Ogilvie's Syndrome in a Male With Bladder Cancer
Jacqueline T Wesolow

TL;DR
This case report describes a male with bladder cancer who developed Ogilvie's syndrome, a condition causing severe colon distention without blockage.
Contribution
The novelty lies in presenting a rare case of Ogilvie's syndrome in a bladder cancer patient, highlighting its management and clinical course.
Findings
The patient exhibited massive colon dilatation without obstruction, consistent with Ogilvie's syndrome.
Supportive care, including decompression and total parenteral nutrition, was used to manage the condition.
The case emphasizes the importance of recognizing and treating Ogilvie's syndrome to prevent bowel complications.
Abstract
Ogilvie's syndrome is characterized by massive distention of the colon without evidence of physical obstruction. This condition can present itself with abdominal distention that is difficult to treat and can lead to ischemia of the bowels and, ultimately, bowel perforation. Treatment is aimed at supportive care with decompression, intravenous fluid hydration, and symptom control. This is a case presentation of Ogilvie's syndrome in an 80-year-old male with bladder cancer. He presented with abdominal distention and was found to have massive dilatation of his colon without evidence of obstruction on a CT scan. He was managed with supportive care, including stool softeners, and ultimately placed on total parenteral nutrition.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
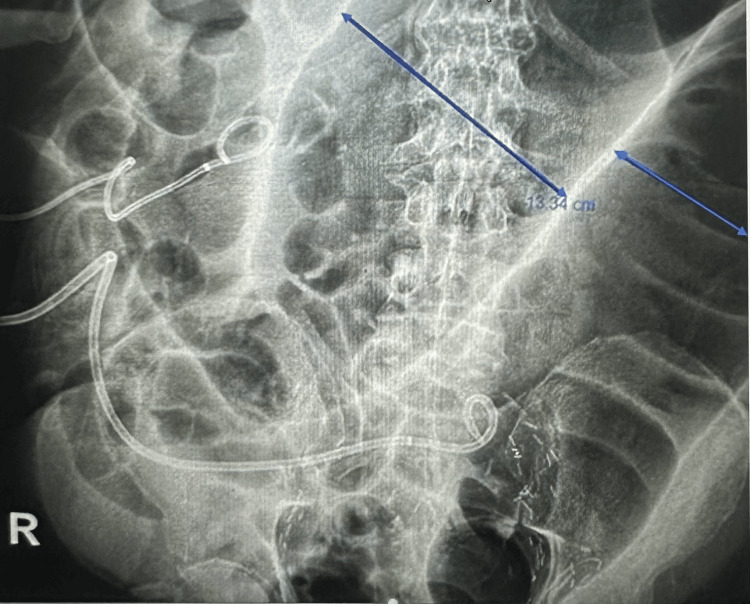 Figure 1
Figure 1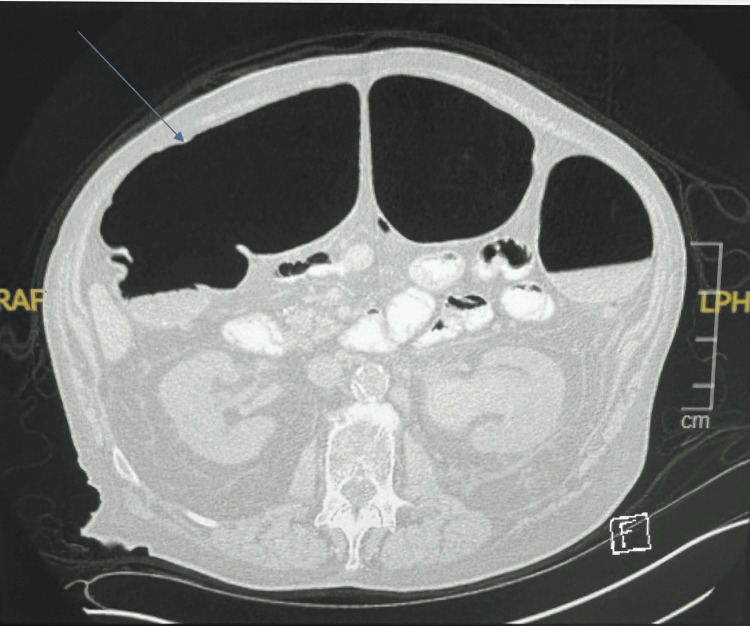 Figure 2
Figure 2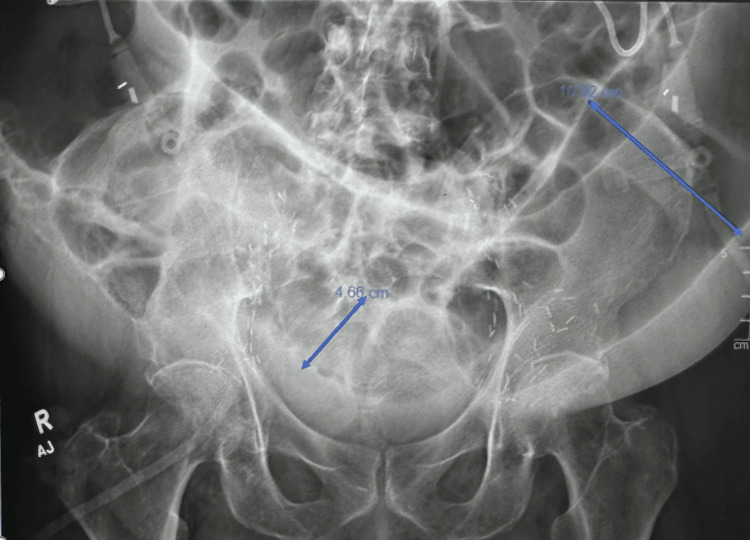 Figure 3
Figure 3 Figure 4
Figure 4| Lab | Patient’s Value | Normal Range |
| Sodium | 135 mEq/L | 135 to 145 mEq/L |
| Potassium | 5.5 mmol/L | 3.6 to 5.2 mmol/L |
| Chloride | 107 mEq/L | 96 to 106 mEq/L |
| CO2 | 15 mEq/L | 23 to 29 mEq/L |
| Creatinine | 3.5 mg/dL | 0.6 to 1.1 mg/dL |
| Phosphorus | 4.1 mg/dL | 2.8 to 4.5 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Pediatric Hepatobiliary Diseases and Treatments · Esophageal and GI Pathology
Introduction
Ogilvie’s is a condition characterized by massive colonic distention that is not due to a mechanical obstruction [1]. These patients do not have any mass or physical blockage causing the distention; hence, it also being called a pseudo-obstructive process. Diagnosis is based on radiographic findings showing colonic distention [1,2]. The distention, if severe enough, can ultimately lead to ischemia or colon perforation, and when that occurs, it has a high mortality rate of ~ 40% [2]. Given the high morbidity and mortality associated with this condition, it is imperative to identify Ogilvie’s in patients. This is seen in the ill, immunosuppressed, or hospitalized patient population. Patients can present with abdominal distention, discomfort, nausea, or vomiting, among other symptoms. Treatment is aimed at supportive care, which includes intravenous fluid hydration, decompression of the abdomen and pain control [2,3].
Case presentation
An 80-year-old male with a past medical history of stroke, atrial fibrillation, COPD, diabetes type 2, hypertension, obesity, obstructive sleep apnea, osteoporosis, and bladder cancer status post radical cystoprostatectomy with ileal conduit creation with ureteral stent that presented to our cancer center's urgent care with hematuria and left flank pain. The patient was recently admitted to our cancer center for two weeks with renal failure secondary to obstruction and displacement of his left ureteral stent. Stent was exchanged at that time. On this presentation, his left ureteral stent was found to be again displaced and coiled within the left ureter. He was subsequently admitted to our internal and hospital medicine services and successfully underwent a stent exchange with our interventional radiology team. Most of his electrolytes were close to or within the normal range (Table 1).
His abdomen was noted to be severely distended. An abdominal X-ray showed extensive colonic distention measuring 11 cm in the descending colon and 13.34 cm in the transverse colon, with extensive postsurgical changes in the pelvis (Figure 1). The patient had persistent bowel dilation throughout his hospital course, with ongoing abdominal distention and significant bowel dilation. A CT scan of the abdomen and pelvis revealed diffuse dilatation of the proximal colon (Figure 2). No evidence of obstruction was noted on the CT scan, supporting the diagnosis of Ogilvie's syndrome.
Abdominal X-ray showing extensive colonic distention up to 13.34 cm.
CT imaging of the abdomen and pelvis shows diffuse dilatation of the proximal colon.
Repeated serial abdominal X-rays noted persistent bowel distention. An X-ray about two weeks into his hospital stay showed a small bowel loop in the pelvis measuring 4.7 cm, with the distal descending colon measuring 10.5 cm (Figure 3). The patient was seen by our gastroenterology surgery team for what was initially thought to be colonic ileus, likely multifactorial related to recent procedures, surgical history, and decreased activity. The patient had bowel movements. The surgery team at the time recommended that the patient remain nothing per oral with sips of clears. The patient had multiple follow-up scans for monitoring, which were also concerning for a possible ileus. He had a nasogastric tube inserted, which was eventually removed without improvement in bowel distention. He was started on total parental nutrition since a gastric tube placement was likely not to be successful, given the degree of bowel dilation and the lack of an adequate window for placement. Additionally, the patient underwent an upper gastrointestinal small bowel follow-through study that showed a normal stomach-to-cecum transit time of approximately two hours (Figure 4). No obvious gastric retention was seen in this study, further supporting the diagnosis of Ogilvie's syndrome.
Abdominal X-ray showing severe colonic distention
The small bowel follow-through study revealed contrast throughout without evidence of obstruction.
The patient was continued on stool softeners and miralax throughout the hospital stay. He remained dependent on total parental nutrition as his primary source of hydration and energy and was discharged from it. A detailed discussion was conducted with the patient and his family on the importance of following up with his primary care physician.
Discussion
Ogilvie’s syndrome carries a high morbidity and mortality risk and is therefore, an important diagnosis to identify early on. Can often be mistaken for ileus if not properly followed up with. This can lead to further distention of the abdominal walls and cause acute ischemia of the bowel, which can lead to a life-threatening abdominal perforation. Diameters of more than 14cm are associated with a higher risk of perforation [4]. Treatment consists of conservative management, including nothing per oral (NPO), intravenous fluid hydration, and symptom control. Due to the dehydration and malnutrition associated with this condition, electrolyte imbalances are often seen. Patients can present with, most notably, hypokalemia, hypocalcemia, and hypomagnesemia [5].
Monitoring can include follow-up serial abdominal series X-rays while the patient is in the hospital. In patients with a cecal diameter of more than 12cm or who have failed supportive management, neostigmine can be considered as a treatment option [6,7]. Decompression with a nasogastric tube is an option and can be helpful for patients who are severely distended with pain. If there is evidence of perforation, then endoscopic decompression and/or a surgical consultation can be considered. Colonoscopic decompression has been shown to decrease the cecal diameter in about 73%-100% of cases [1].
It is thought that neural processes lead to massive colonic distention, causing dysmotility [6]. Ogilvie’s has been reported after surgeries including orthopedic, obstetric, and urologic [6-7]. Pain medications such as opioids should be avoided as they slow down the transit of stool in the bowels, thus increasing the risk of fecal impaction and potentially leading to increased colonic distention. Also, drugs that decrease the motility of the gut, such as antidepressants, antihistamines, and antipsychotics, should also be minimized or avoided. These medications are part of the anticholinergic family of drugs that inhibit nerve impulses responsible for involuntary muscle action, thus decreasing colonic motility [7,8]. It is imperative to review all of the patient’s medications thoroughly.
Unfortunately, our patient could not tolerate much more than sips of clear liquids. Therefore, he required total parenteral nutrition as the main form of nutrition. Our patient stabilized while on total parenteral nutrition. This is a difficult disease process for patients and their families to live with. Consulting with a social worker or patient support team can assist with this disorder. Proper follow-up after patient discharge from a hospital setting with a primary care physician is key to ensuring optimal management.
Our patient case represents a classic clinical scenario of Ogilvie's syndrome. A literature review of another patient case describes a 71-year-old woman with Ogilvie's syndrome who presented with similar symptoms of abdominal distention and pain [3]. Her CT abdomen and abdominal X-rays revealed a parallel pattern of marked non-obstructive distention [3]. Of note, both cases represent a geriatric population.
Conclusions
Ogilvie's syndrome is a rare disease process in which the colon becomes massively distended. It is thought that neural processes lead to the marked distention. Patients can present with abdominal distention, discomfort, and a wide range of electrolyte abnormalities, such as hypokalemia and hypomagnesemia. It is seen commonly in the elderly and hospitalized patient populations. It can lead to bowel ischemia and perforation; therefore, it is crucial to identify this as early on as possible. Just as in our case, treatment includes bowel rest, decompression, and supportive care. Continued close monitoring and follow-up is key to decreasing the risk of perforation and ensuring the best possible outcome for these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute intestinal pseudo-obstruction (Ogilvie's syndrome)Clin Colon Rectal Surg Maloney N Vargas HD 961011820052001134810.1055/s-2005-870890 PMC 2780141 · doi ↗ · pubmed ↗
- 2Ogilvie's syndrome-acute colonic pseudo-obstruction J Visc Surg Pereira P Djeudji F Leduc P Fanget F Barth X 9910515220152577074610.1016/j.jviscsurg.2015.02.004 · doi ↗ · pubmed ↗
- 3A challenge called Ogilvie's syndrome Cureus Soares Miranda L Silva Gonçalves C Silva E FerreiraÁ Araújo Correia J Cruz AR 015202310.7759/cureus.40233 PMC 1033281937435268 · doi ↗ · pubmed ↗
- 4Ogilvie's syndrome: management and outcomes Medicine (Baltimore) Haj M Haj M Rockey DC 097201810.1097/MD.0000000000011187 PMC 607615729979381 · doi ↗ · pubmed ↗
- 5A case of acute colonic pseudo-obstruction (Ogilvie's Syndrome) in a nonsurgical patient with plasma cell leukemia Case Rep Nephrol Hamid A Sabu J Elhawary O Puri I Salifu M Oh M Mallappallil M 6431248202220223646600210.1155/2022/6431248 PMC 9712016 · doi ↗ · pubmed ↗
- 6Early resolution of Ogilvie's syndrome with intravenous neostigmine: a simple, effective treatment Dis Colon Rectum Turégano-Fuentes F Muñoz-Jiménez F Del Valle-Hernández E 13531357401997936911210.1007/BF 02050822 · doi ↗ · pubmed ↗
- 7Acute colonic pseudo-obstruction: rapid correction with neostigmine in the emergency department J Emerg Med Mc Namara R Mihalakis MJ 1671703520081824292310.1016/j.jemermed.2007.06.043 · doi ↗ · pubmed ↗
- 8Acute colonic pseudo-obstruction: a pharmacologic approach Ann R Coll Surg Engl Hutchinson R Griffiths C 364367741992 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 2497637/1416711 PMC 2497647 · pubmed ↗