Magnetic resonance imaging for the assessment of cardiac compression caused by a giant hiatal hernia
Satoshi Kurisu, Hitoshi Fujiwara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
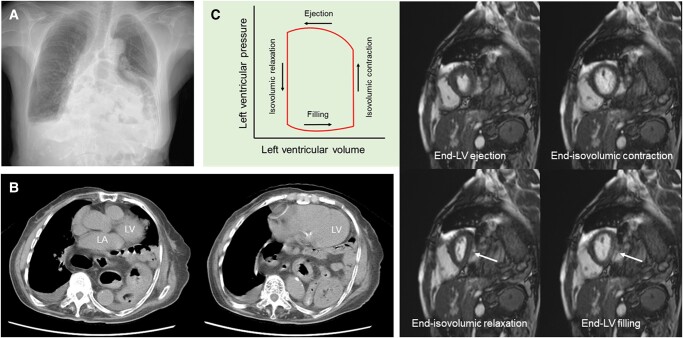 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastroesophageal reflux and treatments · Esophageal and GI Pathology · Dysphagia Assessment and Management
An 86-year-old woman with an untreated giant hiatal hernia presented with a 3-month history of exertional dyspnoea.^1^ A chest radiograph showed multiple abnormal gas shadows overlapping the heart (Figure 1, Panel A). Right-sided pleural effusion suggested heart failure. Computed tomography revealed a giant hiatal hernia with most of the stomach escaping into the thoracic cavity (Figure 1, Panel B). The hernia was located immediately adjacent to the left ventricle (LV) and atrium. Cine magnetic resonance imaging (MRI) was performed to assess the effects of the giant hiatal hernia on LV function during a cardiac cycle (Figure 1, Panel C). Serial LV short-axis images at the following four time points are shown with the schematic diagram of the LV pressure-volume curve. First, the LV free wall was compressed from the hiatal hernia at the end of the LV filling with a characteristically inverted D-shaped LV cavity (lower right corner, arrow). Next, LV pressure increased at the end of isovolumic contraction, thereby producing a circular LV cavity (upper right corner). Subsequently, LV volume decreased with a circular and smaller LV cavity at the end of LV ejection (upper left corner). Finally, LV pressure decreased at the end of isovolumic relaxation, thereby reproducing an inverted D-shaped LV cavity (lower left corner, arrow). Despite the significant cardiac compression visualized on MRI, N-terminal pro-brain natriuretic peptide level (41 pg/mL) was not elevated, and this may be due to impaired LV stretching.^2^ It was suggested that dyspnoea was due to mechanical effects of the giant hiatal hernia, which caused impaired LV filling as well as reduced lung capacity. She refused surgical treatment and was followed up with home oxygen therapy.^3^
Most patients with hiatal hernia are asymptomatic. Typical symptoms include gastroesophageal disease, whereas heart failure as a main symptom is rare. Clinicians should recognize giant hiatal hernia as a possible cause of heart failure.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Matar A , Mroue J, Camporesi E, Mangar D, Albrink M. Large hiatal hernia compressing the heart. Am J Cardiol 2016;117:483–484.26704030 10.1016/j.amjcard.2015.10.064 · doi ↗ · pubmed ↗
- 2Minai K , Komukai K, Arase S, Nagoshi T, Matsuo S, Ogawa K, et al Cardiac tamponade as an independent condition affecting the relationship between the plasma B-type natriuretic peptide levels and cardiac function. Heart Vessels 2013;28:510–513.22926410 10.1007/s 00380-012-0278-x · doi ↗ · pubmed ↗
- 3Mitiek MO , Andrade RS. Giant hiatal hernia. Ann Thorac Surg 2010;89:S 2168–S 2173.20494004 10.1016/j.athoracsur.2010.03.022 · doi ↗ · pubmed ↗