A diagnostic odyssey of herpes zoster mimicking pacemaker pocket infection
Kostopoulou Anna, Cheilas Vasileios, Martinos Antonios, Michalis Efremidis

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
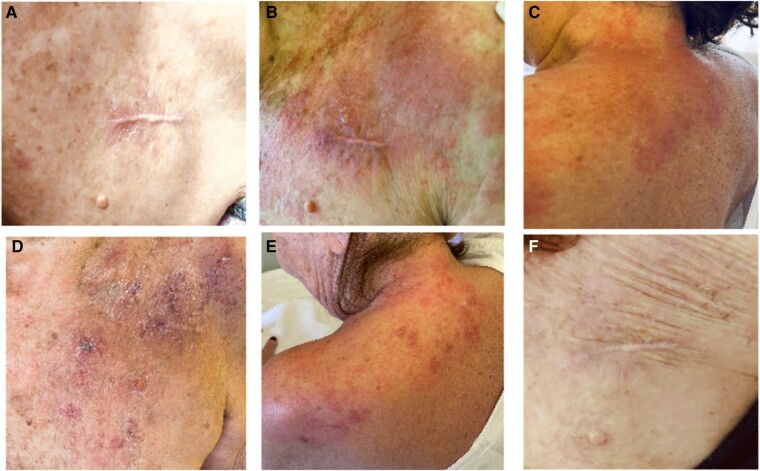 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHerpesvirus Infections and Treatments · Cytomegalovirus and herpesvirus research · Bartonella species infections research
A 73-year-old post-transcather aortic valve implantantion and pacemaker-implanted woman presented with localized redness and pain in the pacemaker pocket region (Figure 1A). Due to initial concerns of an isolated pocket infection, empirical vancomycin administration was initiated after obtaining blood cultures.^1^ Despite the general recommendation of a 2–3-day washout period in stable patients to enhance the precision of microbiological diagnosis, we opted for an earlier initiation in consideration of the patient’s frailty and the presence of a prosthetic valve. This decision was tailored to the specific circumstances of the patient to mitigate the risk of further complications. A transthoracic echocardiogram was conducted to identify lead vegetations and assess valvular involvement. Additionally, a transoesophageal echocardiogram was initially scheduled, but the characteristic progression of the skin lesion prompted a reconsideration of this decision since during the next 2 days, a pale multiforme erythematous lesion with vesicles (Figure 1B and C) unfolded, unmasking the herpes zoster antagonist.^2^ In this point, is worth mentioning, that the patient did not have any history of herpes zoster before. Intravenous acyclovir precipitated rapid improvement within a week (Figure 1D and E), while lingering pain and sensitivity persisted for over a month despite complete erythema healing in two weeks (Figure 1F).^3^ This case highlights the need for identification of distinctive features of rashes suggestive of a pocket infection, consideration for tailored antibiotic initiation, the contemplation of withholding antibiotics in stable patients with concurrent presumed pacemaker pocket infection and confirmed zoster inflammation, and strict adherence to established guidelines for herpes zoster vaccination to prevent similar clinical complexities.
Consent: The authors affirm obtaining written consent from the patient for the submission and publication of this case report, inclusive of images, adhering to COPE guidelines.
Funding: This work received no external financial support. The authors conducted this investigation independently, driven by their commitment to advancing medical knowledge.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Blomström-Lundqvist C , Traykov V, Erba PA, Burri H, Nielsen JC, Bongiorni MG, et al European Heart Rhythm Association (EHRA) international consensus document on how to prevent, diagnose, and treat cardiac implantable electronic device infections-endorsed by the Heart Rhythm Society (HRS), the Asia Pacific Heart Rhythm Society (APHRS), the Latin American Heart Rhythm Society (LAHRS), International Society for Cardiovascular Infectious Diseases (ISCVID) and the European Society of Clinical Microbiolog · doi ↗ · pubmed ↗
- 2Korantzopoulos P , Plakoutsi S, Florou E, Bechlioulis A. Skin lesions over the pocket area that may mimic cardiac implantable electronic device infection: a case series. Pacing Clin Electrophysiol 2018;41:897–901.29785752 10.1111/pace.13378 · doi ↗ · pubmed ↗
- 3Patil A , Goldust M, Wollina U. Herpes zoster: a review of clinical manifestations and management. Viruses 2022;14:192.35215786 10.3390/v 14020192 PMC 8876683 · doi ↗ · pubmed ↗