Quality and Diagnosis on the Lateral View of Pediatric Upper Gastro-Intestinal Series
Shyam Sunder B. Venkatakrishna, Mohamed Elsingergy, Juan S. Calle-Toro, Rebecca Dennis, Hansel J. Otero, Savvas Andronikou

TL;DR
This study evaluates the quality and diagnostic value of the lateral view in pediatric upper gastrointestinal exams, finding that it can help identify duodenum abnormalities but may miss some cases if used alone.
Contribution
The study quantifies the diagnostic accuracy of the lateral view in detecting duodenum redundum and malrotation in children.
Findings
Only 26% of UGI exams had adequate lateral views for interpretation.
23% of adequate lateral views showed the descending staircase sign, corresponding to duodenum redundum.
Using the lateral view alone could lead to a missed diagnosis in one patient.
Abstract
Background: The standard imaging technique for the diagnosis of intestinal malrotation remains the upper gastro-intestinal series (UGIS). The lateral view is promoted as important for making a diagnosis. For this, the lateral view should be of adequate quality, and radiologists must know the normal appearance as well as the appearance of duodenal variants, as misdiagnosis may lead to unnecessary surgery. Objective: We aimed to evaluate the quality, findings including the prevalence of the ”descending staircase” configuration and its correspondence to a diagnosis of duodenum redundum. Materials and Methods: This was a retrospective study and was conducted in a large tertiary children’s hospital in the United States. A retrospective review of UGI fluoroscopy exams in children aged ≤ 18 years between January and December 2018 was performed by a pediatric radiologist. First, the lateral…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
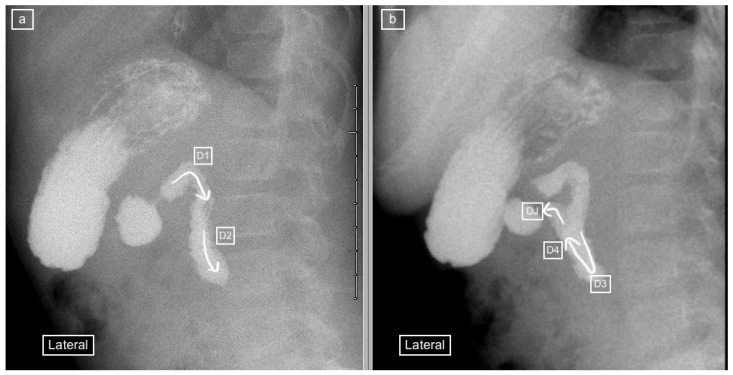 Figure 1
Figure 1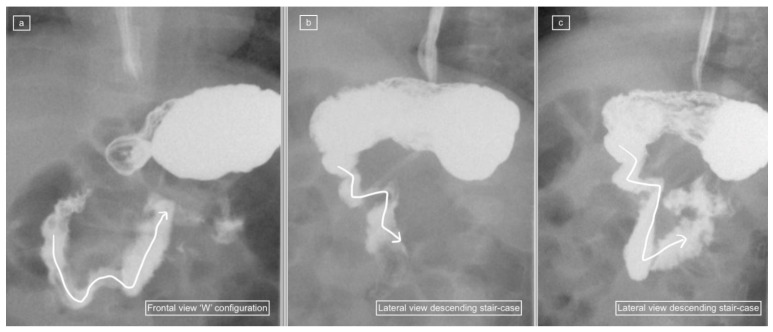 Figure 2
Figure 2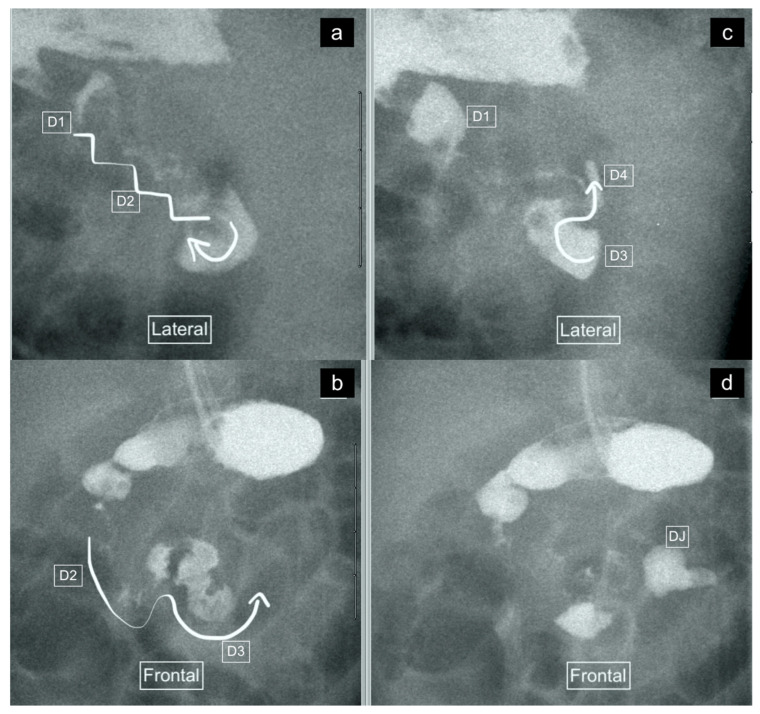 Figure 3
Figure 3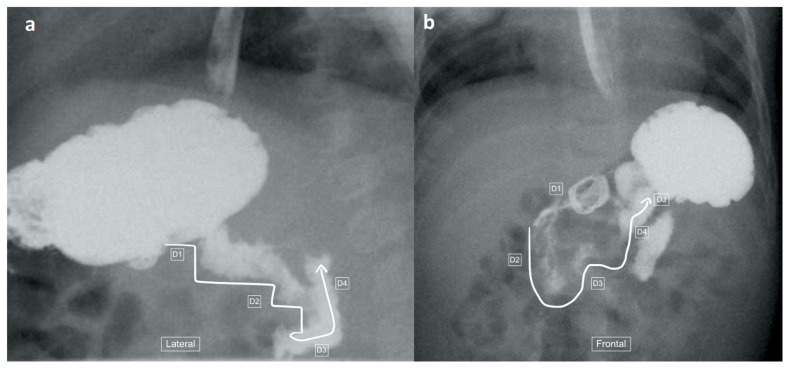 Figure 4
Figure 4 Figure 5
Figure 5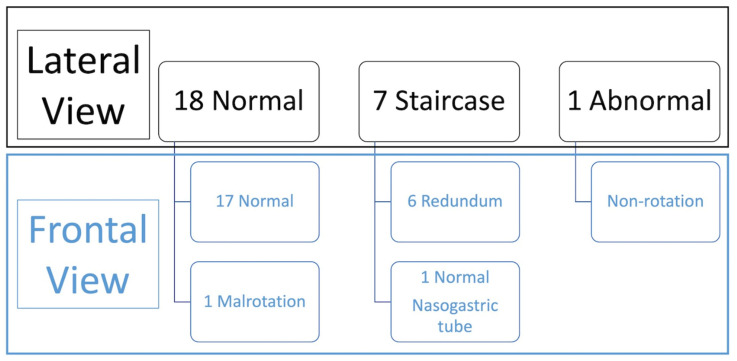 Figure 6
Figure 6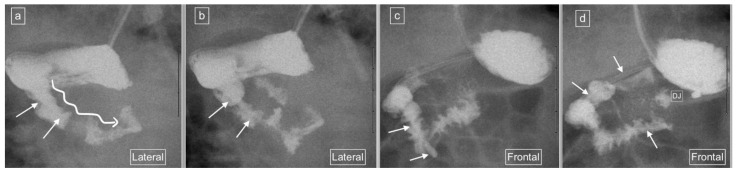 Figure 7
Figure 7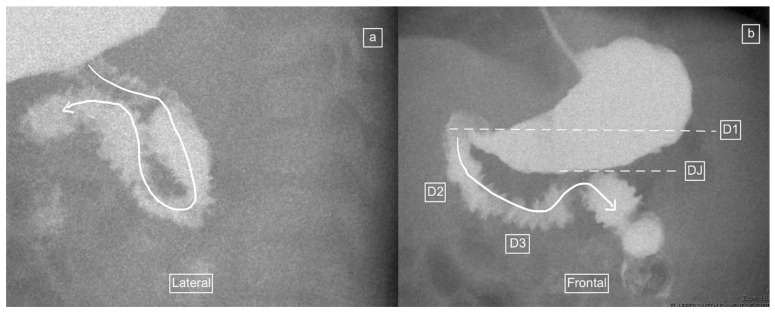 Figure 8
Figure 8Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntestinal Malrotation and Obstruction Disorders · Pediatric Hepatobiliary Diseases and Treatments · Gastrointestinal disorders and treatments
1. Introduction
Despite efforts to move to an ultrasound diagnosis, the standard imaging technique for the diagnosis of malrotation and midgut volvulus in newborns with bilious vomiting remains the fluoroscopically guided upper gastro-intestinal series (UGIS) [1,2,3,4,5,6]. Malrotation is a congenital condition associated with abnormal bowel rotation and can include both small and large intestines. The anomalies can be wide-ranging, from asymptomatic non-rotation to easily diagnosed omphalocele. It is an important condition that needs to be diagnosed on imaging, especially in children presenting to the emergency setting with bilious vomiting, as malrotation predisposes to midgut volvulus with bowel ischemia and potentially significant morbidity and mortality if untreated.
Children are referred to radiologists for demonstration of the duodenal anatomy and diagnosis of malrotation and mid-gut volvulus. The radiologist’s interpretation directly impacts management—patients with normal anatomy are often discharged while those with abnormal duodenal C-loops undergo surgery, sometimes as an emergency [7]. The configuration of the duodenum and position of the duodenojejunal (DJ) flexure on an antero-posterior (frontal) view of the UGIS are most commonly used for diagnosis. Exclusion of malrotation on the UGIS depends on the demonstration of the duodeno-jejunal (DJ) flexure in the correct anatomical position in the left upper quadrant of the abdomen. A diagnosis of malrotation is therefore made if the DJ-flexure is in an abnormal position: (a) overlying or to the right of the left pedicle of 1st lumbar vertebrae; (b) at a more caudal position than the first part of duodenum [8]. A total of 75% of patients with malrotation have one or more radiologic signs, while up to 25% of patients with malrotation have no signs and some reports indicate a false-positive rate up to 15% [8,9].
When performing the UGIS, the radiologist follows a bolus of contrast (the first pass) moving through the duodenum (duodenal C-loop) fluoroscopically [8]. Radiologists routinely place the patient in the right-side-down lateral position to allow gravity to aid a contrast passage from the stomach into the duodenum. However, to achieve the diagnostic image for meeting the above anatomic criteria for excluding or making a diagnosis of malrotation, the patient has to be repositioned into the anteroposterior (AP) view (frontal view)—a maneuver known as the “duodenal roll”, which more often than not results in patient mal-positioning for the most important component of the study. This has been shown to be a common cause for potential false–positive results [7].
Radiologists such as Koplewitz and Daneman have recommended the use of the lateral view for diagnosis, with a posterior retroperitoneal position of the duodenal loop and DJ flexure at the level of the gastric antrum and duodenal cap representing a normal appearance [10], (Figure 1). The lateral position not only allows distinguishing an abnormal anterior from a normal posterior retroperitoneal position of the duodenum but also avoids having to rotate the patient during the study, thereby simplifying the procedure and avoiding missing the important component of the study. However, for the lateral view to be useful, it must be of adequate quality. The quality of the lateral view is often sacrificed in favor of achieving an adequate frontal view during the highly dynamic ”duodenal roll” maneuver. Time is of essence for viewing and capturing the duodenal anatomy because delay in performing the ”duodenal roll” for obtaining the frontal view can lead to contrast flowing into the jejunum with the overlapping intestinal loops affecting the quality and increasing the potential for misdiagnosis [7].
In addition, the presence of duodenal normal variants such as duodenum redundum, may result in misdiagnosis and lead to unnecessary surgery. Duodenum redundum (“redundant duodenum”) and duodenum inversum are the two known normal variants of the duodenum [8,11,12,13]. Duodenum redundum is a normal variant with an elongated third portion of the duodenum resulting in a ”W” or ”WV” configuration of the frontal view. There are no reports of the appearance of duodenum redundum on the lateral view, however, or whether these may mimic pathology. We have anecdotally noted a distinctive ”descending staircase” pattern in cases of duodenum inversum on the lateral view, which deviates from the normal and may be diagnostic but may also be confusing for interpretation of the lateral view.
In this study, we aimed to evaluate the quality and findings on the lateral view of UGIS, including the prevalence of the ”descending staircase” configuration and its correspondence to a diagnosis of duodenum redundum on the frontal view, in a cohort of children imaged with UGIS for suspected malrotation/midgut volvulus.
2. Materials and Methods
This was a retrospective Institutional Review Board (IRB) approved study, compliant with the Health Insurance Portability and Accountability Act (HIPAA), and was conducted in a large tertiary children’s hospital in the United States. A retrospective review of UGI fluoroscopy exams in children aged ≤ 18 years was performed between January and December 2018 by a pediatric radiologist with 24 years of experience in a variety of settings. There was exclusion of patients from the study if they had a history of previous gastrointestinal (GI) surgery (such as Ladd’s procedure) or if they did not have a follow-up clinical examination for confirmation of outcome: (a) surgery for malrotation/volvulus at first presentation or follow-up presentation (classified as abnormal malrotation) or (b) discharge without re-presentation (classified as normal).
The recorded images of the lateral view or cine loops, including the lateral position, were reviewed independently before a review of findings on the frontal (AP) view. Studies were categorized as having ”not captured” or ”inadequately captured” (available but uninterpretable due to inadequate luminal contrast outlining the duodenum on the view) images of the lateral view. We calculated the proportion of studies with adequate lateral views (by excluding the non-captured and inadequately captured cases), and only studies designated to have an adequate lateral view were evaluated further regarding the configuration of the duodenum. This latter subset was then categorized as ”normal”, ”descending staircase”, or abnormal from the lateral view. The descending staircase sign was defined as a stepwise inferior descent of the duodenal course from D1 through D2 oriented posteriorly, after which D3 and D4 ascend in the retroperitoneal position, leading up to the duodeno-jejunal flexure at the same height as D1, before coursing anteriorly (Figure 2, Figure 3 and Figure 4).
The final diagnosis was determined from the frontal view as the standard, and the ”descending staircase” configuration was specifically compared with the AP view for the diagnosis of duodenum redundum.
Imaging Technique
The standard UGI exams in our institution are performed by having the child swallow contrast (usually thin barium), using any one of four methods of administration: bottle, cup, syringe in the mouth or via a nasogastric tube. We avoid overfilling the stomach because a distended stomach can obscure the DJ flexure. We begin with the right-side-down position because gravity can assist with duodenal filling—this position is also used for viewing and recording the lateral duodenal view and identifying a normal posterior and retroperitoneal position of the duodenum. Most radiologists and surgeons require a frontal view for diagnosis, and therefore the child is now required to turn into a supine position on the bed which must be performed rapidly (the ”duodenal roll”) to avoid obscuring important anatomy by contrast flowing into overlying loops of jejunum. We use pulsed fluoroscopy and the recording of a cine loop during the ”duodenal roll”. This is the crucial step of capturing the duodenal “C-loop” during a first pass without overlying contrast in the jejunum. The UGIS in our study were performed by multiple radiologist operators (there were more than 30 pediatric radiologists in our department during the period of the study) who while following this protocol also used individual components to their technique. These diagnostic UGIS reports form the initial clinical diagnostic interpretation for this paper. This technique has been previously published by our group [8].
3. Results
After application of inclusion and exclusion criteria, a convenience sample of 100 studies was selected. Of these, 26 (26%) patients’ UGI exams were designated as having an adequate lateral view for evaluation, (male:16; female:10) with age range of 0 to 16 years (mean age ± SD: 2.8 ± 4.7 years).
Reasons for referral for these 26 studies were: Vomiting reflux—18, Pre-surgical evaluation of duodenal anatomical location—3, Emergency for bilious emesis—1, Congenital diaphragmatic hernia—1, Dysphagia—1, concern for anatomic small bowel obstruction—1, Fussiness—1.
The routes of contrast administration were: Traditional oral route (i.e., contrast swallow)—22, and via nasogastric tube—4.
A total of 18 of the 26 adequate lateral UGI exams (69%) were interpreted as normal, 7/26 (27%) were interpreted as demonstrating the descending staircase configuration (Figure 2, Figure 3 and Figure 4) and 1/26 (4%) was interpreted as abnormal (Figure 5).
Comparison with the AP view was performed (summarized in Figure 6) which demonstrated 2 abnormal exams (1 malrotation and 1 non-rotation), 6 duodenum redundum and 18 normal studies.
Six of the seven lateral views with descending staircase duodenums had duodenum redundum on the AP view and one was reported as normal, but on review contained a naso-jejunal tube in situ, causing distortion of the duodenal anatomy and spasm of the bowel (Figure 7). The single abnormal lateral duodenum was confirmed on AP as a non-rotation (Figure 5). There was one patient with a normal lateral view but malrotation on the frontal view (Figure 8).
4. Discussion
The gold standard imaging examination for the diagnosis of rotational disorders of the midgut has been the UGIS. However, there are several challenges associated with performing UGI examinations reported in the literature [14,15]. These factors can affect the quality of the scan, and include the randomness of the boluses advancing into the duodenum and the repositioning required to obtain an AP view for a diagnosis [14,15]. Exams considered of inadequate quality can lead to non-visualization of the duodenum and DJ flexure, leading to errors in diagnosis. This is because demonstration of DJ flexure in its normal anatomical position is considered essential for exclusion of malrotation on UGI studies [15,16].
The role of the lateral view as a useful adjunct for diagnosing malrotation has previously been published by Koplewitz and Daneman [10]. These authors reported the findings of UGIS in 49 children, out of which 40 had lateral views, and the course of the duodenum on the lateral view could be followed in 27 of these patients, while in 13 patients it was inconclusive [10]. In total, therefore, only 27 of 49 (55%) studies had available and adequate lateral views in the Koplewitz study. Our study had an even lower proportion of 26% of adequate lateral views in UGIS for evaluation. This likely reflects the primary goal of the UGIS for most radiologists being the recording of an adequate frontal view. Despite having only just over half of cases with diagnostic lateral views, Koplewitz and Daneman reported that the lateral view can be a useful adjunct for diagnosis, especially when there is an inconclusive AP view [10]. However, Sizemore et al. reported three cases of false negative (normal) lateral views in patients with malrotation [15] and our own findings include 1 of 26 patients who demonstrated a normal lateral view but had malrotation on the frontal view (Figure 8). These isolated false negative cases suggest that the lateral view should be used with some caution and should not be used in isolation but rather in conjunction with the frontal view, to avoid unnecessary surgery.
Despite the relatively frequent occurrence of duodenal redundancy reported (29% in the study by Sizemore et al. [15]), neither these authors nor any of the other papers reporting and promoting the use of the lateral view refer to the appearance of duodenal variants on lateral views, and whether these cause diagnostic dilemmas such as false positive diagnoses of malrotation. Clinical radiologists should be able to recognize normal variations in order to avoid overdiagnosis of malrotation, resulting in unwanted surgery. We demonstrated a frequency of 23% duodenal variants in our patient population and all of these (100%) demonstrated a characteristic descending staircase sign on the lateral view. However, one case designated as having a descending staircase sign on the lateral view showed a normal duodenum on the frontal view and on review, there is a clear distortion of the duodenum caused by an indwelling naso-jejunal tube with spasm of the bowel. This pitfall is a known potential diagnostic pitfall on the frontal view, which causes malposition of the DJ flexure but is not well documented in the lateral view.
The likely reason that most radiologists do not like to delay the duodenal roll in order to acquire an adequate lateral view is that the delay risks compromising the AP view—reflected by the low rate of adequate lateral views—26% in our sample and 55% in the Koplewitz et al. study [10]. A combination of the lateral view with an AP view can be complementary in supporting the correct diagnosis, with avoidance of ”false positives” and unnecessary surgery. As Long et al. have concluded previously for the frontal view and now shown again for the lateral view, false positives can be avoided by recognizing the variants of normal duodenum [17]. In addition to our recommendation of using the lateral view in conjunction with an AP view for diagnosis, we also recommend (a) an assessment of the lateral view quality before making conclusions, (b) caution when there are indwelling enteric tubes and (c) awareness of the descending staircase sign of duodenum redundum, which represents a variation of normal rather than pathology.
Other imaging techniques for diagnosing malrotation and midgut volvulus include ultrasound, CT and MRI [18,19,20,21], where demonstration of a retroperitoneal duodenum passing the deep [posterior] to the superior mesenteric artery and vein is considered the normal anatomic arrangement. These diagnostic imaging modalities have not gained widespread acceptance. Ultrasound is an obvious choice because of its low cost and lack of ionizing radiation, making it attractive for use in children, as well as its portability, allowing it to be used in the emergency room, in clinics and at the bedside. However, identifying the duodenum passing deep to the superior mesenteric artery (SMA)/superior mesenteric vein (SMV) on ultrasound is challenging or even impossible in some patients due to obscuring bowel gas in the stomach or other portions of the bowel [18]. MRI which also does not use ionizing radiation, may require anesthesia for children under six years of age, which increases the risk, causes delays and is often inaccessible during after-hours when these emergencies present. Using CT to identify the duodenal anatomy has been tested and can be achieved with high reliability, but even though CT scanners are widely available and radiologists of all levels have good expertise with CT, there is a reluctance to apply CT scans in children, due to the perceived risks of radiation [18]. The UGIS therefore remains the mainstay for diagnosing or excluding malrotation and midgut volvulus in children, and any mechanisms for improving the diagnostic yield, such as the use of the lateral view, should be entertained seriously. Recognition of variations of normal on the lateral view therefore becomes more important for the radiologist.
5. Limitations
This is a retrospective study with a small sample size. The imaging reviewed for this study was from DICOM files on PACS, and not from the live fluoroscopy exams, which precludes evaluation of what was seen but not recorded. In addition, there were no other imaging modalities used for comparison with the UGIS exams and patient outcome is assumed to reflect the ground truth where, in fact, patients with malrotation may survive without re-presenting.
6. Conclusions
A total of 26% of UGI studies had lateral views of adequate quality for interpretation. Of these, nearly a quarter (23%) demonstrated the descending staircase sign corresponding to a diagnosis of duodenum redundum on the AP view. Lateral views of the duodenum on UGIS can indeed be useful but as in one of our cases, can also yield false negative results and should be used in conjunction with the frontal view. Obtaining both adequate lateral and frontal views of the duodenum on the first pass presents a challenge, as delay in turning the patient to obtain an adequate lateral view risks compromising the frontal view. Alternative imaging for assessment of the duodenal anatomy should be entertained. However, while the UGIS remains the diagnostic standard, radiologists should be aware of variant duodenum configurations including the descending staircase sign, described in this paper, to avoid misdiagnosis and unnecessary surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Applegate K.E. Evidence-based diagnosis of malrotation and volvulus Pediatr. Radiol.200939(Suppl. S 2)S 161S 16310.1007/s 00247-009-1177-x 19308378 · doi ↗ · pubmed ↗
- 2Strouse P.J. Disorders of intestinal rotation and fixation (“malrotation”)Pediatr. Radiol.20043483785110.1007/s 00247-004-1279-415378215 · doi ↗ · pubmed ↗
- 3Daneman A. Malrotation: The balance of evidence Pediatr. Radiol.200939(Suppl. S 2)S 164S 16610.1007/s 00247-009-1152-619308379 · doi ↗ · pubmed ↗
- 4Tang V. Daneman A. Navarro O.M. Gerstle J.T. Disorders of midgut rotation: Making the correct diagnosis on UGI series in difficult cases Pediatr. Radiol.2013431093110210.1007/s 00247-013-2676-323588775 · doi ↗ · pubmed ↗
- 5Graziano K. Islam S. Dasgupta R. Lopez M.E. Austin M. Chen L.E. Goldin A. Downard C.D. Renaud E. Abdullah F. Asymptomatic malrotation: Diagnosis and surgical management: An American Pediatric Surgical Association outcomes and evidence based practice committee systematic review J. Pediatr. Surg.2015501783179010.1016/j.jpedsurg.2015.06.01926205079 · doi ↗ · pubmed ↗
- 6Girolamo M. Emanuela G. Yu W.M.C. Anna M. Marta P. Grazia C.M. Gandullia P. Arrigo S. Stefano A. Beatrice D.M. Diagnostic accuracy of upper gastrointestinal series in children with suspected intestinal malrotation Updates Surg.2023 ahead of print 10.1007/s 13304-023-01559-837326933 PMC 10806024 · doi ↗ · pubmed ↗
- 7Andronikou S. Arthur S. Simpson E. Chopra M. Selective duodenography for controlled first-pass bolus distention of the duodenum in neonates and young children with bile-stained vomiting Clin. Radiol.201873506.e 1506.e 810.1016/j.crad.2017.12.02029397912 · doi ↗ · pubmed ↗
- 8Calle-Toro J.S. Elsingergy M.M. Dennis R. Grassi D. Kidd M. Otero H. Andronikou S. Frequency of duodenal anatomical variants in neonatal and pediatric upper gastrointestinal tract series (UGI) and the influence of exam quality on diagnostic reporting of these Clin. Imaging 202287283310.1016/j.clinimag.2022.04.00435472665 · doi ↗ · pubmed ↗