Environmental screening for SARS-CoV-2 in long term care facilities: lessons from a pilot study
Rachel Kwiatkowska, Nicola Yaxley, Ginny Moore, Allan Bennett, Matthew Donati, Nicola Love, Roberto Vivancos, Matthew Hickman, Derren R Ready, Timothy R. Julian, Rachel Kwiatkowska

TL;DR
This study explored how SARS-CoV-2 spreads in long-term care facilities through environmental surfaces and found that RNA was detectable, especially in rooms with infected residents.
Contribution
The study provides insights into environmental SARS-CoV-2 detection in LTCFs and suggests elevated surfaces may be better sampled for surveillance.
Findings
SARS-CoV-2 RNA was detected in LTCFs, particularly in rooms with infected residents.
Elevated surfaces were more likely to test positive than common touch-points.
Facilities with enhanced IPC measures had lower contamination levels.
Abstract
Background: The SARS-CoV-2 pandemic has highlighted the risk of infection transmission in long-term care facilities (LTCF) and the vulnerability of resident populations. It is essential to understand the environmental spread of the virus and risk of indirect transmission to inform Infection Prevention and Control (IPC) measures in these settings. Methods: Upon notification of SARS-CoV-2 outbreaks, LTCF within a local authority in the South West of England were approached to take part in this pilot study. Investigators visited to swab common touch-points and elevated ‘non-touch’ surfaces and samples were analysed for presence of SARS-CoV-2 genetic material (RNA). Data were collected regarding LTCF infrastructure, staff behaviours, clinical and epidemiological risk factors for infection (staff and residents), and IPC measures. Criteria for success were: recruitment of three LTCF;…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
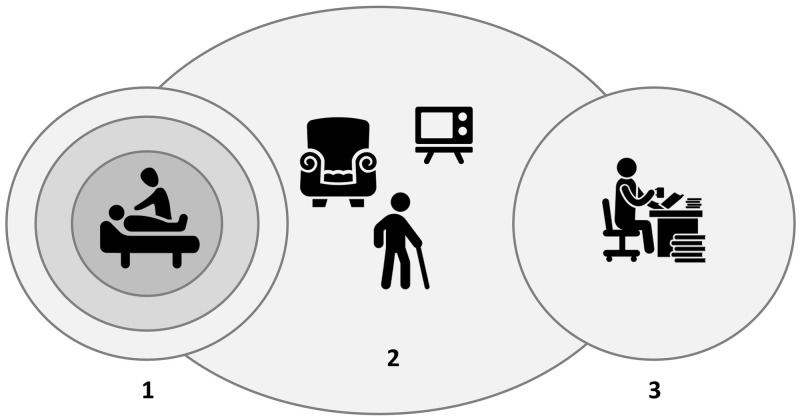 Figure 1
Figure 1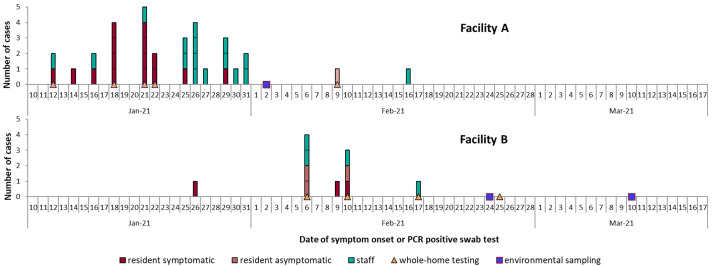 Figure 2
Figure 2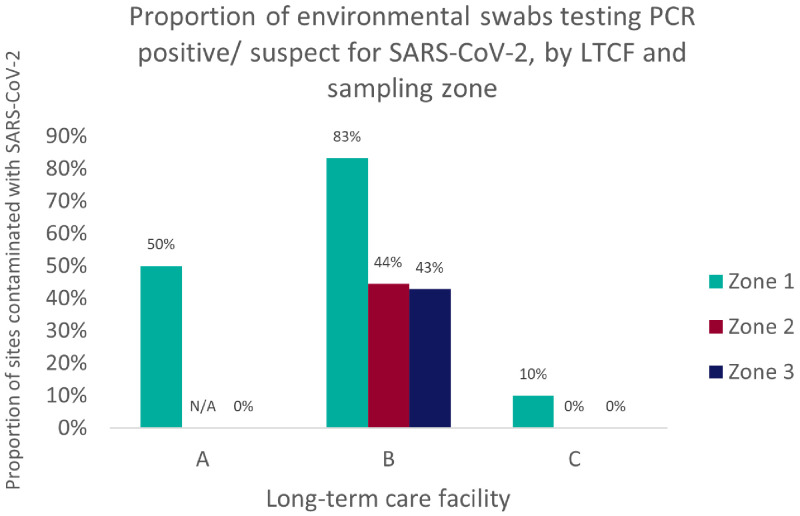 Figure 3
Figure 3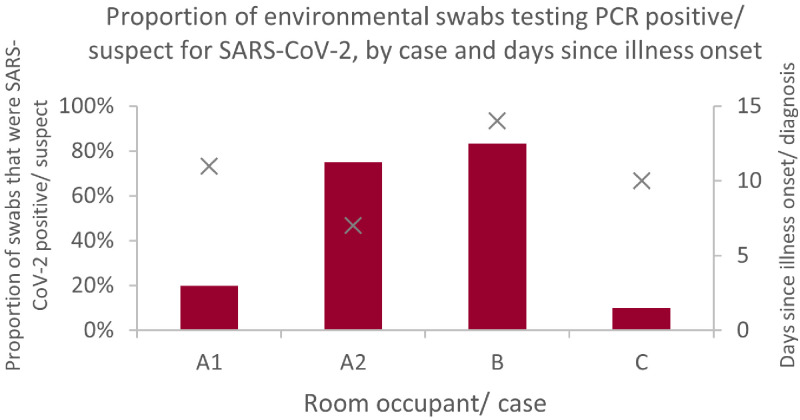 Figure 4
Figure 4| Facility A: sampling sites |
| PCR
| Facility B: sampling sites |
| PCR
| 2nd visit
| Facility C: sampling sites |
| PCR
|
|---|---|---|---|---|---|---|---|---|---|
|
|
|
| |||||||
| 1. Top of lockers (next to door) | E | Negative | 1. Air vent/ extractor | E | Negative | Negative | 1. Top of key cupboard | E | Negative |
| 2. Toilet door: inside handle
| T | Negative | 2. Soap dispenser lever | T | Negative | Negative | 2. Computer mouse | T | Negative |
| 3. Air vent/ extractor (toilet) | E | Negative | 3. Door ledge (outer) | E | Positive (Ct N
| Negative | 3. Top of message board | E | Negative |
| 4. Bench top | T | Negative |
| 4. Telephone receiver | T | Negative | |||
| 5. Soap dispenser lever | T | Negative (Ct N
| 4. Computer mouse | T | Negative | Negative |
| ||
|
|
| 5. Air vent/ extractor | E | Negative | |||||
| 6. Top of TV | E | Negative | 5. Air vent/ extractor | E | Positive (Ct N
| Negative | 6. Soap dispenser lever | T | Negative |
| 7. Top of trolley (for lunch
| E | Negative | 6. Glove box (size small) | T | Negative | N/A |
| ||
| 8. Radio dials | T | Negative |
| 7. Front door keypad (inside) | T | Negative | |||
|
| 7. Toilet booster handles | T | Negative | Negative | 8. Top of kitchen door frame (outside) | E | Negative | ||
| 9. Code pad (door exterior) | T | Negative | 8. Air vent/ extractor | E | Positive (Ct N
| Negative |
| ||
|
| 9. Toilet booster underside | T | Negative | Negative | 9. Air vent/ extractor | E | Negative | ||
| 10. Chair arms | T | Negative |
| 10. Fire exit sign | E | Negative | |||
| 11. Air vent/ extractor | E | Negative | 10. Tablecloth | T | Suspect (Ct N
| Negative | 11. Door handle (exit to reception) | T | Negative |
| 12. Light switch | T | Negative | 11. Tea trolley handles | T | Negative | Negative | 12. Bannister | T | Negative |
|
| 12. Armchair handles | T | Negative | Negative |
| ||||
| 13. UV cabinet handle | T | Negative | 13. Top of picture frame | E | Suspect (Ct N
| Negative | 13. Top of kitchen hatch | E | Negative |
|
| 14. TV remote control | T | Positive (Ct N
| Negative | 14. Chair arms | T | Negative | ||
| 14. Photocopier digital pad | T | Negative |
| 15. Kettle handle & switch | T | Negative | |||
|
| 15. Top of wardrobe | E | Positive (Ct N
| Positive (Ct N
| 16. Microwave handle & dial | T | Negative | ||
| 15. Bedrails (unoccupied) | T | Suspect (Ct N
| 16. Fingertips (L hand) | - | Negative | Negative | 17. Air vent/ extractor | E | Negative |
| 16. Fingertips (R hand) | - | Negative | 17. Fingertips (R hand) | - | Negative |
| |||
| 17. Hoist handle | T | Negative | 18. TV remote | T | Positive (Ct N
| Negative | 18. Glove box – size small | T | Negative |
| 18. Chair seat (occupied) | T | Negative | 19. Tabletop (swab) | T | Negative | Negative | 19. Lip of PPE cabinet | T | Negative |
| 19. Air vent/ extractor
| E | Negative | 20. Tabletop (sponge) | T | Positive (Ct N
| 20. Air vent/
| E | Negative | |
| 20. Catheter stand (bathroom) | T | Negative | 21. Chair arms | T | Positive (Ct N
| Negative | 21. Hand rail | T | Negative |
|
| 22. Walking frame handles | T | Positive (Ct N
| Negative |
| ||||
| 21. Bed remote control
| T | Positive (Ct N
| 23. Bed head | T | Suspect (Ct N
| Suspect (Ct N
| 22. Fingertips (R hand) | - | Negative |
| 22. Air vent/ extractor
| E | Negative | 24. Wardrobe handle | T | Suspect (Ct N
| Negative | 23. Fingertips (L hand) | - | Negative |
| 23. TV control (in use) | T | Positive (Ct N
| 25. Bathroom door handle (outer) | T | Suspect (Ct N
| 24. Table top | T | Negative | |
| 24. Top of TV | E | Positive (Ct N
| 26. Bathroom door handle
| T | Suspect (Ct N
| 25. Chair arms | T | Negative | |
| 25. Top of clock | E | Negative | 27. Air vent/ extractor
| E | Positive (Ct N
| Positive (Ct N
| 26. Bed remote control | T | Negative |
| 26. Commode seat (bathroom) | T | Positive (Ct N
| 28. Toilet seat booster | T | Negative | Negative | 27. Bed head | T | Negative |
| 27. Fingertips (both hands) | - | Negative |
| 28. Walking frame handles | T | Negative | |||
| 28. Top of light above
| E | Positive (Ct N
| 29. Bannister outside
| T | Negative | 29. Curtain
| E | Negative | |
| 29. Oxygen saturations probe
| T | Positive (Ct N
|
| 30. Wheelbarrow handles | T | Negative | |||
| 30. Top of key cabinet | E | Positive (Ct N
| 31. Air vent/ extractor
| E | Suspect (Ct N
| ||||
| 32. Hoist rail (bathroom) | T | Negative | |||||||
| 33. Toilet handle | T | Negative | |||||||
| ID | CQC
| No.
| No.
| Private/
| Care
| Agency
| Dependent/
| Age
| Walk
| Prevalence
|
|---|---|---|---|---|---|---|---|---|---|---|
| A | O | 30/40 (75.0%) | 1 | Private | Residential:
| Yes - block | Mixed | 55–98 | No | 23/30 (76.7%) |
| B | G | 15/16 (93.8%) | 2 | Mixed | Residential:
| Yes | Mixed | 71–97 | Yes | 13/15 (86.7%) |
| C | G | 12/13 (92.3%) | 2 | Private | Residential:
| No | Mixed | 35–88 | Yes | data unavailable |
| ID | Outbreak metrics | Infection Prevention & Control | COVID-19 vaccine | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Attack rate
| Attack rate
| Duration
| COVID-19
| Hospital
| Residents
| Staff
| Staff
| Closed to
| Enhanced
| PPE
| Uptake
| Uptake
| |
| A | 16/30 (53%) | 16/60 (27%) | 63 | 2 | 5 | All | Yes | Yes | Yes
| Yes | Yes | 25/30 (83%) | 147/183 (80%)
|
| B | 6/15 (40%) | 4/22 (18%) | 50 | 1 | 3 | Cases | No | Yes | Yes | Yes | Yes | 15/15 (100%) | 12/22 (55%) |
| C | 1/12 (8%) | 1/35 (3%) | 30 | 0 | 0 | Cases | Yes | Yes | Yes | Yes | Yes | 12/12 (100%) | 24/25 (96%) |
| LTCF | No. (proportion)
| No. (proportion)
|
|---|---|---|
| A | 5/17 (29%) | 2/10 (20%) |
| B | 10/20 (50%) | 6/7 (86%) |
| C | 0/19 (0%) | 1/10 (10%) |
|
|
|
|
- —Wellcome GW4 Clinical Academic Training programme
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfection Control and Ventilation · COVID-19 and healthcare impacts · COVID-19 and Mental Health
Introduction
Long term care facilities (LTCF) are inadvertently ideal environments for the spread of pathogens. ( Strausbaugh et al., 2003) Residents are often susceptible to infection or colonisation, and in frequent and close contact with staff who have links to the wider community. Outbreaks of infectious diseases are common in these settings ( Inns et al., 2017; Inns et al., 2019) and the coronavirus 2019 (COVID-19) pandemic, caused by SARS-CoV-2 coronavirus, has highlighted the vulnerability of people in LTCF to infectious disease threats: there were an estimated 29,542 excess deaths among LTCF residents over the first 23 weeks of the epidemic in England. ( Morciano et al., 2021)
If detected early enough transmission of pathogens within the LTCF can be curbed, ( Inns et al., 2018) however SARS-CoV-2 infections are often asymptomatic or paucisymptomatic leading to large outbreaks. Regular testing of residents and staff helps identify cases early but is resource-intensive and unpleasant for frail individuals, so non-invasive surveillance strategies may be more sustainable in the long term. Swabbing touch-points and elevated surfaces (which airborne pathogens will settle on) could provide early warning of infection as well as providing insights into how the virus is transmitted, which can inform infection prevention and control (IPC) measures. According to a World Health Organization scientific brief on transmission of SARS-CoV-2 (2020), direct (droplet) transmission and indirect spread via fomites (contaminated surfaces) and long-distance aerosols are thought to occur; however there is no conclusive evidence for indirect transmission in LTCF. ( Ben-Shmuel et al., 2020; Greenhalgh et al., 2021; Ong et al., 2020; Ye et al., 2020)
COVID-19: Detecting Indirect Transmission in Facilities for Enhanced Care sTudy (COVID-19: DISinFECT) aims to investigate the role of indirect transmission of SARS-CoV-2 in LTCF and evaluate the potential for environmental surveillance to inform IPC measures. We present findings from a pilot conducted between 14 ^th^ January and 28 ^th^ March 2021, during the second epidemic wave in South West England.
Methods
DISinFECT methods are detailed in the protocol which can be accessed online. ( Kwiatkowska & Ready, 2021) LTCFs were eligible for inclusion if they provided residential care for older adults (>65 years), were within the boundaries of a selected local authority in the Public Health England (PHE) South West region, and experienced a COVID-19 outbreak, defined as two or more laboratory-confirmed cases among staff and/or residents within a 14-day period.
Recruitment
On notification of an outbreak, investigators contacted the LTCF manager with information about DISinFECT and offered environmental sampling as part of outbreak management. If managers expressed an interest they were asked to complete a consent form permitting the study team to conduct telephone interviews, collect information from care home records, sample the care home environment and approach residents and staff for involvement. Prior to the sampling visit, residents and staff were provided with written and pictorial leaflets describing the purpose of the investigations, sampling procedures and how their information would be processed. Each of the residents selected for sampling was consulted to make sure they understood this information and were happy to provide samples. Sampling was not carried out if the individual lacked capacity to complete a consent form. Staff were asked for consent to participate prior to accessing the electronic questionnaire.
Sampling
Settings varied in size and layout but sampling was done systematically, with a focus on common touch points (for example: door handles, light switches, television remote controls) and elevated surfaces onto which airborne virus might settle (for example: door sills, tops of wall-mounted cabinets).
Within each home, sampling sites were categorised in to three ‘zones’: 1) rooms occupied by residents isolating with active SARS-CoV-2 infection, or equipment used by them, 2) areas/equipment used by both staff and residents such as lounges and dining areas, shared kitchen equipment, and 3) staff-only areas/equipment such as offices, recreation areas, and key cabinets (see Figure 1). Surfaces were sampled using wetted flocked swabs and sponges, and wetted swabs were also used to swab the fingertips of residents in isolation rooms. All samples were transported to a public health laboratory specialising in aerobiology, biocontainment and biosafety measures.
Sampling zones in care homes recruited to DISinFECT: 1) rooms/ equipment used mainly by residents, 2) areas/equipment shared by both residents and staff, and 3) staff-only areas/ equipment. Image icons by Delwar Hossain and ProSymbols, sourced from https://thenounproject.com/.
The full DISinFECT protocol includes sampling stool and saliva from resident cases and air and wastewater sampling from the facility but for logistical reasons, stool and saliva could not be taken during this pilot. Likewise, no air sampling was conducted, and wastewater was collected from only one facility; results will be reported separately.
Laboratory analysis
Each sample was analysed in duplicate using a Reverse Transcription Polymerase Chain Reaction (RT-PCR) assay targeting both the N gene and the ORF1ab gene of SARS-CoV-2 (Viasure, CerTest Biotec, Zaragoza). Results were reported in cycle threshold (Ct) numbers. A sample was classified as ‘positive’ for SARS-CoV-2 if amplification of one or both targets was detected in both duplicates; ‘suspect’ if detected in only one duplicate and ‘negative’ if no amplification was detected for either gene target (Ct cut-off was 39). RT-PCR was repeated (in duplicate) for ‘suspect’ samples and samples with an internal control Ct standard deviation of >0.5. If repeat RT-PCR detected amplification of a gene target in both duplicates then the ‘suspect’ sample was reclassified as ‘positive’; otherwise the sample remained ‘suspect’.
Where possible, diagnostic isolates were sent for whole genome sequencing (WGS) to identify SARS-CoV-2 variants and mutations of interest/concern.
Epidemiological data collection
In addition to sampling, the study team recorded details of LTCF layout, cleaning and IPC measures, and staff and resident behaviours. Clinical test results (nasopharyngeal swabs analysed with PCR) were obtained from the regional public health laboratory and LTCF managers provided additional information about clinical case notifications, resident risk factors for infection and IPC measures. Finally, staff members were sent an electronic questionnaire asking questions about exposures and risk factors for infection.
Criteria for success in the pilot are presented in Box 1.
Box 1. DISinFECT pilot criteria for successa) Recruitment of three LTCF and consent to participate from at least one resident per facility;b) Detection of SARS-CoV-2 RNA from surface sampling;c) Variation by sampling zone in the proportion of sample sites testing positive for SARS-CoV-2 RNA;d) Potential to assess transmission risk from environmental contamination, in the context of individual risk factors for infection.
Ethical considerations
These investigations were carried out as part of a public health response to the SARS-CoV-2 pandemic. Ethical approval was granted on 14 ^th^ January 2021 by the Public Health England Research Ethics and Governance Group (PHE REGG: RD 415).
Results
Four LTCFs were approached on notification of an outbreak: one declined to participate on the grounds that they did not have capacity to consider the study information or arrange for residents to be consulted. Three LTCFs were sampled between 2 ^nd^ February and 10 ^th^ March 2021 and a total of 84 environmental swabs were taken (56 from common touch points, 28 from elevated sites). One home had two sampling visits, 14 days apart. For simplicity, we have labelled the homes A, B and C in order of sampling dates. Table 1 contains the full list of sampling sites.
Setting and population
LTCF sizes ranged in size: there were 40 beds in facility A, which was a self-contained unit within an 80-bedded LTCF, 16 beds in facility B and 13 beds in facility C. The number of occupants was 30 (A), 15 (B) and 12 (C) on the date of onset of the first case. Facility A was a short stay residential unit with clients aged between 55 and 98 years; facility B a residential home for older adults (65 and over) with and without dementia; facility C a residential home for adults with learning difficulties aged between 35 and 88 years. All residents were included in the epidemiological analysis, regardless of age. All residents slept in single occupancy rooms; residents in facilities A and C all had private bathrooms and 13/16 rooms in facility B were en-suite. Characteristics of the three facilities are summarised in Table 2.
Outbreak trajectory and control measures
SARS-CoV-2 attack rates among residents were highest in facility A: 16/30 (53%, of which 15/16 (94%) were symptomatic), followed by facility B: 6/15 (40%, of which 3/6 (50%) symptomatic). Only one resident tested positive in LTCF C (8%): this individual was asymptomatic and had received the first vaccine dose four weeks beforehand. They also had a history of laboratory-confirmed COVID-19 a year previously. A repeat sample taken 10 days after the most recent diagnosis was PCR negative for SARS-CoV-2, nonetheless the individual remained in isolation for 14 days as a precaution. Non-agency staff attack rates were also highest in facility A: 16/60 (27%) followed by facility B: 4/22 (18%) and C: 1/35 (3%). Numbers of agency staff were not available. Duration of outbreak (calculated from the date of first illness onset to 28 days after onset of the final case) was 63, 50 and 30 days for facilities A, B and C respectively. Facilities A and B had residents admitted to hospital (n=5 symptomatic cases and n=3 of which one was symptomatic, respectively). Sadly there were COVID-19-related deaths among residents (facility A: n=2, both receiving end-of-life care, one hospitalised; facility B: n=1, hospitalised). Figure 2 illustrates outbreak trajectories in facilities A and B.
Epidemic curves illustrating case onset in LTCFs A (30 residents) and B (15 residents).Community case rates peaked at the end of December during the second wave of the UK epidemic.
Only facility A (the short stay unit) was effectively isolating all residents within their rooms at the time of the sampling visit. Facilities A and C were cohorting staff, allocating them to work exclusively with SARS-CoV-2 positive residents or with SARS-CoV-2 negative residents, and the infected resident in facility C was isolated on a separate floor to the rest of the residents. Staff in all three facilities underwent daily lateral flow (point-of-care) antigen tests for a minimum of five days followed by routine twice weekly testing, as well as weekly PCR testing for SARS-CoV-2 according to national guidance for testing in care homes. All homes were closed to visitors and new admissions for the duration of the outbreak, except for end of life visits in facility A. Table 3 summarises outbreak metrics and control measures.
All homes adopted enhanced cleaning protocols in response to the COVID-19 epidemic, with increased frequency and a focus on common touch points. In addition, facility A provided fresh uniforms for staff at the beginning of each shift (laundered on site) and had installed a UV cabinet for treating phones and keys prior to handover. All LTCF managers stated that personal protective equipment (PPE) was available to staff in line with national guidance.
In facilities B and C, 100% of residents had received the first dose of a COVID-19 vaccine more than two weeks prior to outbreak onset. In facility A, 83% of residents had received the first dose of vaccine but just four days before onset of the outbreak. In facility A, 80% of non-agency staff were reported to have received a vaccine, though these figures related to the wider facility and exact vaccination dates were not provided. Facility B reported 55% and facility C 96% of non-agency staff vaccinated with at least one dose more than two weeks prior to the outbreak.
Observations
Facility A was a modern building with spacious, uncluttered rooms of a uniform layout. Signage was in place to remind staff to clean surfaces and socially distance, and the sampling team observed good adherence to PPE donning and doffing protocols. All residents were isolated in their rooms, and staff wore ‘scrubs’.
Facility B was an older building, once a large house. Residents’ rooms were small and somewhat cluttered with several sampling sites visibly soiled. Several residents were observed using the dining area and lounge (unmasked); staff wore their own clothing.
Facility C was a relatively modern building; rooms were small but uncluttered with fewer soft furnishings than LTCFs A and B. Two residents were observed walking with purpose (unmasked), accompanied by carers; staff wore their own clothing.
Proportion of sites testing positive and distribution of SARS-CoV-2 RNA
Facility B had the highest proportion of sampling sites testing positive/ suspect for SARS-CoV-2 RNA (PCR positive on one or both duplicates): 17/28 (61%), followed by LTCF A: 6/27 (22%). In LTCF C, all environmental swabs were negative for SARS-CoV-2 except for one suspect positive from an air extractor in the index case’s bathroom: positivity 1/31 (3%).
A repeat visit to facility B two weeks after the initial sampling visit yielded a much lower proportion of SARS-CoV-2 positive/ suspect sampling sites (4/19; 21%).
Concentrations of SARS-CoV-2 RNA, as inferred from Ct values, were very low for all positive and suspect samples. The lowest Ct value found was 31.8, and only four samples had a Ct value of below 35. Amplification was below the limit of detection in two samples (see Table 1).
SARS-CoV-2 positive/ suspect surfaces were most common in zone 1 (rooms occupied by residents with active SARS-CoV-2 infection, and equipment used by them), as illustrated in Figure 3.
Proportion of sampling sites testing PCR positive for SARS-CoV-2, by sampling zone.Zone 1 represents areas/ equipment used by COVID-19 positive residents; Zone 2: areas/facilities used by both residents and staff; Zone 3: staff-only areas/equipment. There were no zone 2 areas to sample in LTCF A, since all residents were confined to their rooms.
Proportion of SARS-CoV-2 positive sites in proximity to a COVID-19 case
Within zone 1, there was significant variation in the proportion of sample sites testing positive/ suspect for SARS-CoV-2 RNA. For example, in facility A two residents’ rooms were sampled: in the first room, 1/5 (20%) of sample sites was ‘suspect positive’ for SARS-CoV-2 RNA and in the second room 6/8 (75%) of sample sites tested positive. Both rooms were similar in size and layout, and subject to the same cleaning protocols. The first room was occupied by an individual who was bed/chair bound, and who had tested positive for the virus 11 days previously and had fever and a slight cough. The occupant of the second room spent much of their time confined to bed, though was mobile with a wheelchair. This individual tested positive for SARS-CoV-2 infection seven days prior to the visit and had a cough. Figure 4 shows the environmental sample site positivity in relation to the time from onset of illness for the room occupant.
Proportion of sample sites that tested positive for SARS-CoV-2 RNA within the rooms of infected residents.Resident A1 had fever and slight cough and was bed/chair-bound; A2 had a cough and was mobile with a wheelchair; B reported only lethargy, and was independently mobile; C was asymptomatic and independently mobile; this individual’s positive PCR result was unexpected given history of prior infection and vaccination.
Proportion of common touch points testing positive for SARS-CoV-2 vs elevated surfaces
Overall, the proportion of common touch points testing positive/ suspect for SARS-CoV-2 RNA (15/56; 27%) was slightly lower than the proportion of sites testing positive/ suspect (10/28; 36%), though this was not consistent between LTCFs (see Table 4). Where the proportion of positive common touch points was highest (facility B), a large proportion of elevated sites were also tested positive/ suspect for SARS-CoV-2 RNA.
Fingertip samples
None of the swabs taken from fingertips of residents with confirmed COVID-19 were PCR positive for SARS-CoV-2 RNA.
WGS of clinical isolates
A small number of outbreak isolates were sequenced by the COVID-19 Genomics UK Consortium (COG-UK) (facility A: n=3; facility B: n=3). All were identified as B.1.1.7 (VOC-202012/01), with no E484K substitution detected.
Staff survey results
Response rates to the electronic staff survey were poor: 11/60 (18%) from facility A, 6/22 (27%) from facility B and 0/35 (0%) from facility C, meaning there was insufficient data to assess clinical and epidemiological risk factors for infection. None of the respondents raised concerns about access to PPE as recommended in national guidelines for working in care homes.
Discussion
The greatest proportions of SARS-CoV-2 positive/ suspect sample sites were found in the immediate vicinity of laboratory-confirmed COVID-19 cases, which is consistent with findings from other studies and indicates that environmental swabbing can detect the presence of an infected individual. ( Onakpoya et al., 2021) The proportion of SARS-CoV-2 positive/ suspect sites varied considerably within zone 1 however, even between rooms with similar layouts and cleaning regimes occupied by individuals with comparable symptom profiles. The exact timing of cleaning was not captured and may have affected these results, though variation was also observed in elevated sites which were unlikely to have been cleaned as part of daily routine. Equally, the sensitivity of surface swabbing may have differed between rooms though the same sampler swabbed both. Environmental sampling around COVID-19 patients evacuated from the Diamond Princess cruise ship demonstrated a similar lack of correlation between clinical signs of illness and levels of environmental contamination. ( Santarpia et al., 2020) It is likely that our findings illustrate the myriad of environmental, clinical, behavioural and pathogen factors affecting dispersion of the virus, ( Moore et al., 2021) which must be controlled for in any analysis of infection risk by indirect transmission.
Survey response rates were poor, which is likely to reflect the pressures staff were under at the time. Consequently, there was insufficient epidemiological information to assess whether transmission occurred via fomites or long-distance aerosol during these outbreaks. Concentrations of SARS-CoV-2 RNA were very low for all positive and suspect samples, therefore it is highly unlikely that viable virus was present. ( Huang et al., 2020; Transmission of Covid-19 in the Wider Environment Group (TWEG) reporting to UK Scientific Advisory Group on Emergencies (SAGE) 2020) This is in keeping with results from environmental surveillance in Canadian care homes. ( Nelson et al., 2021)
The fact that fingertip swabs were all PCR negative for SARS-CoV-2, despite observing infected residents touch various items which returned a positive result, was surprising: people typically touch their nose, eyes and mouth more than 20 times per hour and an experimental study suggests that the virus can persist on skin for at least 8 hours at body temperature. ( Harbourt et al., 2020; Kwok et al., 2015) Sampling may have occurred too late to detect viral shedding, since participants were between seven and 14 days of diagnosis, and the concentration of virus on fomites was low which might reduce the likelihood of transfer to fingers. It is also possible that residents applied hand sanitiser unobserved, or that the sampler did not apply sufficient pressure or friction to pick up viral RNA. ( Mbithi et al., 1992)
Notably, facility A experienced the highest attack rates despite implementing more comprehensive IPC and cleaning measures compared to facilities B and C. Residents in facility A were more susceptible to infection than those in facilities B and C, having only received the first dose of vaccine shortly before the outbreak onset. ( Shrotri et al., 2021; Tenforde et al., 2021) Facility A also had a higher rate of admissions from the local hospitals and these factors, as well as the relatively large size of the facility, may have increased the probability of multiple introductions of the virus to the premises. ( Burton et al., 2020; Shallcross et al., 2021) Unfortunately staff survey response rates were too low to enable a comparative analysis of other infection risk factors within and outside the facility.
High attack rates may also have reflected community case rates, which peaked at the end of December and remained high through January (see Figure 2 for pilot LTCF outbreak trajectories). This surge in case rates was fuelled by emergence of the more transmissible B.1.1.7 Alpha variant, which quickly entered English LTCFs. ( Krutikov et al., 2021) At this time a substitution at the E484K location of the receptor binding domain also emerged, raising concerns that the virus might evade the host immune response. ( Wise, 2021) Six clinical samples were sequenced and were all of the B.1.1.7 Alpha variant with no E484K substitution, however we cannot exclude the possibility that multiple strains of the virus were contributing to these outbreaks.
Results from surface swabbing provided some reassurance that facility A (with staff cohorting and enhanced IPC measures) was effectively containing the environmental spread of the virus, in contrast to LTCF B (without cohorting) in which viral RNA was widely distributed. Repeat sampling 14 days after the initial visit to facility B yielded a much lower proportion of SARS-CoV-2 positive/suspect sites. Since the first visit corresponded with the end of the final case’s infectious period and no further cases of COVID-19 were identified it is reasonable to assume that nobody in the facility was actively shedding virus at the second sampling visit. Our observations could reflect the effectiveness of cleaning protocols introduced between sampling visits or of swabbing at the first round of sampling, or degradation of viral RNA over a 14 day period. ( Onakpoya et al., 2021; van Doremalen et al., 2020) Facility C was the only one to isolate its resident case on a separate floor/wing which may have helped reduce egress to other areas within the home. However, this individual’s history of vaccination and prior infection, and a negative repeat PCR test suggest that the diagnosis was a false positive and they were not shedding SARS-CoV-2 at the time of sampling.
Elevated sampling sites, being cleaned less regularly, may be a more pragmatic means of SARS-CoV-2 detection than common touch points: of the four sites that remained positive/suspect for SARS-CoV-2 on a repeat visit to facility B, three were elevated. Reactive sampling, as applied in this pilot, will not distinguish between historic and current viral shedding but there is evidence that levels of surface contamination with SARS-CoV-2 RNA mirror contemporaneous levels of airborne SARS-CoV-2 RNA. ( Cherrie et al., 2021; Dumont-Leblond et al., 2021) Air vents may be useful sentinel sampling points since three of four air vents in facility B tested positive for SARS-CoV-2 RNA, and in facility C the air vent was the only sampling site that tested suspect positive. Similar observations are reported from sampling ventilation grates in the Diamond Princess COVID-19 quarantine rooms, and respiratory viruses have been isolated from air filters in aeroplanes and large public buildings. ( Goyal et al., 2011; Korves et al., 2011; Santarpia et al., 2020) It is interesting that none of the air vents sampled from facility A tested positive for SARS-CoV-2 RNA, including one in a room that was otherwise quite heavily contaminated. This could have been an artefact of different sampling techniques, or reflect the design of the air vents, which were circular with a single ring opening rather than a slatted grate, though the vent that tested suspect positive in facility C was of the same circular design. Facility A may also have been better ventilated than the other facilities, however this seems unlikely given positive results in other elevated sites in the building.
The uncluttered environment in facility A, in reducing build-up of dust, may also have helped limit environmental spread of SARS-CoV-2. Evidence that respiratory droplets containing SARS-CoV-2 are adsorbed to dust and particulate matter, creating ‘aerosolised fomites’, is emerging ( Andree, 2020; Conticini et al., 2020; Qu et al., 2020; Renninger et al., 2021; Setti et al., 2020; Travaglio et al., 2021) and in healthcare settings we have observed that elevated surfaces accumulate greater quantities of SARS-CoV-2 RNA in dusty environments such as changing rooms, bathrooms, and cluttered spaces (unpublished data). This merits further investigation.
Limitations
This pilot has several limitations, not least the small sample size, lack of control sites and heterogeneity of LTCFs. Our interpretation of results is speculative and intended to generate hypotheses rather than answer questions.
Between-site variation in layout and infrastructure means that sampling frames cannot be entirely standardised, and there may be a tendency to oversample areas that are visibly soiled. Sampling technique may also vary between samplers. Results from surface swabs represent a snapshot in time and cover a fraction of the LTCF environment so we may not have accurately captured overall levels of environmental contamination. Among other things these may have been influenced by trends in community prevalence of COVID-19 (affecting risk of importation), expansion of new variants, and the effects of vaccination rollout (affecting viral shedding and transmissibility).
We were unable to confirm whether the diagnostic test for the single resident case in facility C was a true positive, therefore the SARS-CoV-2 RNA detected in this individual’s rooms may have been residual from previous occupants or their carers. This bias also applies to the other facilities to some extent, since all were likely to have been exposed to the virus (whether or not it manifested clinically) at some point prior to the outbreak.
Sequencing data were only available for minority of outbreak samples therefore we were unable to assess whether new or multiple strains were responsible for the outbreaks in question.
Conclusions and recommendations
We have successfully recruited three pilot LTCF to the DISinFECT study and observed SARS-CoV-2 RNA on a high proportion of surfaces around individuals with a laboratory-confirmed infection, though this varied considerably within and between settings.
This pilot demonstrates that surface swabbing can provide reassurance that IPC measures such as self-isolation, staff cohorting and enhanced cleaning collectively reduce egress of the virus from quarantine rooms to the wider care home environment. The heterogeneity of settings and situations means that we cannot assess impact of environmental contamination or individual IPC measures on transmission risk, however. An analysis of national LTCF-level data would be beneficial to assess which, if any, IPC measures influence attack rates during outbreaks of SARS-CoV-2.
Results also highlight that LTCF staff can be overburdened with information requests during outbreaks. There is a need for efficient and parsimonious data collection tools, using routine sources of intelligence wherever possible, to gather sufficient epidemiological information for the interpretation of environmental surveillance data.
Finally, sampling frameworks focussing on elevated surfaces/those which accumulate particulate matter may be less susceptible to the effects of cleaning regimes and thus a useful tool for detecting outbreaks and evaluating IPC measures.
In summary: this pilot demonstrates the potential utility of surface swabbing in LTCF to assess environmental spread and effectiveness of IPC measures, and monitor for outbreaks of infectious disease. At present, the potential to assess SARS-CoV-2 infection risk via indirect routes is limited by the heterogeneity of LTCFs and their populations, and challenges around data collection.
Data availability
Underlying data
To preserve anonymity of LTCF residents and staff, the study data are stored on a secure drive hosted by Public Health England (PHE) Field Services South West. Access to personal identifiable data is restricted to personnel responsible for outbreak investigations. Non-identifiable data may be made available to others upon formal request (please contact the corresponding author for an information request form) and subject to approval from the PHE Office for Data Release.
Extended data
Open Science Framework: COVID-19: Detecting Indirect Spread in Facilities for Enhanced Care sTudy (COVID-19: DISinFECT). Investigating environmental epidemiology of SARS-CoV-2 in long term care facilities in England. Protocol v4.1. https://doi.org/10.17605/OSF.IO/3QN9Z ( Kwiatkowska & Ready, 2021)
This project contains the following files:
-DISinFECT_Protocol_OSF.pdf. The protocol for this research study.-DISinFECT_staffsurvey.pdf. The electronic survey distributed to staff to collect information on epidemiological and clinical risk factors for SARS-CoV-2 infection.-DISinFECT_Tools_line list_v6.xlsx. The data collection template for LTCF residents: clinical and epidemiological risk factors for SARS-CoV-2 infection.-DISinFECT_Tools_setting log_v2.xlsx. The data collection template for details of LTCF layout and staffing arrangements.
Data are available under the terms of the Creative Commons Attribution 4.0 International license (CC-BY 4.0).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andree BPJ : Incidence of COVID-19 and Connections with Air Pollution Exposure : Evidence from the Netherlands.Policy Research Working Paper; No. 9221. World Bank, Washington, DC. Washington, DC.2020. Reference Source
- 2Ben-Shmuel A Brosh-Nissimov T Glinert I : Detection and Infectivity Potential of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-Co V-2) Environmental Contamination in Isolation Units and Quarantine Facilities. Clin Microbiol Infect. 2020;26(12):1658–62. 10.1016/j.cmi.2020.09.004 32919072 PMC 7481174 · doi ↗ · pubmed ↗
- 3Burton JK Bayne G Evans C : Evolution and Effects of COVID-19 Outbreaks in Care Homes: A Population Analysis in 189 Care Homes in One Geographical Region of the UK. Lancet Healthy Longev. 2020;1(1):e 21–31. 10.1016/S 2666-7568(20)30012-X 34173614 PMC 7574931 · doi ↗ · pubmed ↗
- 4Cherrie JW Cherrie MPC Smith A : Contamination of Air and Surfaces in Workplaces with SARS-Co V-2 Virus: A Systematic Review. Ann Work Expo Health. 2021;wxab 026. 10.1093/annweh/wxab 026 34329379 PMC 8385829 · doi ↗ · pubmed ↗
- 5Conticini E Frediani B Caro D : Can Atmospheric Pollution Be Considered a Co-Factor in Extremely High Level of SARS-Co V-2 Lethality in Northern Italy? Environ Pollut. 2020;261:114465. 10.1016/j.envpol.2020.114465 32268945 PMC 7128509 · doi ↗ · pubmed ↗
- 6Dumont-Leblond N Veillette M Bhérer L : Positive No-Touch Surfaces and Undetectable SARS-Co V-2 Aerosols in Long-Term Care Facilities: An Attempt to Understand the Contributing Factors and the Importance of Timing in Air Sampling Campaigns. Am J Infect Control. 2021;49(6):701–6. 10.1016/j.ajic.2021.02.004 33587983 PMC 7879049 · doi ↗ · pubmed ↗
- 7Goyal SM Anantharaman S Ramakrishnan MA : Detection of Viruses in Used Ventilation Filters from Two Large Public Buildings. Am J Infect Control. 2011;39(7):e 30–8. 10.1016/j.ajic.2010.10.036 21549446 PMC 7132662 · doi ↗ · pubmed ↗
- 8Greenhalgh T Jimenez JL Prather KA : Ten Scientific Reasons in Support of Airborne Transmission of SARS-Co V-2. Lancet. 2021;397(10285):1603–5. 10.1016/S 0140-6736(21)00869-2 33865497 PMC 8049599 · doi ↗ · pubmed ↗