Cold snaring biopsies to increase screening efficacy during endoscopic surveillance of patients at high risk of diffuse gastric cancer
Marie Lemoine Laroussinie, Mathieu Pioche, Laura Calavas, Tanguy Fenouil, Jean-Christophe Saurin, Arnaud Pasquer, Nicolas Benech

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
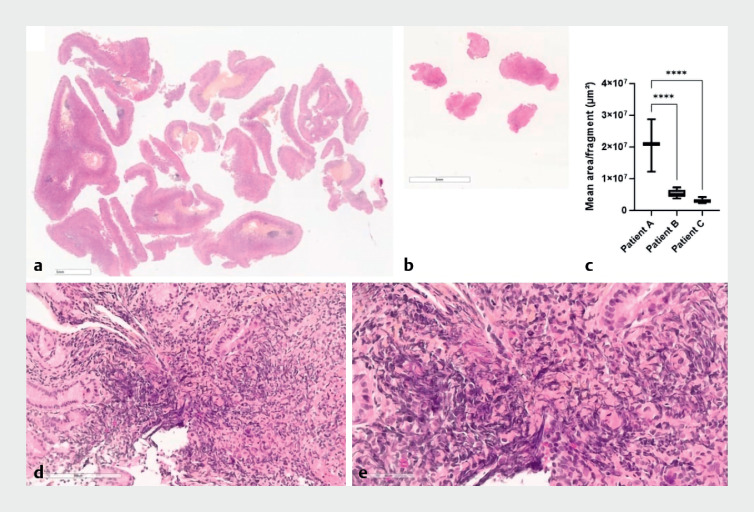 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHelicobacter pylori-related gastroenterology studies · Gastric Cancer Management and Outcomes · Wnt/β-catenin signaling in development and cancer
Diffuse gastric cancer (DGC) is a poorly differentiated adenocarcinoma of the stomach characterized by independent “signet-ring” cells that invade the gastric wall with mainly submucosal infiltration resulting in delayed diagnosis 1 . Mutations in the CDH1 gene, encoding E-cadherin, have been identified in families with multiple cases of gastric cancer, with a 50%–80% increased risk of DGC in carriers 2 . In cases with a proven constitutional CDH1 mutation, guidelines recommend prophylactic total gastrectomy between the ages of 20 and 30 years, or endoscopic surveillance if surgery is refused or postponed 3 .
Given the multiple possible localizations and frequency of small carcinomatous foci, a minimum of 30 biopsies divided into six zones using standard forceps is recommended 3 4 . However, multiple sampling of the gastric mucosa using conventional biopsy forceps still represents a limited surface area that can be analyzed. Increasing the size of the biopsy sample using cold snaring may increase diagnostic sensitivity.
We report here the case of a 33-year-old patient with regular endoscopic surveillance after identification of a CDH1 mutation in a familial context.
Gastroscopy and endoscopic ultrasound were performed, with no findings of macroscopic abnormalities, parietal thickening, or suspicious adenopathy ( Video 1 ). To increase the size of the tissue sampled for histological analysis, 24 cold snaring biopsies (6 upper fundus, 6 body, 6 lower body, and 6 antrum) were performed. Pathological analysis revealed a single focal area of independent cell adenocarcinoma in the chorion (pTis) seen only in one sample. A gastrectomy was then performed, with a millimetric focal adenocarcinoma with signet-ring cells on the surgical specimens.
Gastric sampling using random cold snaring of the whole stomach with visualization of the corresponding resected area.Video 1
Histopathological analysis was improved, with the average size of biopsy fragments being significantly larger with cold snaring than with standard forceps, and with a reduction in crush artifacts ( Fig. 1 ).
Histopathological characterization (hematoxylin and eosin) of specimens from patients followed endoscopically due to familial predisposition for CDH1 mutation-related gastric adenocarcinoma. a Cold snaring biopsy. b Standard forceps biopsy. c The mean size of biopsy fragment was significantly increased with cold snaring (patient A) compared with standard forceps (patients B and C), based on the examination of three patients with 18, 30, and 28 fragments biopsied, respectively (one-way analysis of variance with Dunnett’s multiple comparisons, **** P < 0.0001; GraphPad Prism v10.0.0). d Cold snaring sample: the crushing artifacts often observed with standard forceps were not seen in the cold snaring biopsies (×20 magnification; e ×40 magnification).
In conclusion, this case suggests that large samples obtained with cold snaring could potentially decrease the focal adenocarcinoma miss rate in CDH1 mutation carriers.
Endoscopy_UCTN_Code_TTT_1AO_2AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ikoma N Agnes A Chen H-C Linitis plastica: a distinct type of gastric cancer J Gastrointest Surg 2020241018102510.1007/s 11605-019-04422-731754987 · doi ↗ · pubmed ↗
- 2Hansford S Kaurah P Li-Chang H Hereditary diffuse gastric cancer syndrome: CDH 1 mutations and beyond JAMA Oncol 20151233210.1001/jamaoncol.2014.16826182300 · doi ↗ · pubmed ↗
- 3Fitzgerald RC Hardwick R Huntsman D Hereditary diffuse gastric cancer: updated consensus guidelines for clinical management and directions for future research J Med Genet 20104743644410.1136/jmg.2009.07423720591882 PMC 2991043 · doi ↗ · pubmed ↗
- 4van der Post RS Vogelaar IP Carneiro F Hereditary diffuse gastric cancer: updated clinical guidelines with an emphasis on germline CDH 1 mutation carriers J Med Genet 20155236137425979631 10.1136/jmedgenet-2015-103094 PMC 4453626 · doi ↗ · pubmed ↗