Precut over a pancreatic stent using the marking method to aid biliary cannulation in a patient with Roux-en-Y reconstruction
Yuichi Takano, Naoki Tamai, Jun Noda, Tetsushi Azami, Fumitaka Niiya, Fumiya Nishimoto, Masatsugu Nagahama

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
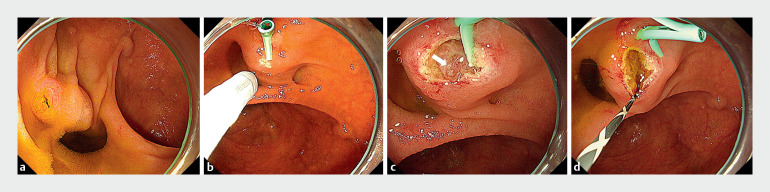 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Esophageal and GI Pathology
Despite the remarkable development of balloon enteroscopy-assisted endoscopic retrograde cholangiopancreatography (ERCP), deep biliary cannulation in patients with surgically altered anatomy remains challenging 1 2 . We report a case where biliary cannulation was successfully achieved via precutting over a pancreatic stent using the marking method 3 .
A 78-year-old man with a history of total gastrectomy and Roux-en-Y reconstruction for gastric cancer visited our hospital with a chief complaint of epigastric pain. He was diagnosed with a common bile duct stone on computed tomography. A single-balloon enteroscope (SIF-H290S; Olympus Medical Systems, Tokyo, Japan) was inserted to reach the naïve papilla of Vater ( Fig. 1 a ). Wire-guided cannulation was attempted, but biliary cannulation was unsuccessful. It was possible to place a guidewire in the pancreatic duct, so a pancreatic guidewire-assisted technique was performed, but biliary cannulation was still impossible. A 5-Fr, 5-cm straight-type pancreatic stent (Geenen Pancreatic Stent Sets; Cook Meical Japan, Tokyo, Japan) was placed. Marking was performed using a needle knife (KD-10Q-1; Olympus Medical Systems) at the bulge of the papilla in the 6 o’clock direction from the pancreatic stent, which was believed to be the direction of the bile duct ( Fig. 1 b ). Fistulotomy was performed by making an incision between the pancreatic stent and the marking point. A red nodule was observed on the incised surface, suspected to be the biliary orifice ( Fig. 1 c ). The catheter was gently applied to the nodule, and deep biliary cannulation was achieved ( Fig. 1 d ). A 7-Fr, 7-cm double-pigtail biliary plastic stent was placed, and the procedure was completed without any adverse events ( Video 1 ). Endoscopic stone extraction was performed 5 days later.
Endoscopic images showing: a the naïve papilla of Vater, which was reached with a single-balloon enteroscope; b a marking made using a needle knife at the bulge of the papilla in the 6 o’clock direction from the pancreatic stent, which was believed to be the direction of the bile duct; c a red nodule on the incised surface, suspected to be the biliary orifice (arrow), that was observed after fistulotomy had been performed by making an incision between the pancreatic stent and the marking point; d successful deep biliary cannulation after a catheter had been gently applied to the nodule.
Precutting is performed over a pancreatic stent using the marking method to aid biliary cannulation in a patient with Roux-en-Y reconstruction.Video 1
In patients with surgically altered anatomy, the papilla is upside down, making it difficult to recognize the direction of the bile duct 4 . Precutting in such patients requires a high degree of skill but, using the marking method, safe and reliable precutting can be performed.
Endoscopy_UCTN_Code_TTT_1AP_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Testoni PA Mariani A Aabakken L Papillary cannulation and sphincterotomy techniques at ERCP: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline Endoscopy 20164865768310.1055/s-0042-10864127299638 · doi ↗ · pubmed ↗
- 2Ishii K Itoi T Tonozuka R Balloon enteroscopy-assisted ERCP in patients with Roux-en-Y gastrectomy and intact papillae (with videos)Gastrointest Endosc 20168337738626234697 10.1016/j.gie.2015.06.020 · doi ↗ · pubmed ↗
- 3Nagai K Katanuma A Takahashi KA simple and novel marking method for correctly identifying the precutting direction to achieve safe and efficacious precut sphincterotomy (with video)Endosc Int Open 20197 E 3E 830648133 10.1055/a-0752-9755 PMC 6327752 · doi ↗ · pubmed ↗
- 4Tanisaka Y Mizuide M Fujita A Usefulness of a novel sphincterotome for transpancreatic biliary sphincterotomy to achieve selective biliary cannulation in patients with Roux-en-Y gastrectomy Endoscopy 202355 E 651E 65337084777 10.1055/a-2063-3521 PMC 10121321 · doi ↗ · pubmed ↗