Coagulopathy Induced by Antibiotics Usage and Bowel Obstruction With Colon Cancer: Report of a Rare Case
Sho Fujiwara, Ryujiro Akaishi, Tomoki Yokosawa, Hiroshi Suzuki, Toru Hoshida

TL;DR
An elderly woman with bowel obstruction and colon cancer developed coagulopathy due to antibiotic use, which was resolved with vitamin K treatment.
Contribution
Highlights a rare case linking antibiotic-induced vitamin K deficiency to coagulopathy in patients with bowel obstruction.
Findings
Antibiotic administration led to vitamin K deficiency-related coagulopathy in a patient with chronic bowel obstruction.
PIVKA-II was effective in diagnosing vitamin K deficiency in this case.
Discontinuation of antibiotics and IV vitamin K2 resolved the coagulopathy.
Abstract
This case report presents a rare occurrence of coagulopathy induced by antibiotics in a woman in her 90s with chronic bowel obstruction and massive colon cancer. The patient developed vitamin K deficiency-related coagulopathy following antibiotic administration, resulting in bleeding complications. Despite initial consideration of disseminated intravascular coagulation, further investigations revealed antibiotic-induced vitamin K deficiency. Prompt discontinuation of antibiotics and IV vitamin K2 administration led to the resolution of coagulopathy. The case emphasizes the importance of cautious antibiotic use in patients with chronic bowel obstruction and prolonged fasting. The protein induced by vitamin K absence-II (PIVKA-II) proved valuable in diagnosing vitamin K deficiency. The learning points include the potential for coagulopathy with antibiotics in prolonged bowel obstruction…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1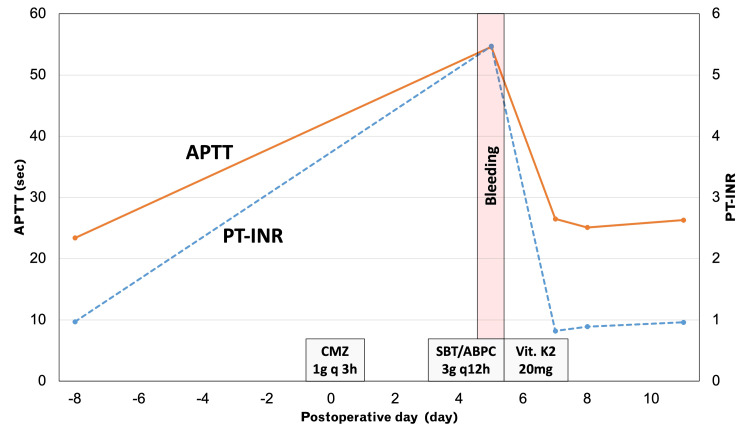 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVitamin K Research Studies · Vitamin C and Antioxidants Research · Renal function and acid-base balance
Introduction
Vitamin K deficiency can lead to coagulopathy in some clinical scenarios. Some major causes of vitamin K deficiency are decreased intake or absorption of vitamin K, altered biosynthesis in intestinal bacteria, and inhibition of liver metabolism [1-3]. Antibiotics with N-methylthiotetrazole (NMTT) side chain could risk vitamin K deficiency by inhibiting vitamin K epoxide reductase like warfarin. In addition, chronic intestinal blockage and fasting for more than seven days can also reduce vitamin K absorption [1]. However, vitamin K deficiency and coagulopathy in adults are rare because adults have enough storage and intake of vitamin K, although it is common in neonates [4]. Here, we present a case of coagulopathy with vitamin K deficiency caused by these multiple risk factors: chronic bowel obstruction due to colon cancer and preoperative use of antibiotics with NMTT side chain.
Case presentation
A female patient in her nineties with a medical history of hypertension presented with vomiting and distension. The symptoms began three days ago, and the family physician prescribed 5 mg of metoclopramide and 330 mg of magnesium oxide orally. However, she was not able to eat well seven days ago. The patient regularly takes 20 mg of esomeprazole for esophageal reflux and 40 mg of telmisartan for hypertension. A physical examination revealed abdominal distension and a palpable tumor in the right lower quadrant. Abdominal contrast-enhanced CT revealed colon cancer invading the terminal ileum and causing bowel obstruction (Figure 1).
Preoperative abdominal contrast-enhanced CTAbdominal contrast-enhanced CT revealed massive colon cancer with invasion of the terminal ileum (yellow arrow) and bowel obstruction.
To palliatively relieve the obstruction, we performed ileocolic side-to-side anastomosis, considering the patient's performance status. During the surgery, we administered prophylactic antibiotic cefmetazole (1 g) intravenously every three hours. Although the patient had a bowel movement on postoperative day (POD) three, she experienced vomiting due to ileus and developed aspiration pneumonia on POD four. Subsequently, the patient was administered 3 g of ampicillin/sulbactam intravenously every 12 hours. On POD five, the patient experienced melena and bleeding from a surgical wound after three administrations of antibiotics. A blood test revealed a prothrombin time and international normalized ratio (PT-INR) of 5.47 and an activated partial thromboplastin time (APTT) of 54.6 seconds (Figure 2).
Time courses of the coagulation testsOn postoperative day five, the patient received 3 g of ampicillin/sulbactam intravenously every 12 hours due to aspiration pneumonia. After receiving three rounds of antibiotics, the patient developed melena and bleeding from a surgical wound.APTT: activated partial thromboplastin time; PT-INR: prothrombin time and international normalized ratio
Initially, we considered disseminated intravascular coagulation (DIC) as the cause of coagulopathy due to bacterial translocation caused by chronic dilated bowel obstruction. However, the platelet count, fibrinogen level, and fibrin/fibrinogen degradation products were within the normal range. Subsequently, we evaluated vitamin K deficiency by examining the protein induced by vitamin K absence-II (PIVKA-II). The patient was diagnosed with antibiotic-induced vitamin K deficiency as PIVKA-II was 33,000 mAU/mL. Consequently, we discontinued the antibiotics and administered IV vitamin K2 20 mg for two days. The coagulopathy improved on POD seven. INR and APTT were within normal range without additional treatment for coagulopathy. Oral taking started on POD 10 and the patient was discharged from our hospital on POD 18 without requiring a blood transfusion.
Discussion
Antibiotic-induced vitamin K deficiency is a rare cause of coagulopathy. The normal reference range of vitamin K is 0.8-5.4 ng/mL and the dietary requirement of vitamin K is 1 μg/kg/day [5,6]. There are several major causes of vitamin K deficiency, including decreased intake or absorption of vitamin K, alteration of vitamin K biosynthesis in gut bacteria, and inhibition of the metabolic cycle of vitamin K in the liver [1]. Metabolic inhibition is induced by cephalosporins with an NMTT side-chain, inhibiting vitamin K epoxide reductase, similar to warfarin. Antibiotics that contain the NMTT or 2-methyl-1,3,4-thiadiazole side chain, such as cefamandole, cefmenoxime, cefoperazone, cefotetan, moxalactam, and cefazolin, inhibit the γ-carboxylation and activation of vitamin K-dependent clotting factors. They also decrease liver microsomal vitamin K-2,3-epoxide activity. These inhibitions can induce coagulopathy in vitamin K deficiency [7].
In this case, ampicillin/sulbactam was considered to be safer than cephalosporins because it does not contain the NMTT side chain [8], but caution should still be exercised due to the lack of oral intake for more than seven days and chronic intestinal obstruction leading to decreased vitamin K absorption [1]. Moreover, the administration of ampicillin/sulbactam can alter the intestinal bacteria. It is important to note that cefmetazole, which was administered as a prophylactic antibiotic, contains an NMTT side chain that could exacerbate coagulopathy [8]. These factors can lead to vitamin K deficiency and coagulopathy. Therefore, administering antibiotics to patients with chronic bowel obstruction, advanced colorectal cancer, and long-term absence of oral intake requires caution. PIVKA-II is a useful tool for evaluating vitamin K deficiencies [9]. If DIC is ruled out and fresh frozen plasma is considered, vitamin K2 should be administered intravenously [10]. There are no reports on whether vitamin K1 or vitamin K2 is appropriate for this case. However, we used vitamin K2 intravenously because vitamin K2 is absorbed from the intestine and produced by intestinal flora. In this case, bowel obstruction and changing microbiota could worsen the vitamin K2 deficiency [11]. Thus, vitamin K2 was supposed to be more appropriate.
Conclusions
Even if we use ampicillin/sulbactam, which does not contain the NMTT side chain, we still need to be careful about vitamin K deficiency if we use antibiotics with the NMTT side chain as a prophylactic for surgery after a long period of bowel obstruction and fasting. To evaluate a deficiency in vitamin K, PIVKA-II can be used. After ruling out DIC and other causes of coagulopathy, the administration of Vitamin K2 should be considered.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The relationship among intestinal bacteria, vitamin K and response of vitamin K antagonist: a review of evidence and potential mechanism Front Med (Lausanne) Yan H Chen Y Zhu H 829304920223551025010.3389/fmed.2022.829304 PMC 9058076 · doi ↗ · pubmed ↗
- 2Acquired vitamin K deficiency as unusual cause of bleeding tendency in adults: a case report of a nonhospitalized student presenting with severe menorrhagia Case Rep Obstet Gynecol Zekavat OR Fathpour G Haghpanah S Dehghani SJ Zekavat M Shakibazad N 4239148201720172892899910.1155/2017/4239148 PMC 5592002 · doi ↗ · pubmed ↗
- 3Vitamin K in neonates: facts and myths Blood Transfus Lippi G Franchini M 49920112108400910.2450/2010.0034-10PMC 3021393 · doi ↗ · pubmed ↗
- 4Hemorrhagic pleural effusion: a rare presentation of vitamin k deficiency in an adult patient Cureus Nwaedozie ST Najjar Mojarrab J Svoboda DC Medani A 012202010.7759/cureus.11374 PMC 772339333312776 · doi ↗ · pubmed ↗
- 5Routine clinical determination of carotene, vitamin E, vitamin A, 25-hydroxy vitamin D 3 and trans-vitamin K 1 in human serum by straight phase HPLC Biomed Chromatogr Van Haard PM Engel R Postma T 798821987350683910.1002/bmc.1130020209 · doi ↗ · pubmed ↗
- 6Dietary intake and adequacy of vitamin KJ Nutr Booth SL Suttie JW 7857881281998956698210.1093/jn/128.5.785 · doi ↗ · pubmed ↗
- 7Association of broad-spectrum antibiotic therapy and vitamin E supplementation with vitamin K deficiency-induced coagulopathy: a case report and narrative review of the literature J Pers Med Matthaiou AM Tomos I Chaniotaki S 13202310.3390/jpm 13091349 PMC 1053318637763117 · doi ↗ · pubmed ↗
- 8Effect of N-methyl-thiotetrazole on vitamin K epoxide reductase Thromb Res Creedon KA Suttie JW 147153441986378756410.1016/0049-3848(86)90130-1 · doi ↗ · pubmed ↗