Empowering Pacific Patients on the Weight Loss Surgery Pathway: A Co-designed Evaluation Study
Tamasin Ariana Taylor, Grant Beban, Elaine Yi, Michael Veukiso, Genevieve Sang-Yum, Ofa Dewes, Wendy Wrapson, Nalei Taufa, Andrew R. T. Campbell, Richard J. Siegert, Peter Shepherd

TL;DR
A culturally tailored pre-surgery program for Pacific patients in New Zealand improved retention and satisfaction in weight loss surgery pathways.
Contribution
The study introduces a co-designed, culturally anchored preoperative program that increases retention and completion rates for Pacific patients.
Findings
Nine out of 14 participants attended all preoperative sessions.
Six participants underwent weight loss surgery after completing the program.
Cultural safety, accessibility, and group support were key to program success.
Abstract
Despite having the highest medical needs by population for weight loss treatment, Pacific patients in Aotearoa New Zealand face substantial levels of attrition in publicly funded weight loss surgery programs. In collaboration with the Auckland City Hospital bariatric surgery team, a Pacific-led preoperative weight loss surgery program was co-designed, delivered, and evaluated between 2020 and 2023. This was a single-arm, prospective co-designed evaluation study that took place at Auckland City Hospital in Aotearoa New Zealand. Participants were Pacific patients (n = 14) referred to the weight loss surgery program. Survey and video diaries were analyzed to determine if the program had the potential to increase Pacific patient retention through the preoperative stage of weight loss surgery, increase surgery completion rates, and improve the quality of treatment experiences. Nine out of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
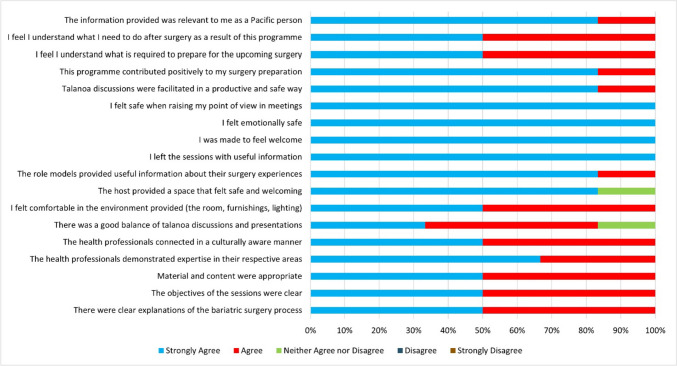 Figure 1
Figure 1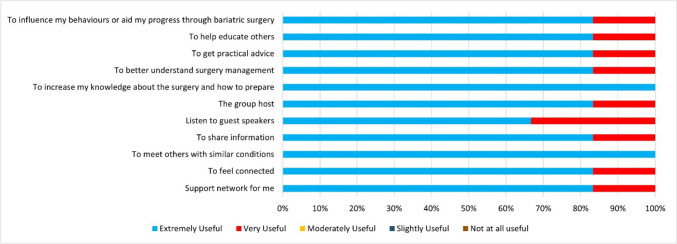 Figure 2
Figure 2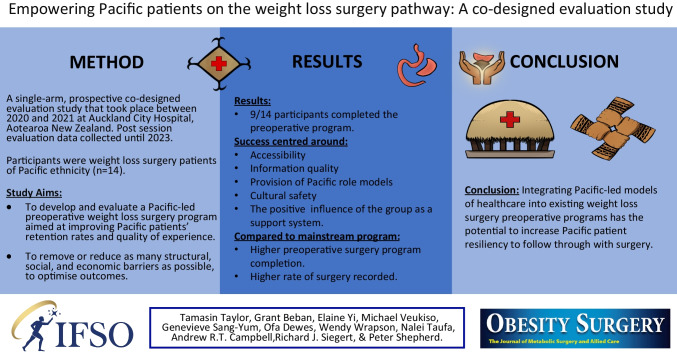 Figure 3
Figure 3- —University of Auckland
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBariatric Surgery and Outcomes · Obesity and Health Practices · Enhanced Recovery After Surgery
Introduction
Weight loss surgery is one of the most effective long-term treatments for obesity-related co-morbidities [1–3], outperforming lifestyle treatments (e.g., diet and exercise) [4] and anti-obesity medications [5]. A reported 84% of patients with type 2 diabetes experience complete remission after weight loss surgery, and conditions such as sleep apnoea, hyperlipidaemia, and hypertension are resolved or significantly improved [6, 7].
Pacific populations in Aotearoa New Zealand (NZ), have the highest prevalence of obesity and obesity-related co-morbidities of all ethnic groups. They are 2.3 times more likely to be obese, three times more likely to have diabetes, and four times more likely to have kidney failure than non-Pacific people [8]. Despite having the greatest need for obesity treatment, Pacific populations have the lowest engagement and completion rates for publicly funded weight loss surgery. The number of eligible Pacific patients receiving publicly funded weight loss surgery in NZ shows a substantial disparity, with 0.7 surgeries undertaken per 1000 for Pacific ethnicities, compared with 3.0 for NZ Europeans [9]. A later study calculated that eligible Pacific people received approximately half the rate of publicly funded surgeries as European and Māori each year over the 2013–2017 period [10].
Once referred to a weight loss surgery program, Pacific patients moving through the preoperative stage are highly vulnerable to attrition. During the preoperative stage of surgery, patients must attend specialist appointments (e.g., with the surgeon or dietitian) and group support sessions normally located within the hospital. Patients need to demonstrate eating and exercise patterns relevant to preparing for the upcoming surgery. Lifestyle improvements facilitate more effective treatment outcomes through higher post-surgical weight loss, nutritional management, and long-term weight loss maintenance. If a patient cannot attend all appointments and group education sessions and demonstrate they have made sufficient lifestyle changes before surgery, they are discharged from the pre-surgery program and referred to their GP or specialist. In one major program located at Auckland City Hospital (NZ) between 2007 and 2016, 73% of Pacific patients referred for weight loss surgery dropped out before surgery took place, and for Pacific males, the attrition rate was 87% [11]. Another study at Counties Manukau, Auckland, NZ, found that only 28% of Pacific patients underwent surgery after being accepted into the surgery program compared to 63% of NZ European patients [12].
The authors’ previous work has identified the challenges facing patients of Pacific ethnicity at the preoperative surgery stage. Twenty-one health sector professionals who worked directly with Pacific patients (surgeons, dietitians, nurses, GPs, psychologists) or in wrap-around services (community health workers, public health physicians) were interviewed to explore factors contributing to Pacific patients’ disproportionately high preoperative attrition rates [13]. Following this, 15 former weight loss surgery patients of Pacific ethnicity who had entered weight loss surgery programs at two hospitals in the wider Auckland region were interviewed [14]. The themes arising from these interviews were used to develop a Pacific-led preoperative weight loss surgery program by targeting the barriers to program completion (see Table 1 for changes to the mainstream program). Table 1. Details of the differences between the mainstream preoperative program and the Pacific-led programStandard support programPacific-led support programPurpose of changePatient recruitment to the program Patients identified as eligible by the ACH bariatric surgery team are sent a letter inviting them to attend an information session held at the hospital, usually at 2 pm on a weekday If patients decide to participate in the weight loss surgery program after attending that information session, they begin the standard group support sessionsThe ACH bariatric team identifies eligible patients of Pacific descent and seeks their consent for the project team to contact them. If consent is granted, the principal investigator (PI) phones the patients and explains the purpose of the Pacific-led support program. Patients are invited to attend the initial information session, which is held on a Saturday afternoon, followed by the other Pacific-led group support sessions over the following monthsBy phoning patients individually, and introducing herself and the program, the PI aims to establish a positive and trusting relationship with the patient at the outset of the programTogether the patient and PI can work through potential barriers, such as transport, session times, and social support needsLocation and timing of sessions Group support sessions are held in a clinical centre during normal working hoursGroup support sessions are held in a community centre in a private room on a Saturday afternoonThis aims to reduce barriers associated with fear of hospitals, shyness about needing weight loss surgery, and difficulties around parking and transportArrangement and conduct of sessions Patients sit in rows in a conference room. The surgeon or other bariatric team member talks to the group about what the surgery involves and the changes patients need to make. Questions are invited at the endSessions follow a Pacific protocol with:• Seats arranged in a semi-circle• Opening and closing prayers• Introductions around the group• Presentation by a health professional (e.g., surgeon or bariatric nurse)• Talanoa and closing remarks• Light refreshmentsThis aims to create a culturally safe environment and to build trust and mutual respect between the health professionals and patientsPacific role models Role models are not currently employed in the standard support program. However, patients can contact the bariatric nurse by mobile phone if they have any concernsThe various Pacific weight loss surgery role models attend all sessions alongside the health professional and facilitator. In the first session, two role models (one female, one male) relate their weight loss surgery journey. A video clip of one of the role models’ journey is played. Patients can ask the role model questions during sessions or at a later date via SMS, telephone, or emailThe need for role models of Pacific ethnicity was a key improvement to the standard program suggested by Pacific patients interviewed in the PI’s previous interview studyBeing able to talk about the surgery journey with others who have successfully completed surgery helps build patients’ confidence and overcome their fears and concerns. Emphasizing the benefits of surgery motivates them to stay in the programWorldview of health and illness Sessions focus on the western biomedical model of health, whereby surgery is a means of improving physical health and avoiding an early onset of death. Surgery preparation focuses on improving diet and increasing exerciseSessions reflect a holistic Pacific worldview of health, which includes physical, mental, social, and spiritual wellbeing [15]. Surgery preparation focuses on improving diet and increasing exercise but also on developing skills to cope with stress and difficult social situations in positive waysBy moving away from a Eurocentric, individualistic model of health towards a more holistic Pacific model incorporating the need to be a productive member of one’s family and community, patients’ motivation to go through with surgery is enhancedFrequency of sessions After the initial information session, patients attend three group education sessions, one each run by the clinical nurse specialist, dietitian, and health psychologistAfter the initial information session, patients attend four group support sessions, one each run by the clinical nurse specialist and health psychologist and two run by the dietitiansThe higher number of sessions aims to improve connection with the program and increase the level of support provided to patientsSession facilitation Group education/support sessions are run by mainly NZ European bariatric surgery team members (nurse, dietitian, health psychologist)Group education/support sessions are facilitated by the PI, who is of Pacific heritage. She is assisted by up to two Pacific patient role models per session. It is made clear to everyone at the outset that meetings are confidential and individual information is not to be discussed outside of the meetingsThis aims to increase cultural safety, to encourage patients to feel comfortable and less concerned about being judged. It is emphasized that everyone is part of each other’s weight loss surgery support group or Aiga (family) and that participants are all on a journey togetherFamily involvement Support people are allowed to attend group support sessionsFamily members are encouraged to attend and are involved in discussions. Children can watch a movie and play in an adjoining room. Babies and toddlers can remain with their parentsEncouraging families to attend provides practical support and reduces social stigma. Patients know that, if they choose to, they can bring their family with them on their journeyPractical barriers Patients pay for parking and travel. Sessions are held during normal working hoursPractical barriers are reduced according to each individual’s needs. Parking and petrol costs are reimbursed for those who need them, and sessions are held outside normal working hoursThese initiatives help to reduce practical barriers that patients may face
Study Aims
The primary aims of the current study were:
- To develop and evaluate a Pacific-led preoperative weight loss surgery program based on Pacific health values to improve Pacific patients’ retention rates and quality of experience.
- To optimize outcomes and remove or reduce as many structural, social, and economic barriers as possible.
The focus was on the preoperative stage because this was identified as the point at which Pacific patients are disproportionately vulnerable to disengaging with the program and dropping out. Specific requirements included reducing the time spent in clinical spaces and increasing access to culturally safe spaces when providing support services; minimizing the financial burden arising from childcare, transport, food, and other costs; and employing Pacific role models to support patients and their families.
The secondary aims of this study were:
- To determine whether the Pacific-led preoperative weight loss surgery program had the potential to increase retention for Pacific patients.
- To identify which components of the program positively impacted patient satisfaction.
Method
This single-arm, prospective evaluation study employed quantitative and qualitative methods to analyse survey and video diaries data. The study took place in Auckland, Aotearoa New Zealand, and was limited to patients within the catchment area of the Auckland District Health Board (ADHB) (now part of Te Whatu Ora) who were referred to the Auckland City Hospital (ACH) weight loss surgery program. The study was supported by the ACH bariatric team, who co-designed the program, made initial contact with patients to recruit them into the study, and conducted the preoperative education sessions. The program was also co-designed with two Pacific role models who had previously undergone surgery. From a medical point of view, there was no difference between the two programs: the differences lay in the support structures and services provided.
Differences to the program included the following: the first information and subsequent group education sessions were held in a community space rather than at a clinical centre, and sessions were led by the bariatric team members accompanied by a Pacific facilitator and one or two Pacific role models who had gone through the surgery process previously. The study covered travel and parking costs if participants needed this assistance, and patients were welcome to bring along family members. A key session component was group talanoa, a Pacific form of interaction that “…allows people to engage in social conversation which may lead to critical discussions or knowledge creation that allows rich contextual and inter-related information to surface…” [16]: 2009, p. 24). This enabled in-depth conversation around the surgery process. In addition to the medical preparation for surgery, each session involved discussing some of the stigma, barriers, and enablers of the patients’ surgery process.
The initial information session occurred on 31 October 2020, and the group support sessions ran from 22 May to 10 July 2021. The inclusion criteria were being of Pacific heritage, 18 years or older, and acceptance into the ACH weight loss surgery program. After attending all five sessions, participants completed a post-preoperative session survey. This was designed to measure the extent to which participants found these sessions useful in their preparation for weight loss surgery and to gather qualitative data about their experiences. Participants then followed the normal clinical path to surgery.
Results
Of 20–25 eligible patients invited to the Pacific sessions, 15 expressed an interest in attending the information session, and 12 turned up on the day. Another two subsequently attended a second scaled-down session, resulting in 14 attendees. Nine out of 14 participants attended five education/support sessions, as was required to remain eligible for surgery. Six participants missed one of the community sessions and had to attend one mainstream session to make up for the missed session. Four attended a mainstream health psychology session, and two attended a mainstream dietitian session. Of the 14 participants, seven were born in NZ, and seven were Island-born. The average age was 45 years; 11 identified as female, two as male, and one as transgender. Of the 14 participants, nine identified as having Samoan heritage, four as Cook Island Māori, one as Tongan, one as Niuean, and one as having Tokelauan heritage. The average weight was 148.8 kg, and the average BMI was 53 kg/m^2^ (range 42.4–72.6 kg/m^2^). All participants had one or more co-morbidities, the five most prevalent being obstructive sleep apnoea (n = 10), type 2 diabetes (n = 9), hypertension (n = 7), joint/back pain (n = 5), and dyslipidaemia (n = 4).
Nine out of 14 participants attended all preoperative support sessions. Reasons for five patients dropping out before completion of these sessions included limited understanding of English, mental health issues, the need to look after family members, death of the patient, and no reason given. Six of the nine remaining participants underwent weight loss surgery, two dropped out after the sessions concluded, and one was still in the program. Reasons for dropping out or not proceeding to surgery after the education sessions included change of mind, not attending further pre-surgery appointments, and failure to meet preoperative medical requirements. The retention rate for surgery was 43% (6/14).
Data from the post-preoperative session survey indicated that components of the program that had a positive impact on patient success and satisfaction centred around accessibility, information quality, having Pacific role models, feeling culturally safe, and the effect of the group as a support system. Participants liked the community hall venue and being able to attend sessions outside normal working hours. This compared favourably with the less-welcoming environment of previous clinical spaces they had encountered, with parking and accessibility issues. Participants were happy with the quality and quantity of the information provided during the five group sessions. Feedback indicated that the overall content of the preoperative sessions was consistently positive with a mean score of 4.7/5 across all survey items. All respondents “strongly agreed” with four statements: “I felt safe when raising my point of view in meetings”, “I felt emotionally safe”, “I was made to feel welcome”, and “I left the sessions with useful information”. See Fig. 1 for further details of feedback on the overall content of the information sessions.Fig. 1. Participant feedback on the content of preoperative information sessions
Feedback on the program’s overall usefulness was consistently positive, with a mean score of 4.8/5 (see Fig. 2).Fig. 2. Overall usefulness of the program
Responses to the Open-Ended Questions
Respondents’ comments indicated that the sessions were conducted in a culturally competent manner: “warm, welcoming, acknowledged our Pasifika-ness and values of inclusiveness, aroha, manaakitanga and space”. Some participants felt comfortable asking questions in this environment: “Everything was on point. I felt comfortable in the surroundings to raise my hand if I needed to ask questions”. One participant pointed out that given this was the first prototype of such a program, there would need to be some aspects that would evolve and need to be adjusted: “It’s an evolving process, not the perfect cookie cut, the beginning of many things, and some things may need to be adjusted”. Some participants indicated that the sessions were informationally relevant, and at the same time, there could have been more of a focus on being accountable to yourself. In response to the question, “How hopeful about the surgery process do you feel after attending the group sessions?”, 83% of respondents were “very hopeful”, and the remainder were “somewhat hopeful”. Respondents’ comments highlighted the supportive relationships built among group members during the program. This is reflected in the following comment:The strength of the sessions has been as much about the support and relationships built with our Pacific cohort as it has been about the speakers that came to our meetings. The collegiality, trust and vulnerability. Without the connection to our group... I don’t know if I would have made it through these last 18 months.
Future of Program
When asked whether the Pacific-led program should be made available to patients in the future, all respondents answered in the affirmative. One participant indicated that they felt that Pacific patients should have to opt out of the program rather than opt into it. Another participant recognized that the program would lead to higher success rates for Pacific people. One participant felt the program offered a safe space due to being conducted in a Pacific social context:... No one can walk this journey on their own… It is important that we can have a safe space [where] we can voice our concerns and have like-minded people who are on the same journey support us every step of the way. The Pasifika stream is so vital because our psyche is different. Our social construct is different.
Discussion
The primary aim of this study—to develop and evaluate a Pacific-led preoperative weight loss surgery program aimed at improving retention—was achieved despite the global pandemic and associated lockdowns. After an initial development and recruitment phase, the formal program ran from October 2020 to July 2021, when the last preoperative session was held. From a research viewpoint, the study continued beyond this point, with the deployment of the post-preoperative session survey and the ongoing recording of video diaries. The retention rate was 43%, which is substantially higher than the mainstream program’s retention rate between 2007 and 2016 of 27% [11]. However, this result must be viewed cautiously because the sample size was too small for this increase to be tested for statistical significance. As such, larger studies and a randomized control trial would be needed to support the current findings.
The components contributing to the success of the current program have also been identified in previous studies. A qualitative interview study exploring patient experiences (n = 12) of a bariatric program for managing obesity in Southwest England found that participants felt that the group was a resource for a lifestyle change, there was a sense of self that was based upon their participation in the group, psychological connections to other patients were established, and shared social identity was regarded as a key feature through which the program’s educational material was accessed [17]. Participants’ weight became a “problem” through a collective lens, empowering the initiation of a sustained individual lifestyle change. In the current study, feedback indicates that the collective cohesion of the group was a key factor in supporting participants’ progress.
Additionally, co-designing the program with the surgery team and Pacific role models effectively achieved a culturally anchored format. One recent community-centre diabetes-prevention intervention study co-designed by youth, health providers, and researchers found that co-designing interventions for Pacific populations needed to be culturally tailored to meet the realities of the communities [18]. One of the themes they identified, namely “Building a safe space”, was also achieved in the current study, with participants indicating the importance of journeying with the group and for accountability. Despite not being a formal part of the program, the support group (also known as the Aiga or “bari family”) appears to have played a major role in boosting patient satisfaction and preventing attrition. Having grown out of the preoperative sessions as a face-to-face phenomenon, it moved online during the COVID-19 lockdown and persisted well beyond the completion of the program and the study.
A limitation of the study was that due to resourcing constraints, there were no bariatric multi-disciplinary team (MDT) members working on the study who were of Pacific descent. This may have affected retention rates and quality of service and experiences for participants in the study, due to the potential gaps in Pacific cultural competency levels, of the MDT team members. Previous research has found that non-Pacific providers may lack an understanding of Pacific collectivist cultural values and practices [19]. Although one answer to this issue going forward would be to employ Pacific health professionals on MDT teams, there is a significant and ongoing paucity of Pacific health professionals available to work in weight loss surgery MDT roles across NZ [20]. As such, it would not be practical to expect all members of a bariatric MDT taking part in a Pacific-led preoperative program to be of Pacific descent. One way to approach this gap is an intervention aimed at developing the knowledge and Pacific cultural competency [21, 22] of all non-Pacific MDT members. Taking this limitation into account, the current study overall supports the need for affirmative action at the policy level to include Pacific-led preoperative weight loss surgery programs into existing publicly funded weight loss surgery programs.
Translations
Talanoa: talk or discussion.
Aroha: to love, feel pity, feel concerned for, feel compassion, empathize.
Manaakitanga: hospitality, kindness, generosity, support—the process of showing respect, generosity, and care for others.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Adams TD Davidson LE Litwin SE Weight and metabolic outcomes 12 years after gastric bypass N Engl J Med 2017377121143115510.1056/NEJ Moa 170045928930514 PMC 5737957 · doi ↗ · pubmed ↗
- 2Cornejo-Pareja I Molina-Vega MGómez-Pérez AM Factors related to weight loss maintenance in the medium-long term after bariatric surgery: a review J Clin Med 2021108173910.3390/jcm 1008173933923789 PMC 8073104 · doi ↗ · pubmed ↗
- 3English WJ De Maria EJ Hutter MM American Society for Metabolic and Bariatric Surgery 2018 estimate of metabolic and bariatric procedures performed in the United States Surg Obes Relat Dis 202016445746310.1016/j.soard.2019.12.02232029370 · doi ↗ · pubmed ↗
- 4Sundström J Bruze G Ottosson J Weight loss and heart failure: a nationwide study of gastric bypass surgery versus intensive lifestyle treatment Circulation 2017135171577158510.1161/CIRCULATIONAHA.116.02562928258170 PMC 5404408 · doi ↗ · pubmed ↗
- 5Müller TD Blüher M Tschöp MH Anti-obesity drug discovery: advances and challenges Nat Rev Drug Discov 202221320122310.1038/s 41573-021-00337-834815532 PMC 8609996 · doi ↗ · pubmed ↗
- 6De Lorenzo A Romano L Di Renzo L Obesity: a preventable, treatable, but relapsing disease Nutrition 20207111061510.1016/j.nut.2019.11061531864969 · doi ↗ · pubmed ↗
- 7Rubino F Schauer PR Kaplan LM Metabolic surgery to treat type 2 diabetes: clinical outcomes and mechanisms of action Annu Rev Med 20106139341110.1146/annurev.med.051308.10514820059345 · doi ↗ · pubmed ↗
- 8Ministry for Pacific Peoples. Pacific Aotearoa status report: a snapshot. 2020. Retrieved from https://www.mpp.govt.nz/assets/Reports/Pacific-Peoples-in-Aotearoa-Report.pdf.