Five-Year Survival Analysis and Causes of Late Deaths of Infants Admitted to the Tertiary Newborn Intensive Care in Latvia
Baiba Balmaka, Sandija Skribāne, Ildze Ābele, Reinis Balmaks

TL;DR
This study examines the five-year survival rates and causes of late deaths in infants admitted to a tertiary NICU in Latvia, finding higher mortality in both premature and term infants.
Contribution
The study provides novel insights into long-term outcomes and late mortality causes in NICU infants in Latvia.
Findings
143 (7.1%) of NICU infants died before 5 years of age.
Premature infants had lower five-year mortality (0.9%) compared to term infants (3.2%).
Common causes of late deaths included congenital heart disease and chromosomal abnormalities.
Abstract
Background and Objectives: Studies on long-term survival following admission to neonatal intensive care units (NICUs) are scarce. The aim of this study was to analyse the epidemiology, five-year survival, and causes of late death of infants admitted to the only tertiary NICU in Latvia. Materials and Methods: The study population included all newborns admitted to the Children’s Clinical University Hospital (CCUH) NICU from 1 January 2013 to 31 December 2017. The unique national identity numbers from the infants or their mothers were used to link the CCUH electronic medical records to the Medical Birth Register and the Database of Causes of Death of Inhabitants of Latvia maintained by The Centre for Disease Prevention and Control of Latvia. Results: During the study period, a total of 2022 patients were treated in the tertiary NICU. The average admission rate was 18.9 per 1000 live births…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
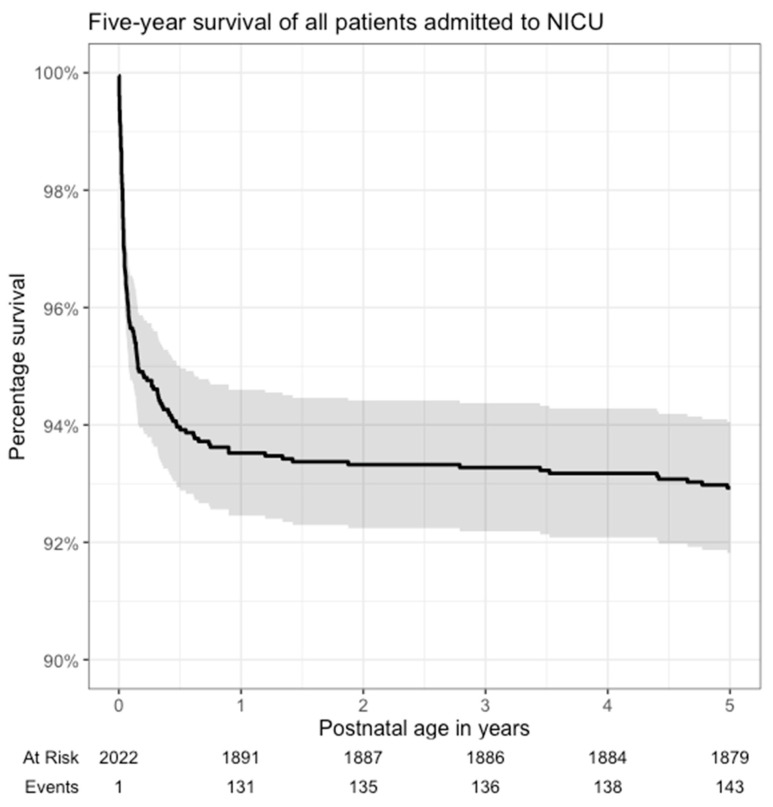 Figure 1
Figure 1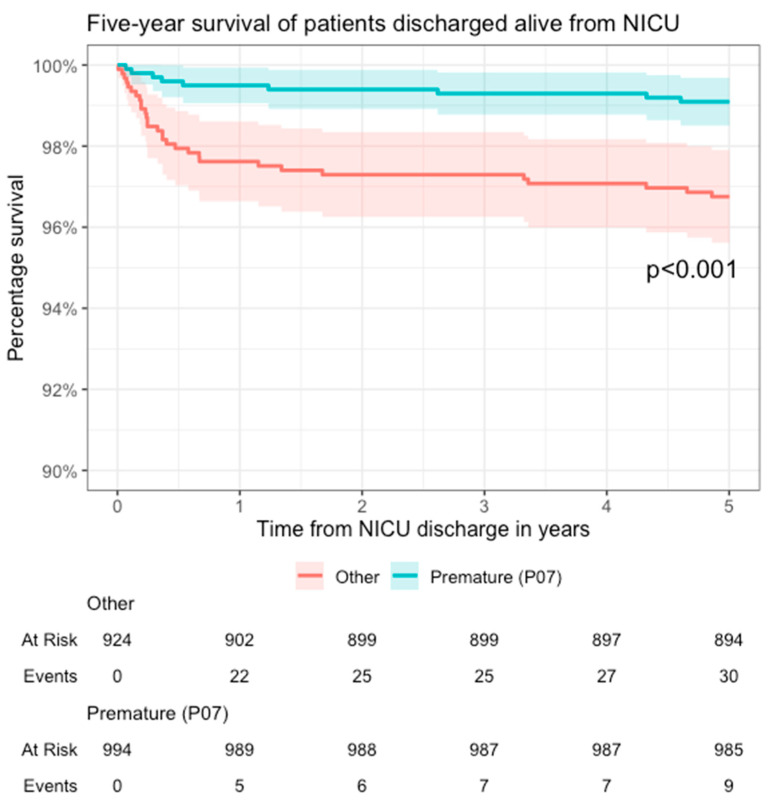 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSocial Sciences and Policies
1. Introduction
Even though neonatal intensive care has been highly effective at improving newborn outcomes, preterm birth remains the leading cause of death in children under five years of age, and neonatal conditions are the leading cause of loss of human capital [1]. Up to 10% of all infants born alive are admitted to neonatal intensive care units (NICU) [2]. The high risk of long-term delayed growth and neurodevelopmental disorders of NICU survivors is well recognized and has led to the establishment of neonatal follow-up programmes [3]. However, less is known about the long-term survival. A recent study from Israel showed that term infants have increased mortality even years after discharge [4]. Overall, studies on the long-term outcomes of neonatal intensive care patients have focused on specific subsets of newborns and lack a population-based perspective. The population-based neonatal (28-day) mortality monitoring programme MBRRACE-UK has allowed identifying regional, social, and ethnic inequalities and thus targeted interventions [5]. The aim of this study was to analyse the epidemiology, five-year survival, and causes of late death of infants admitted to the only tertiary NICU in Latvia.
2. Materials and Methods
In Latvia, all critically ill newborns following birth are transferred to one of six perinatal care centres, one of which is linked to a high-risk obstetric unit. However, intensive care following the sixth day of life (i.e., after a perinatal period) and all paediatric subspecialty and surgical care is provided only at the single tertiary paediatric hospital—Children’s Clinical University Hospital (CCUH). CCUH is a stand-alone paediatric hospital not linked to a delivery ward. The study population included all newborns admitted to the CCUH NICU from 1 January 2013 to 31 December 2017. The unique national identity numbers from the infants or their mothers were used to link the CCUH electronic medical records to the Medical Birth Register and the Database of Causes of Death of Inhabitants of Latvia maintained by The Centre for Disease Prevention and Control of Latvia. Prematurity was defined as any case when at least one of the discharge diagnoses was branched from ICD-10 code “P07” (10th revision of the International Statistical Classification of Diseases and Related Health Problems by the World Health Organization). The population denominators were obtained from the Central Statistical Bureau of Latvia’s publicly available annual reports [6]. All analyses were performed using R software version 4.3.0; the survival package was used for Kaplan–Meier analysis [7]. We used a five-year observation period for each patient; therefore, there were no censored cases.
3. Results
During the study period, a total of 2022 patients were treated in the tertiary NICU. At the same time, 107,117 infants were born alive in Latvia; thus, the average admission rate was 18.9 per 1000 live births per year. One hundred and four patients (5.1%) died in the tertiary NICU before hospital discharge. In the context of the national statistics, 1 of 119 (0.8%) deaths on day of life 0, 25 of 95 (26.3%) from day of life 1 to 6, and 54 out of 74 (73.0%) from day of life 7 to 27 occurred in the tertiary NICU. Of all 288 national neonatal deaths before 28 days of life (2.7 per 1000 live births), 80 (27.8%) were from the study cohort; all before hospital discharge. A total of 131 (6.5%) patients from the study cohort died before 12 months of age and 143 (7.1%) before 5 years of age (shown in Figure 1). Patients with any degree of prematurity had a lower five-year mortality (0.9%, 9 out of 994 discharged alive) than term infants (3.2%, 30 out of 924 discharged alive; p < 0.001) (shown in Figure 2). Of the 39 patients who died after discharge from the NICU, the most common causes of death were congenital heart disease 35.9% (n = 14), multiple congenital malformations and chromosomal abnormalities 17.9% (n = 7), cerebral palsy 10.3% (n = 4), and viral infections 7.7% (n = 3) (Table 1).
4. Discussion
4.1. Major Findings
The NICU admission rate (18.9 per 1000 live births) in our study was low compared to the reported 2.75% to 10% in other population-based studies [2,4], which in our case can be explained by the organization of perinatal care in Latvia. The observed NICU mortality was low; however, only a minority of newborns died in the tertiary NICU. This finding requires an assessment of whether patients need to be transferred sooner to the tertiary NICU, where highly specialized treatments such as neonatal surgery and extracorporeal membrane oxygenation (ECMO) are available. The national neonatal mortality in Latvia (2.7 per 1000 live births) was significantly higher compared to the UK (1.65 per 1000 live births) [5]. Similar to the MBRRACE-UK findings, our results warrant exploration into regional and social inequalities, as our group has previously found significant regional variability in paediatric critical illness and mortality in Latvia [8].
The under-five mortality of 7.1% in the NICU population is significantly higher than the population average of 5.4–11 deaths per 10,000 live births during the same period [6]. The 143 deaths in the study population during the observation period approximate to about one-third of all under-five deaths in Latvia during the study years. Furthermore, the survival curve never reached a stable plateau, indicating how vulnerable this population is. Similarly, a study from Israel showed a 20-fold increased risk for death in term infants following NICU admission even up to 15 years following discharge [4]. In Latvia, NICU follow-up is provided for patients for 2 years; however, globally this practice varies from 2 weeks to 3 years [3]. Our findings could suggest a higher end of this range to prevent late deaths. Moreover, the follow-up should target all NICU patients not only premature patients.
With regard to the causes of late deaths, more than one-third were from congenital heart disease. Previously, our group has demonstrated a low five-year survival of patients with univentricular congenital heart disease in Latvia [9], which reflects difficulties in providing high-quality neonatal heart surgery in a country with a small population.
4.2. Study Strengths
Due to the low migration effect of the Latvian population, the highly centralized tertiary NICU care, and the unique identification number allocated to each mother and child, we were able to cross-link the medical records and national registries and examine long-term follow-up for mortality.
4.3. Study Limitations
There are several significant limitations to the generalizability of these findings. First, the organization of and indications for NICU care may not represent the practice in other countries. Second, we used an administrative dataset with very limited data on obstetric history. Third, the causes of death in some instances were vague (e.g., gastroschisis at age 4). Fourth, we did not analyse other important outcomes such as morbidity, neurodevelopment, and quality of life. Finally, over the last 10 years, several major improvements have been introduced into newborn medicine in Latvia such as the universal adoption of therapeutic hypothermia (2012) and more recently extracorporeal membrane oxygenation (2022). Importantly, the newborn follow-up programme was established in 2015; hence, the data presented in this article are from the pre “follow-up era”, and it is possible that more recent data would demonstrate reduced long-term mortality.
5. Conclusions
By linking medical records with national registries, we were able to analyse a population-based epidemiology of five-year survival following admission to the tertiary NICU in Latvia. Thus, this study adds to the little investigated field of the long-term survival of the general NICU population. Furthermore, we provide insights into the causes of late deaths of tertiary NICU patients. In conclusion, we suggest a longer, up to five years, NICU follow-up programme and investigation of mortality in regional perinatal centres where most neonatal, particularly premature, deaths occur.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Born Too Soon: Decade of Action on Preterm Birth World Health Organization Geneva, Switzerland 2023110
- 2Braun D. Braun E. Chiu V. Burgos A.E. Gupta M. Volodarskiy M. Getahun D. Trends in Neonatal Intensive Care Unit Utilization in a Large Integrated Health Care System JAMA Netw. Open.20203 e 20523910.1001/jamanetworkopen.2020.523932556257 PMC 7303809 · doi ↗ · pubmed ↗
- 3Kang S.R. Cho H. Research Trends of Follow-Up Care after Neonatal Intensive Care Unit Graduation for Children Born Preterm: A Scoping Review Int. J. Environ. Res. Public Health 202118326810.3390/ijerph 1806326833809933 PMC 8004188 · doi ↗ · pubmed ↗
- 4Talisman S. Guedalia J. Farkash R. Avitan T. Srebnik N. Kasirer Y. Schimmel M.S. Ghanem D. Unger R. Granovsky S.G. Neonatal intensive care admission for term neonates and subsequent childhood mortality: A retrospective linkage study BMC Med.2023214410.1186/s 12916-023-02744-736747227 PMC 9903506 · doi ↗ · pubmed ↗
- 5Draper E.S. Gallimore I.D. Smith L.K. Matthews R.J. Fenton A.C. Kurinczuk J.J. Smith P.W. Manktelow B.N. MBRRACE-UK Perinatal Mortality Surveillance, UK Perinatal Deaths for Births from January to December 2021: State of the Nation Report The Infant Mortality and Morbidity Studies Department of Population Health Sciences, University of Leicester Leicester, UK 2023
- 6Central Statistical Bureau Children in Latvia, Collection of Statistics Central Statistical Bureau Kuwait City, Kuwait 2017130 p
- 7Therneau T.M. A Package for Survival Analysis in R. R Package Version 3.5-52023 Available online: https://CRAN.R-project.org/package=survival/(accessed on 1 September 2023)
- 8Setlere L. Vegeris I. Stale M. Balmaks R. Regional Variability of Admission Prevalence and Mortality of Pediatric Critical Illness in Latvia Anesth. Crit. Care 20191152210.26502/acc.003 · doi ↗