A case of late-onset bleeding from an intercostal artery pseudoaneurysm after hemostasis using soft coagulation
Rie Shimizu, Kenichi Suda, Toshiki Takemoto, Shota Fukuda, Masato Chiba, Masaki Shimoji, Junichi Soh, Tetsuya Mitsudomi, Yasuhiro Tsutani

TL;DR
A patient developed late-onset bleeding from an intercostal artery pseudoaneurysm after hemostasis using soft coagulation during thoracic surgery.
Contribution
This case highlights the potential risk of pseudoaneurysm formation with soft coagulation and suggests additional hemostasis measures may be needed.
Findings
Late-onset bleeding occurred from a pseudoaneurysm after soft coagulation hemostasis.
Tissue carbonization observed during surgery may indicate incomplete hemostasis.
Embolization was required to stop the bleeding after contrast-enhanced CT diagnosis.
Abstract
The use of soft coagulation is becoming common in thoracic surgery. Soft coagulation provides rapid hemostasis from small vessels during surgery by dehydrating tissue and denaturing proteins, without burning the tissue. A 68-year-old man, with a history of right lower lobectomy 3 years prior, underwent a partial resection of the right upper lobe for a pulmonary nodule suspicious for secondary lung cancer. During the surgery, dissection of the adhesion caused a bleeding from the 6th intercostal artery, and hemostasis was achieved using soft coagulation (some degree of tissue carbonization was noticed at later mortality and morbidity conference). He experienced hemoptysis at postoperative day 18 and was transferred to our hospital. Contrast-enhanced CT scan revealed bleeding from the pseudoaneurysm of the 6th intercostal artery. Embolization was performed by angiography to stop the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
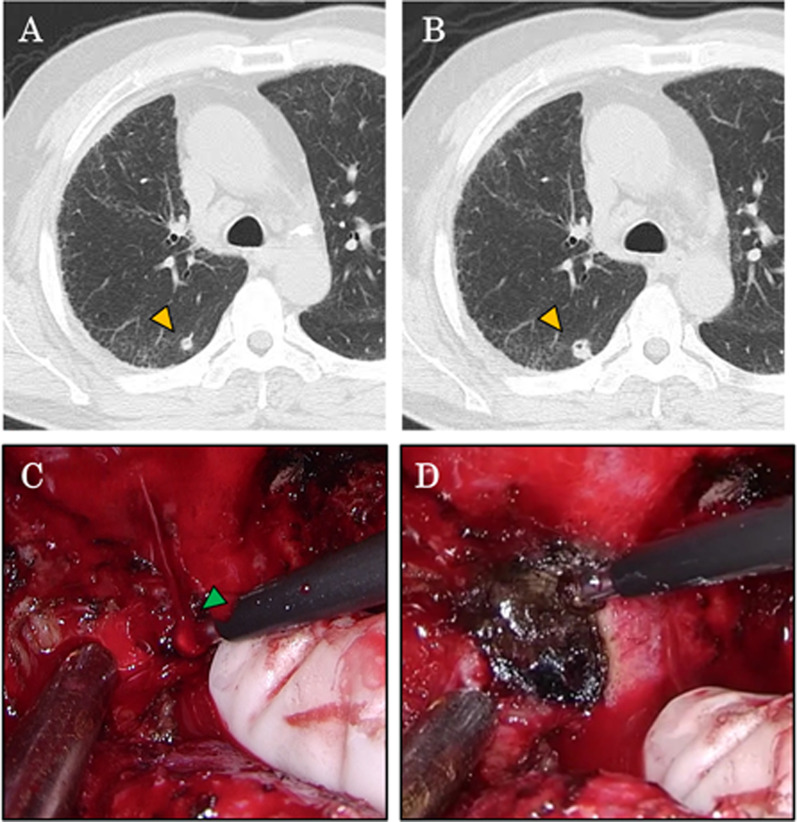 Figure 1
Figure 1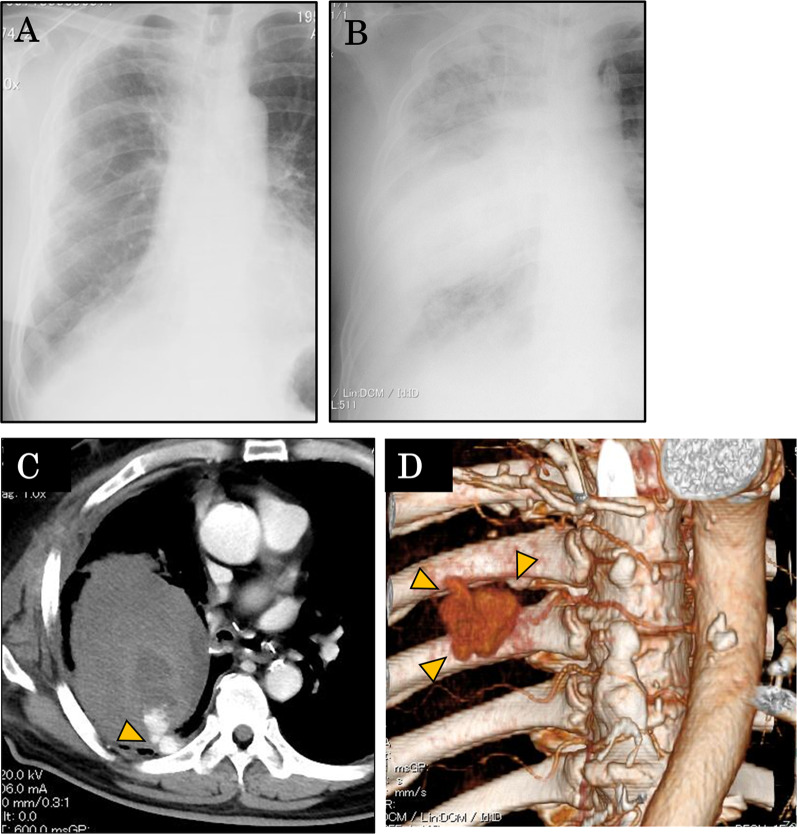 Figure 2
Figure 2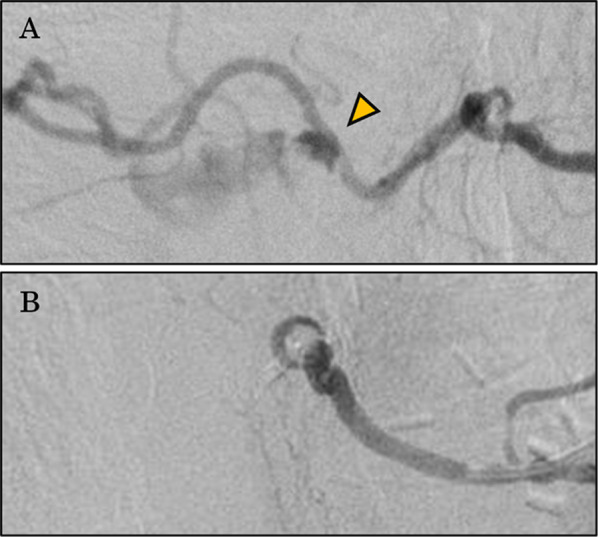 Figure 3
Figure 3- —http://dx.doi.org/10.13039/501100001691Japan Society for the Promotion of Science
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Anomalies and Treatments · Tracheal and airway disorders · Trauma Management and Diagnosis
Background
Lung cancer surgery in Japan is becoming safer as a result of multiple factors, including the development of surgical instruments, improved perioperative management, and the increase of small/peripheral lung nodules [1–3]. However, serious complications may still occur after lung cancer surgery, including postoperative hemorrhage, bronchopleural fistula and pyothorax, and brain strokes, although the frequencies of these events are quite low. Postoperative hemorrhages are usually observed during the early postoperative period, and delayed hemorrhage may occur in some rare cases. The proportion of postoperative hemorrhage cases that require reoperation is approximately 0.6–1.3% [4–6]. Here we report a case of a lung cancer patient with late-onset postoperative hemorrhage (postoperative 18th day) after partial resection of the lung.
Case presentation
A 68-year-old man underwent right lower lobectomy for invasive mucinous adenocarcinoma (pT2aN1M0 Stage IIB) in June 2016 by an open thoracotomy approach. Postoperative follow-up computed tomography (CT) examinations revealed a pure-solid pulmonary nodule in the right upper lobe of his lung (Fig. 1a), which was found to be slightly enlarged on a follow-up CT evaluation (Fig. 1b). In July 2019, a partial pulmonary resection of the right upper lobe was performed. During the surgery, a severe adhesion between the lung and the chest wall was noted, and dissection of the adhesion caused bleeding from the 6th intercostal artery (Fig. 1c). Hemostasis was achieved using soft coagulation (Fig. 1d). Dissection of the adhesion was performed only to the extent necessary to perform the partial resection. The postoperative course was uneventful, and the patient was discharged 5 days after surgery.Fig. 1. The enlarged pulmonary tumor and intraoperative bleeding and hemostasis. A second primary lung cancer identified during postoperative follow-up after right lower lobectomy (December 2018) (a) that enlarged slightly 6 months later (June 2019) (b). Partial resection was planned for the pulmonary nodule. Intraoperative findings showed bleeding from an intercostal artery during the surgery (c) and hemostasis was achieved using soft coagulation (d)
The first postoperative outpatient visit was 18 days after surgery, and blood test and chest X-ray (Fig. 2a) showed no abnormal findings. However, the patient later experienced hemoptysis at the toilet of a convenience store adjacent to the hospital. He was rushed to the hospital by medical staff who were assembled by a stat call. His vital scores were unstable; blood pressure (BP) was 117/98 mmHg, heart rate (HR) was 125 bpm, respiratory rate (RR) was 30 beats/min, and SpO_2_ was 70% (room air). A second chest X-ray on the same day showed decreased permeability in the right middle lung field (Fig. 2b). Contrast-enhanced CT scan of the chest showed a hematoma with a maximum diameter of 11 cm in the right thoracic cavity, a small amount of free air, and leakage of contrast medium into the hematoma from 6th intercostal artery (Fig. 2c). A 3D-reconstruction of the chest CT revealed a pseudoaneurysm of the intercostal artery (Fig. 2d).Fig. 2. Radiological examinations performed on the day of late-onset bleeding (18 days after surgery). Chest X-rays before the bleeding (a) and after the emergency transportation (b) are shown. Contrast-enhanced CT examination revealed bleeding from the intercostal artery (arrowhead) and a large intrathoracic hematoma (c). The 3D reconstruction of the CT revealed a pseudoaneurysm (arrowhead) of the intercostal artery (d)
The patient was immediately admitted to the Radiology Department for emergency angiography. Because his systolic BP was 58 mmHg on admittance, a rapid transfusion of four units of red cell concentrate (RCC) was administered during the preparation for angiography. The angiography through the right femoral artery revealed extravasation from the 6th intercostal artery (Fig. 3a). Therefore, the 6th intercostal artery was embolized using an embolization agent (NBCA:lipiodol = 1:3) to stop the bleeding.Fig. 3. Successful hemostasis by angiographical embolization. Angiography successfully identified the bleeding point (arrowhead) of the intercostal artery (a). Embolization using n-butyl-2-cyanoacrylate plus lipiodol in a 1:3 mixture was performed, and hemostasis was obtained (b)
After the emergency angiography, the patient’s general condition recovered. However, a CT examination performed 2 days later found free air within the hematoma. Because pulmonary fistula was suspected, a chest drain tube (24Fr.) was inserted into the intrathoracic cavity. The air leak disappeared on day 17 after angiography and the patient was discharged on day 22.
Discussion
Here we report a case of late-onset postoperative hemorrhage (postoperative 18th day) after partial resection of the lung. Hemoptysis, the symptom of the hemorrhage, occurred at a convenience store adjacent to the hospital, and medical staffs in our hospital rushed to the store in response to a stat call. It may be questioned whether the stat call was adequate at an out-of-hospital facility, we speculate that the quick transport of the patient might have saved his life as he was in a pre-shock state when he arrived at the angiography room. This may suggest that a rupture of a pseudoaneurysm of the intercostal artery can be a potentially fatal situation.
The primary symptom in this case was hemoptysis. In general, the differential diagnosis of hemoptysis after pulmonary resection includes bleeding from the staple line, pulmonary artery–bronchial fistula [7], and aspergillosis in the remaining cavity in the lung [8]. Because the patient received partial resection and 3 years had passed since he received right lower lobectomy, a pulmonary artery–bronchial fistula was unlikely. Therefore, a contrast-enhanced CT scan was immediately performed to investigate the bleeding point. We concluded that hemorrhage from the intercostal artery caused the hematoma, and the increased pressure within the hematoma caused a break of the adhesion between the lung and the chest wall, resulting in lung injury (pulmonary fistula). The patient may have inhaled the blood of the hematoma into the bronchus through the pulmonary fistula, leading to hemoptysis.
Postoperative intercostal artery pseudoaneurysm is a very rare complication. To the best of our knowledge, only two case reports have been reported thus far [9, 10]. Kawai et al. reported a case who experienced pseudoaneurysm of the 7th intercostal artery after video-assisted right lower lobectomy. The authors suspected that the pseudoaneurysm occurred at the site of a surgical port (with the possibility of injury of the intercostal artery during surgery). Intrathoracic hemorrhage was observed at postoperative days 4 and 18, and surgery was performed to control the hemorrhage on the 18th postoperative day [11]. The second case experienced a pseudoaneurysm caused by a biopsy of the parietal pleura (it is also possible that the intercostal artery was injured). In our case, we found that the intercostal artery was injured (Fig. 1C) and we used soft coagulation to stop the bleeding (Fig. 1D).
In the use of the coagulation mode of conventional electrocautery, hemostasis is achieved by burning the surface of the tissue. This leads to the formation of carbonized crusts; if the carbonized crusts detach, for example from mechanical stress, this can lead to postoperative bleeding. On the other hand, in soft coagulation, dehydrated dry tissues and denatured proteins are the main mechanisms that contribute to hemostasis; therefore, the risk of postoperative bleeding is lower than the coagulation mode of conventional electrocautery [12]. The soft coagulation used during the surgery (AMCO, Tokyo, Japan) is the one widely used in general, and was used with the standard soft coagulation mode output setting of Valleylab™ FT10 (Medtronic plc, Dublin, Ireland). However, while soft coagulation was used in our patient, intraoperative video recorded some degree of tissue carbonization likely due to the electrode being held in place a little longer than usual (Fig. 1D). We consider this may be one of the reasons for the vulnerability of the artery wall to form a pseudoaneurysm.
Conclusions
Soft coagulation is widely used to control minor bleeding from small vessels during pulmonary resection. Soft coagulation is a useful because it provides rapid hemostasis without carbonizing the tissue. However, our experience in treating the current case indicates that additional hemostasis, such as the ligation at the proximal site of the hemorrhage point, would be considered for small arteries after hemostasis is achieved by soft coagulation, especially when some degree of tissue carbonization is suspected.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Suda K Sato K Mizuuchi H Recent evidence, advances, and current practices in surgical treatment of lung cancer Respir Investig 201452632232910.1016/j.resinv.2014.06.00325453375 · doi ↗ · pubmed ↗
- 2Kaga A Ikeda T Tachibana K An innovative oral management procedure to reduce postoperative complications JTCVS Open 2022161044245310.1016/j.xjon.2022.01.021PMC 939021336004276 · doi ↗ · pubmed ↗
- 3Motono N Ishikawa M Iwai S Analysis of risk factors for postoperative complications in non-small cell lung cancer: comparison with the Japanese National Clinical Database risk calculator BMC Surg 202222118010.1186/s 12893-022-01628-635568860 PMC 9107161 · doi ↗ · pubmed ↗
- 4Uramoto H Shimokawa H Tanaka F Postoperative bleeding after surgery in patients with lung cancer Anticancer Res 201434298198424511043 · pubmed ↗
- 5Yano M Numanami H Akiyama T Reoperation for postoperative bleeding following pulmonary resection: a report of a single-center experience Gen Thorac Cardiovasc Surg 20196760861410.1007/s 11748-018-01060-930656590 · doi ↗ · pubmed ↗
- 6Zheng S Ye T Li B Bleeding-related re-exploration following pulmonary resection: a report of a single-center experience J Cancer Res Clin Oncol 20231496841684810.1007/s 00432-023-04591-836808301 PMC 11796579 · doi ↗ · pubmed ↗
- 7Hinderberger P Fliss B Thali JM Intercostal artery pseudoaneurysm after thoracoscopic lung resection Gen Thorac Cardiovasc Surg 20095755055310.1007/s 11748-008-0369-x 19830520 · doi ↗ · pubmed ↗
- 8Jiang C Dai J Bao Y Surgical treatment of pulmonary aspergilloma: a 13-year experience from a single clinical center Ann Thorac Surg 2022114131131810.1016/j.athoracsur.2021.06.07434343475 · doi ↗ · pubmed ↗