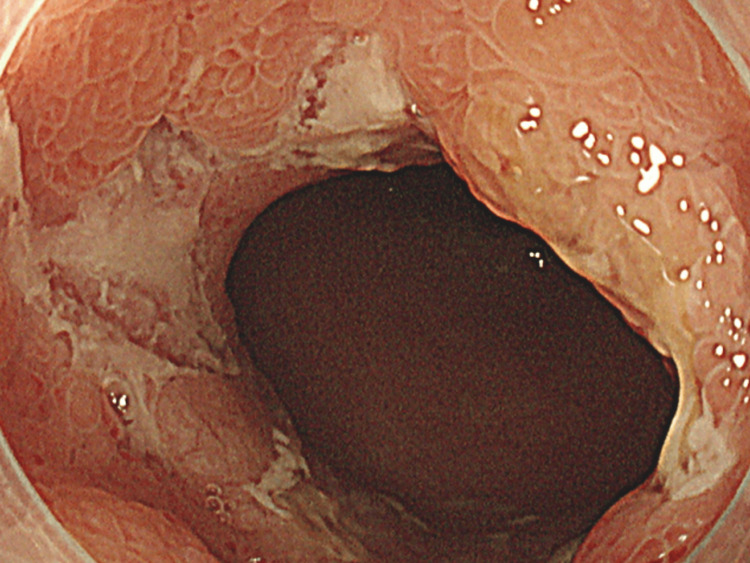 Figure 2
Figure 2| Parameter | Level | Reference |
| White blood cells | 12.7 | 3.5–9.1 × 103/μL |
| Neutrophils | 75.7 | 44.0–72.0% |
| Lymphocytes | 19.8 | 18.0–59.0% |
| Monocytes | 3.4 | 0.0–12.0% |
| Eosinophils | 0.5 | 0.0–10.0% |
| Basophils | 0.6 | 0.0–3.0% |
| Red blood cells | 2.96 | 3.76–5.50 × 106/μL |
| Hemoglobin | 8.9 | 11.3–15.2 g/dL |
| Hematocrit | 26.3 | 33.4–44.9% |
| MCV | 88.9 | 79.0–100.0 fL |
| Platelets | 32.4 | 13.0–36.9 × 104/μL |
| Total protein | 6.3 | 6.5–8.3 g/dL |
| Albumin | 3.8 | 3.8–5.3 g/dL |
| Total bilirubin | 0.4 | 0.2–1.2 mg/dL |
| Aspartate aminotransferase | 34 | 8–38 IU/L |
| Alanine aminotransferase | 45 | 4–43 IU/L |
| Alkaline phosphatase | 70 | 106–322 U/L |
| γ-Glutamyl transpeptidase | 21 | <48 IU/L |
| Lactate dehydrogenase | 203 | 121–245 U/L |
| Blood urea nitrogen | 34.6 | 8–20 mg/dL |
| Creatinine | 0.71 | 0.40–1.10 mg/dL |
| eGFR | 61.3 | >60.0 mL/min/L |
| Serum Na | 138 | 135–150 mEq/L |
| Serum K | 4.4 | 3.5–5.3 mEq/L |
| Serum Cl | 103 | 98–110 mEq/L |
| Serum Ca | 9.1 | 8.8–10.2 mg/dL |
| Serum P | 3.2 | 2.7–4.6 mg/dL |
| Serum Mg | 1.9 | 1.8–2.3 mg/dL |
| Serum iron | 42 | 43-172 mg/dL |
| Ferritin | 51.3 | 14.4–303.7 ng/mL |
| CK | 64 | 56–244 U/L |
| CRP | 0.04 | <0.30 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRheumatoid Arthritis Research and Therapies · Chronic Lymphocytic Leukemia Research · Interstitial Lung Diseases and Idiopathic Pulmonary Fibrosis
Introduction
Rheumatoid arthritis (RA), a chronic inflammatory condition primarily impacting the joints, manifests uniquely in older adults as elderly onset rheumatoid arthritis (EORA) [1]. Within the treatment paradigm for EORA, methotrexate (MTX) has risen as a fundamental treatment, instrumental in reducing disease activity and steering patients toward remission [2]. However, MTX administration, especially in elderly patients, presents distinct challenges [3]. The heightened susceptibility of senior individuals with EORA demands prudent management due to the array of potential adverse effects associated with MTX [3].
In managing EORA with MTX, stringent monitoring of its side effects is essential, requiring detailed medical oversight and immediate intervention. This necessity is accentuated by the variability in both the side effects of MTX and the manifestation of EORA symptoms, which can vary from minor discomforts to severe, potentially life-endangering conditions [4]. Gastrointestinal issues are particularly common among these complications [5]. In certain instances, these symptoms may progress to critical states such as gastrointestinal bleeding and profound anemia, thereby significantly endangering the patient's health and safety [6,7].
This case report presents a 72-year-old female diagnosed with EORA and undergoing MTX treatment, who developed acute gastrointestinal bleeding, severe anemia, and abdominal lymphadenopathy. A comprehensive medical examination revealed multiple ileal ulcers, a consequence attributed to MTX-induced inflammation of the stomach lining, concomitant with reactive lymphadenopathy. This case illustrates the intricate challenges in diagnosing and treating acute anemia due to gastrointestinal bleeding in patients with EORA, further complicated by MTX use. The lessons from this case emphasize the imperative for increased vigilance and diagnostic precision in treating older RA patients, particularly when utilizing medications like MTX that have a high risk of serious side effects.
Case presentation
A 72-year-old woman presented at a rural community hospital with the primary symptom of hematochezia. The day before admission, she experienced nausea and abdominal bloating. On the morning of admission day, she had multiple episodes of hematochezia. She reported no chest, abdominal, or back pain, or diarrhea. There were no sick contacts or people with similar symptoms around her. She had no recent travel or unusual dietary history that might suggest infection. Her medical history included four years of EORA. She was on 16 mg/week of MTX and 5 mg/week of foliate. An upper endoscopy and fecal occult blood test performed three years prior showed no abnormalities.
At the time of the visit, her vital signs were as follows: blood pressure 157/88 mmHg, pulse rate 95 beats/min, body temperature 36.8 °C, respiratory rate 21 breaths/min, and oxygen saturation 98% on room air. She was oriented to time, place, and person. The physical examination revealed pale conjunctiva without jaundice and mild abdominal tenderness without rebound or percussion tenderness. No other neurological abnormalities, chest irregularities, or skin eruptions were observed. Laboratory tests indicated severe anemia but no signs of inflammation, as her hemoglobin level two months ago was 14.5 g/dL (Table 1).
Abdominal CT with contrast showed local lymphadenopathy around the stomach without extravasation in the gastric mucosa and without continual bleeding (Figure 1).
Abdominal computed tomography with contrast clarifying local lymphadenopathy around the stomach without any extravasation on the stomach's mucus (white arrows).
An urgent lower gastrointestinal endoscopy identified multiple ulcers on the mucosa of the ileum (Figure 2).
Lower gastrointestinal endoscopy clarifying multiple ulcers on the mucosa of the ileum.
Subsequently, an urgent upper gastroduodenal endoscopy revealed no bleeding. Based on these findings, the patient was diagnosed with MTX-induced ileal ulcer and suspected MTX-induced lymphoma. Additional tests showed normal lactate dehydrogenase and soluble interleukin-2 receptors. Biopsies from the stomach, duodenum, ileum, and colon mucosa revealed no malignancy indicative of lymphoma. The patient was treated with oral vonoprazan (20 mg) and rebamipide (300 mg) per day, and MTX was discontinued. One week later, her anemia improved to a hemoglobin level of 10 g/dL, and she experienced no nausea or vomiting. She was discharged with a full return to daily activities and continued follow-up in the outpatient department without anemia recurrence.
Discussion
This case report details a unique presentation of severe anemia resulting from MTX-related damage to the ileal mucosa, accompanied by lymphadenopathy. While gastrointestinal complications are commonly associated with MTX treatment, instances leading to critical conditions are rare. Given the frequent use of MTX in RA management, it is crucial for clinicians to thoroughly investigate progressive anemia in RA patients, considering potential MTX-related complications affecting the gastrointestinal mucosa.
The diverse nature of MTX complications necessitates that physicians, particularly in rural areas, meticulously monitor their patients on MTX for signs of progressive anemia [8,9]. In this case, a 72-year-old female diagnosed with EORA exhibited hematochezia, notably without pain, diarrhea, or known infectious contacts, highlighting the need for increased attention to atypical symptom presentations. This case emphasizes the importance of comprehensive evaluation in RA patients receiving MTX treatment, especially when they present with non-specific symptoms such as nausea and vomiting. Patients with RA on MTX therapy may experience mild anemia due to suboptimal disease control or disease flares [10,11]. It is essential to distinguish between anemia caused by chronic inflammation and that resulting from gastrointestinal bleeding. The absence of inflammatory indicators, such as elevated CRP, as demonstrated in this case, indicates the necessity for further investigation into potential causes of gastrointestinal bleeding [12].
The approach to investigating anemia in MTX-treated patients should be thorough. This case revealed severe anemia, a surprising finding given the lack of significant pain or discomfort typically associated with EORA. A diagnostic approach combining both imaging and endoscopy was instrumental in determining the extent of gastrointestinal involvement [13]. The lack of active bleeding observed during endoscopy, alongside the discovery of multiple ulcers in the ileal mucosa, pointed to progressive mucosal damage rather than acute gastrointestinal bleeding [14,15]. The absence of previous anemia episodes and normal findings from earlier upper and lower endoscopies had delayed more immediate gastroduodenal exploration. Additionally, MTX can cause an increase in the mean corpuscular volume (MCV) of red blood cells [16]. Detecting changes in MCV is crucial, as iron deficiency anemia from bleeding typically leads to a decrease in MCV [16]. Therefore, evaluating anemia in patients with EORA on MTX should include an assessment of inflammation and regular checks for gastrointestinal tract damage through endoscopy, rather than solely relying on laboratory data.
Another significant aspect of this case is the differential diagnosis of lymphadenopathy in patients on MTX, including MTX-induced lymphoma, a rare but notable long-term complication of MTX therapy that necessitates its discontinuation [17]. This patient's normal lactate dehydrogenase and soluble interleukin-2 receptor levels, combined with the absence of malignancy in mucosal biopsies, excluded lymphoma. The management strategy involved immediate cessation of MTX, providing symptomatic relief and addressing the anemia [18]. The patient's positive response to treatment, including anemia resolution and overall health improvement, further confirms MTX's role in her condition.
Conclusions
This case illuminates several key clinical insights. It underscores the importance of ongoing monitoring and reassessment of patients undergoing long-term MTX therapy, especially when new or escalating gastrointestinal symptoms arise. It also highlights the necessity of considering drug-induced complications in the differential diagnosis of anemia in RA patients. Lastly, it advocates for personalized treatment plans tailored to each patient's specific presentation and therapeutic response.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Elderly-onset rheumatoid arthritis: characteristics and treatment options Medicina (Kaunas) Pavlov-Dolijanovic S Bogojevic M Nozica-Radulovic T Radunovic G Mujovic N 18785920233789359610.3390/medicina 59101878 PMC 10608066 · doi ↗ · pubmed ↗
- 2Rheumatoid arthritis Lancet Smolen JS Aletaha D Mc Innes IB 2023203838820162715643410.1016/S 0140-6736(16)30173-8 · doi ↗ · pubmed ↗
- 3Efficacy of pharmacological treatment in rheumatoid arthritis: a systematic literature research informing the 2019 update of the EULAR recommendations for management of rheumatoid arthritis Ann Rheum Dis Kerschbaumer A Sepriano A Smolen JS 7447597920203203393710.1136/annrheumdis-2019-216656 PMC 7286044 · doi ↗ · pubmed ↗
- 4Overview of methotrexate toxicity: a comprehensive literature review Cureus Hamed KM Dighriri IM Baomar AF 014202210.7759/cureus.29518 PMC 959526136312688 · doi ↗ · pubmed ↗
- 5Influence of methotrexate on gastrointestinal symptoms in patients with rheumatoid arthritis Int J Rheum Dis Asai S Nagai K Takahashi N 2072132220193016827410.1111/1756-185X.13380 · doi ↗ · pubmed ↗
- 6Life-threatening gastrointestinal mucosal necrosis during methotrexate treatment for rheumatoid arthritis Case Rep Gastroenterol Tsukada T Nakano T Miyata T Sasaki S 470475720132434831910.1159/000356817 PMC 3843920 · doi ↗ · pubmed ↗
- 7Gastrointestinal bleeding secondary to use of high-dose methotrexate: a case report J Surg Med Peker A YarkıcıH Akar H 15115322018
- 8Japan College of Rheumatology guideline for the use of methotrexate in patients with rheumatoid arthritis Mod Rheumatol Kameda H Fujii T Nakajima A 31402920192971874610.1080/14397595.2018.1472358 · doi ↗ · pubmed ↗