Ossifying renal tumor of infancy: A case report
Saad Andaloussi, Omar Dalero, Aziz Elmadi

TL;DR
This paper presents a rare case of a benign kidney tumor in an infant with unusual symptoms.
Contribution
The paper adds a new case report of Ossifying Renal Tumor of Infancy with an unusual clinical presentation.
Findings
ORTI is a rare and benign renal neoplasm often presenting with painless hematuria.
Diagnostic imaging techniques like ultrasound and MRI are effective for evaluation.
The etiology of ORTI remains unclear despite diagnostic advances.
Abstract
Ossifying Renal Tumor of Infancy (ORTI) represents an extremely rare and benign renal neoplasm, with limited cases published in the literature. Predominantly characterized by painless and intermittent gross hematuria, the diagnostic evaluation is effectively facilitated through ultrasound, computed tomography, and magnetic resonance imaging. Despite progress, its etiology has not yet been elucidated. We report an additional case with an unusual clinical presentation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1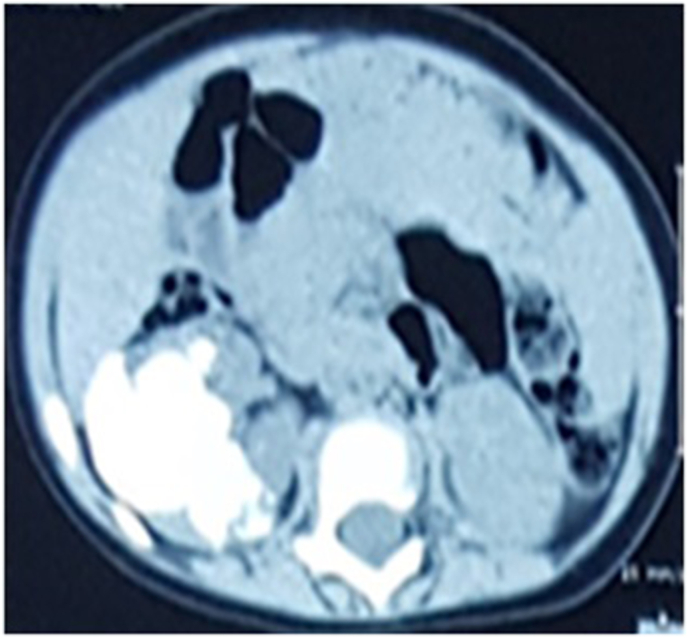 Figure 2
Figure 2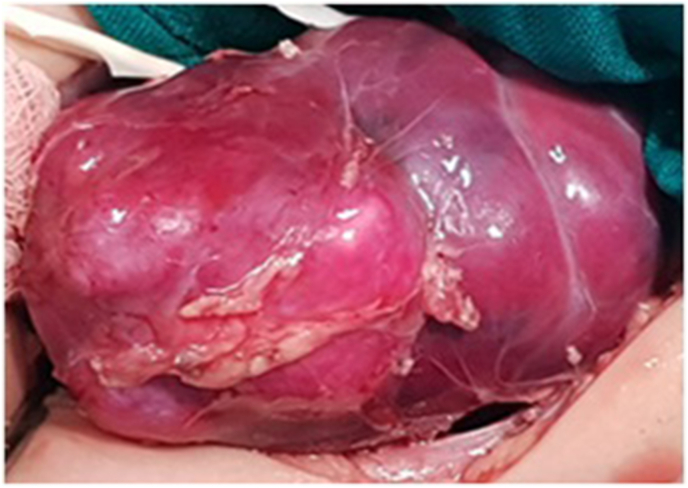 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsRenal and related cancers · Medical Imaging and Pathology Studies · Renal cell carcinoma treatment
Introduction
1
Ossifying Renal Tumor of Infancy (ORTI) is an extremely rare benign renal tumor with limited cases documented to date. It was initially described by Chatten et al., in 1980. Typically affecting male infants, ORTI manifests with intermittent episodes of painless gross hematuria. Occasionally, an abdominal mass may be present; however, arterial hypertension has not been reported in the literature. The radiologic appearance of ORTI may potentially lead to confusion with renal calculus disease or a calcified Wilms tumor. Recognition of ORTI is crucial because neither chemotherapy nor radiotherapy is deemed necessary for its management. Surgical excision is curative, and recurrence or malignant transformation have not been documented.
Case presentation
2
We describe a case of an 8-month-old boy who referred to our hospital with painless intermittent gross hematuria since the age of 2 months. The parents denied any history of fever or trauma. The child didn't show any other clinical symptoms and no associated anomalies were seen. He had no signs of a urinary tract infection. The physical examination was unremarkable except for arterial hypertension; the blood pressure was 128/70. The patient's abdomen was soft, not distended, without a palpable mass or tenderness to palpation. Urinalysis results showed numerous red blood cells per high-power field. Neither bacteria nor nitrites were found. Renal function and electrolyte examinations returned normal results. Plain radiograph revealed flecks of calcifications in the expected area of the right kidney (Fig. 1). Ultrasonography examination showed a solid calcified mass in the upper pole and central part of the right kidney with no distortion of the renal contour. No obvious hydronephrosis or ureter dilatation was seen and no abnormalities were identified in the other kidney. Non-contrast computed tomography revealed a 45 mm benign looking renal mass, calcified, located in the upper pole and central part of the right kidney with no tissue portion visible (Fig. 2). No other associated anomalies were identified. Initially, a partial nephrectomy was considered via an open transabdominal approach; however, the persistence of arterial hypertension, despite the total resection of the tumor, prompted us to complete with a radical nephrectomy of the right kidney. Intraoperatively, no obvious macroscopic extension of the tumor was identified and the procedure was conducted without complication (Fig. 3). The patient had an uncomplicated hospital stay and was discharged on the fifth postoperative day. Pathology analysis subsequently confirmed the diagnosis of ORTI. At his 4-year follow-up, the patient was clinically well without hematuria or arterial hypertension, and repeated abdominal ultrasounds showed no signs of recurrence on the ipsilateral or contralateral sides.Fig. 1. Plain radiograph shows flecks of calcifications in the expected area of the right kidney.Fig. 1. Fig. 2Axial nonenhanced CT image shows a calcified renal mass located in the upper pole and central part of the right kidney with no tissue portion visible.Fig. 2. Fig. 3Resected specimen revealed an ossifying-like appearance that occupied the right kidney.Fig. 3
Discussion
3
ORTI represents an exceedingly rare and benign renal tumor typically observed in early infancy. It was initially described as a distinct variant of pediatric renal tumors by Chatten in 1980.1 To our knowledge, only 30 cases of ORTI have been reported in the literature.2 Concerning its pathogenesis, some publications suggest that it may arise from the epithelium of the urinary tract rather than the renal parenchyma, others believe that it is a subtype of congenital mesoblastic nephroma while no cases of associated Wilms tumor have been reported.3 Microscopically, the tumor presents three major histologic components: osteoblast-like cells within and at the periphery of the core, spindle cells, and an osteoid core. The proportion of these components varies, but the proportion of osteoid and degree of osseous maturation augment with increasing age of the patient. Compared to the usual renal tumors found in infancy, the histological features of our case are distinctive. This ossifying tumor does not display the triphasic pattern characteristic of a typical nephroblastoma, which consists of stroma, blastema, and epithelium. In addition, clonal trisomy 4 has been identified as a cytogenetic feature of ORTI, distinguishing it from Wilms tumor with calcification.4 No case presented malignant transformation or recurrence of the tumor.
Clinically, ORTI generally occurs during early childhood, most often in male patients less than 1 year old. Painless intermittent gross hematuria is the most common symptom. Although less common, an abdominal mass may also be present. No patient presented with arterial hypertension, a distinction observed in our case. Associated hypertension is related to an increase in renin activity caused by secretion from entrapped juxtaglomerular cells. In imaging studies, a plain abdominal radiograph serves to confirm calcification within this region. Ultrasound typically reveals an echogenic mass with shadowing. Computed tomography and magnetic resonance imaging with contrast can be useful in the differential diagnosis of ORTI. Calculi are very rare in infants, even with metabolic disease associated with crystalluria. The primary radiological differential diagnosis is Wilms tumor versus ORTI. It is important to recognize this distinct tumor because no chemotherapy or radiotherapy is necessary. Treatment is based on complete resection of the mass with preservation of the renal parenchyma through an open transabdominal approach. A safe laparoscopic nephrectomy in children with ORTI has been reported.5 However, in specific cases, a radical nephrectomy may be considered necessary such as observed in our patient due to the persistence of arterial hypertension. Subsequently, a prolonged follow-up is imperative to ensure the absence of recurrence.
Conclusion
4
ORTI is an exceptional renal tumor in children. It must be considered in the differential diagnosis in cases of intermittent episodes of painless macroscopic hematuria occurring in the pediatric population, especially when associated with a non-invasive calcified renal mass on radiology. However, this case report recommends a systematic evaluation of arterial hypertension, potentially influencing the therapeutic approach.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Informed consent
Patient's attendant (father) provided informed consent prior to study participation.
Declarations of interest
None.
CRediT authorship contribution statement
Saad Andaloussi: Writing – review & editing, Writing – original draft, Validation, Conceptualization. Omar Dalero: Visualization. Aziz Elmadi: Validation, Supervision.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chatten J.Cromie W.J.Duckett J.W.Ossifying tumor of infantile kidney report of two cases Cancer 45198060961210.1002/1097-0142(19800201)45:3<609::AID-CNCR 2820450330>3.0.CO;2-06243512 · doi ↗ · pubmed ↗
- 2Banerjee A.Reddy K.A.Munghate G.Bodhanwala M.Bendre P.S.Ossifying renal tumor of infancy-a case report J Pediatr Surg Case Rep 93202310265010.1016/j.epsc.2023.102650 · doi ↗
- 3Lowe L.H.Isuani B.H.Heller R.M.Pediatric renal masses: Wilms tumor and beyond Radiographics 2020001585160310.1148/radiographics.20.6.g 00nv 05158511112813 · doi ↗ · pubmed ↗
- 4Liu J.Guzman M.A.Pawel B.R.Clonal trisomy 4 cells detected in the ossifying renal tumor of infancy: study of 3 cases Mod Pathol 26201327528110.1038/modpathol.2012.12022976287 · doi ↗ · pubmed ↗
- 5Hajiran A.Jessop M.Werner Z.Ossifying renal tumor of infancy: laparoscopic treatment and literature review Case Rep Urol 201820181510.1155/2018/1935657 PMC 621874430425880 · doi ↗ · pubmed ↗