Use of veno-venous extracorporeal membrane oxygenation for stabilization prior to redo sternotomy for aortic pseudoaneurysm repair
Anson Y. Lee, Emily L. Larson, Ifeanyi D. Chinedozi, Jennifer S. Lawton, Hamza Aziz

TL;DR
A 62-year-old man with a life-threatening aortic pseudoaneurysm was stabilized with veno-venous ECMO before undergoing successful surgical repair.
Contribution
This case highlights the successful use of veno-venous ECMO to stabilize a patient with respiratory distress due to aortic pseudoaneurysm before redo sternotomy.
Findings
Veno-venous ECMO provided respiratory support in a patient with tracheal compression from an aortic pseudoaneurysm.
The patient underwent successful redo sternotomy and repair of the pseudoaneurysm defect.
A combination of surgical and respiratory strategies enabled successful treatment of a complex case.
Abstract
Background: Aortic pseudoaneurysms are particularly dangerous because of the risk of rupture and compression of mediastinal structures, including the trachea, and resultant respiratory distress. If respiratory distress progresses to respiratory failure, extracorporeal membrane oxygenation may be used to provide oxygenation prior to or during pseudoaneurysm repair. Case presentation: A 62-year-old male with a history of emergent aortic ascending and arch replacement for Stanford Type A dissection 10 months prior presented to his primary care physician with dyspnea. Chest radiography revealed a widened mediastinum, and subsequent computed tomography angiogram revealed a pseudoaneurysm at the distal suture line of the aortic arch replacement. Due to the location of the pseudoaneurysm, the patient’s trachea was compressed, and he was emergently placed on veno-venous (VV) extracorporeal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
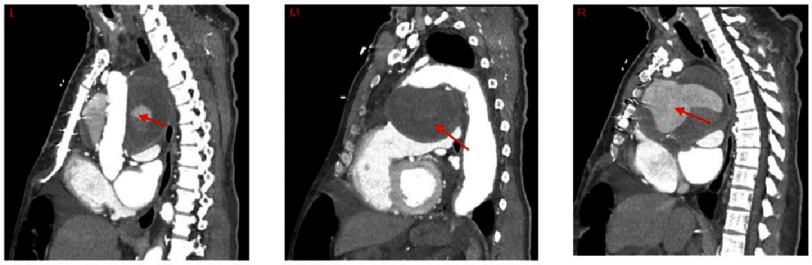 Figure 1
Figure 1 Figure 2
Figure 2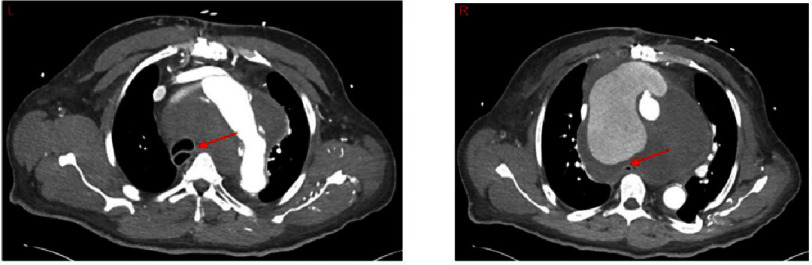 Figure 3
Figure 3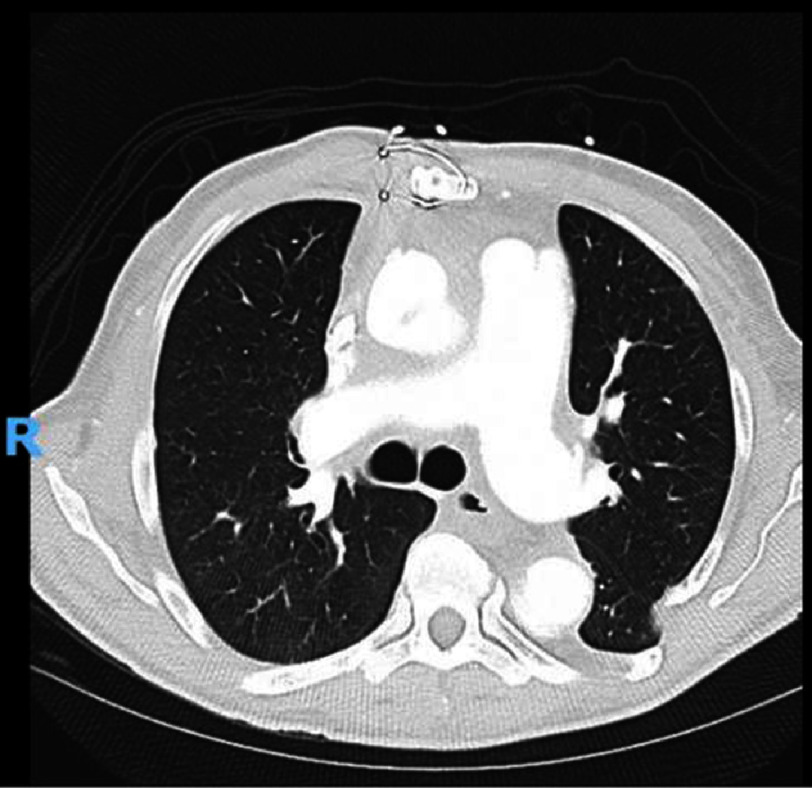 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAortic Disease and Treatment Approaches · Mechanical Circulatory Support Devices · Aortic aneurysm repair treatments
Introduction
Pseudoaneurysms are locally formed hematomas secondary to arterial injury contained by products of the coagulation cascade and do not involve the vessel wall. In contrast, true aneurysms are outpouchings contained by all three layers of the arterial wall^1^. Pseudoaneurysms are commonly associated with catheter-based procedures that can decrease the integrity of the arterial wall, but may also form at the suture lines of arterial repairs^2–8^. Iatrogenic femoral pseudoaneurysms following femoral catheterization are most commonly reported, with aortic pseudoaneurysms being less common^9–12^. Because of this rarity, reports on aortic pseudoaneurysms are primarily limited to case reports and series^13–24^. Patel et al. published a review of multiple single-institution studies in 2014 that specifically analyzed the role of percutaneous closure in these patients. They found that, although percutaneous closure provided satisfactory short-term outcomes, there were associated risks of embolization, device migration, and leaks^25^. For patients in whom percutaneous closure is not an option, endovascular graft placement or open repair remains as an alternative^3,18^.
Aortic pseudoaneurysms pose an additional unique risk of tracheal compression owing to their anatomical location. Thus, respiratory distress and even failure can occur depending on the size and location of the aneurysm. If endotracheal intubation is not possible due to the anatomical location of such aneurysms, ECMO may be required to provide adequate oxygenation^26,27^. However, ECMO is associated with additional operative risks, which may be a barrier to its implementation^28–31^. To the best of our knowledge, no study has reported aortic pseudoaneurysm repair in patients receiving ECMO.
Case report
A 62-year-old male underwent aortic ascending and arch replacement for emergent Stanford Type A dissection 10 months prior to presentation. Additional relevant surgical history included Stanford Type B dissection repair, Crawford type III thoracoabdominal aneurysm repair, abdominal aortic aneurysm repair, and atrial septal defect repair via sternotomy. The medical history included essential hypertension, pulmonary hypertension, chronic diastolic heart failure, and chronic kidney disease.
In the most recent procedure, Stanford Type A dissection began at the ascending aorta, extended into the arch along the lesser curvature, and did not involve the arch vessels. A graft was placed with the distal anastomosis to the proximal descending aorta 1–2 cm proximal to the prior thoracoabdominal graft, with some sections of this anastomosis consisting of a graft-to-graft anastomosis. The proximal anastomosis was two centimeters above the right coronary artery. Additionally, the arch vessels were isolated as island grafts and attached to the arch graft. The patient did well and was discharged on aspirin, atorvastatin, and labetalol.
Ten months later, the patient presented to his primary care physician after experiencing dyspnea for several months. An initial chest X-ray scan revealed a widened mediastinum. Three days later, the patient presented to the emergency department with acutely worsening dyspnea. A computed tomography angiogram (CTA) revealed a pseudoaneurysm at the distal suture line of the aortic arch graft from the prior acute Type A aortic dissection repair which could be viewed in the sagittal (Figure 1), coronal (Figure 2), and axial (Figure 3) planes. The pseudoaneurysm distorted the mediastinal anatomy and compressed the trachea. The aortic pseudoaneurysm also abutted the posterior sternal table. The patient was transferred to the intensive care unit, where he was placed on bi-level positive airway pressure (BiPAP) for poor oxygenation. Over the next 16 h, the patient became more fatigued as PCO2 increased to 87 mmHg. Additionally, he desaturated and became increasingly tachypneic and diaphoretic. Endotracheal intubation was attempted for acute hypoxic respiratory failure, but was unsuccessful. The decision was made to perform emergent venovenous extracorporeal membrane oxygenation (VV ECMO) via bilateral femoral vein cannulation. ECMO flows of 3.2 L/min were achieved with patient stabilization and improved oxygenation.
Sagittal Images of CT scan of a patient on VV ECMO with an aortic pseudoaneurysm at the distal suture line of a prior aortic arch replacement.Left: Large pseudoaneurysm (arrow) behind the aortic graft, compressing the trachea and esophagus posteriorly. Middle: Large pseudoaneurysm below arch (arrow), compressing heart inferiorly. Right: Large pseudoaneurysm (arrow) just posterior to the sternum, compressing the heart inferiorly while compressing the esophagus and trachea posteriorly. Abbreviations: CT - computed tomography, CTA - computed tomography angiogram, VV ECMO - venovenous extracorporeal membrane oxygenation.
Coronal Images of CT scan of a patient on VV ECMO with an aortic pseudoaneurysm at the distal suture line of a prior aortic arch replacement.Left: Large pseudoaneurysm (arrow) with graft anastomosis visible just distal to the left subclavian, left atrium and heart compressed inferiorly. Middle: Large pseudoaneurysm (arrow) leading to compression of the aortic graft. Right: Large pseudoaneurysm compressing the trachea (arrow) with rightward displacement. Abbreviations: CT - computed tomography, CTA - computed tomography angiogram, VV ECMO - veno-venous extracorporeal membrane oxygenation.
Axial Images of CT scan of a patient on VV ECMO with an aortic pseudoaneurysm at the distal suture line of a prior aortic arch replacement.Left: Aortic arch with large pseudoaneurysm and compression and distortion of the trachea (arrow) to the right side. Right: Aortic extravasation of contrast into pseudoaneurysm which can be seen compressing the esophagus (arrow). Abbreviations: CT - computed tomography, CTA - computed tomography angiogram, VV ECMO - venovenous extracorporeal membrane oxygenation.
The following day, the patient required cannula adjustment due to poor flow as low as 2 L/min and PaO2 of 33 mmHg. The inflow and outflow cannulas were adjusted, with subsequent flow improvement to 4 L/min.
The following day, the patient underwent a redo sternotomy and pseudoaneurysm repair. Because the preoperative CT scan of the pseudoaneurysm revealed it was abutting the posterior sternal table, VV ECMO was converted to cardiopulmonary bypass using a peripheral arterial cannula in the right femoral artery. Upon entry into the chest, no identifiable cardiac structures were observed, leading to difficulty in dissecting the right heart border. The decision was made to use deep hypothermic circulatory arrest (HCA) to repair the pseudoaneurysm. After the initiation of HCA (18 °C), the pseudoaneurysm was opened and showed a 2–3 mm defect on the anterior aspect of the distal suture line. Prolene sutures were used to reinforce the suture line. An additional suture was utilized to reinforce the arch vessel island. The patient was weaned from CPB and had profound coagulopathy and hemorrhage, requiring blood product transfusion. The chest was left open and packed owing to coagulopathy and was successfully closed two days later. Postoperative CTA displayed decompression of local structures consistent with resolution of the pseudoaneurysm (Figure 4).
Axial Image of a postoperative CT scan of a patient following the repair of an aortic pseudoaneurysm at the distal suture line of a prior aortic arch replacement on VV ECMO.Axial image of the chest at the level of T7 in a patient following pseudoaneurysm repair 10 months after ascending and aortic arch replacement for acute type A aortic dissection. Mediastinal anatomy and trachea are consistent with resolution of the large pseudoaneurysm. Abbreviations: CT is computed tomography, VV ECMO is venovenous extracorporeal membrane oxygenation.
The postoperative course was complicated by the need for intermittent BiPAP for hypercarbia and hypoxia, as well as diuresis for hypervolemia. The patient progressed well and was discharged home on postoperative day 13.
What we learned
The potential complications of ECMO may deter surgeons from its use in patients with high-risk aortic pathology who present with respiratory distress^28–31^. However, when intubation is not feasible and respiratory failure is inevitable, it can become a necessity. In this case, pseudoaneurysm repair was successful in a patient with preoperative VV ECMO, providing evidence supporting the feasibility of this technique in similarly precarious and high-risk emergencies.
This procedure carried the additional risks of a complex redo operation in a patient with a history of multiple aortic procedures. A previous case report characterized the challenges of redo operations for pseudoaneurysms, including difficulty with sternal entry that may precipitate fatal hemorrhage or air emboli.^32^ Another study noted the risk of stroke, paraplegia, or respiratory failure in redo surgeries of the ascending aorta and aortic arch.^33^ Fortunately, despite this being the patient’s third sternotomy, none of these potential risks occurred.
To our knowledge, this is the first reported case of pseudoaneurysm repair in a patient on preoperative VV ECMO. This success in the face of the extreme operative risk combining ECMO with a redo aortic operation supports the expanded use of ECMO.
Author Statement
Conceptualization
Jennifer S. Lawton and Hamza Aziz.
Writing - original draft
Anson Y. Lee, Emily L. Larson, and Ifeanyi D. Chinedozi.
Writing - review & editing
Anson Y. Lee, Emily L. Larson, Ifeanyi D. Chinedozi, Jennifer S. Lawton, and Hamza Aziz.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Razzouk A Gundry S Wang N Heyner R Sciolaro C Van Arsdell G Bansal R Vyhmeister E Bailey L 1993 Pseudoaneurysms of the aorta after cardiac surgery or chest trauma Am Surg 59128188238256935 · pubmed ↗
- 2Kresowik TF Khoury MD Miller BV Winniford MD Shamma AR Sharp WJ Blecha MB Corson JD 1991 A prospective study of the incidence and natural history of femoral vascular complications after percutaneous transluminal coronary angioplasty J Vasc Surg 1323283351990173 · pubmed ↗
- 3Bossone E Ranieri B Romano L Russo V Barbuto L Cocchia R Pezzullo F Amato C Vriz O Di Tommaso L Iannelli G Czerny M 2020 Acute aortic syndromes: diagnostic and therapeutic pathways Heart Fail Clin 163305315 doi: 10.1016/j.hfc.2020.03.00232503754 · doi ↗ · pubmed ↗
- 4March KL Sawada SG Tarver RD Kesler KA Armstrong WF 1989 Current concepts of left ventricular pseudoaneurysm: pathophysiology, therapy, and diagnostic imaging methods Clin Cardiol 129531540 doi: 10.1002/clc.49601209112676292 · doi ↗ · pubmed ↗
- 5Popovic B Freysz L Chometon F Lemoine J Elfarra M Angioi M Selton-Suty C de Chillou C Aliot E 2010 Femoral pseudoaneurysms and current cardiac catheterization: evaluation of risk factors and treatment Int J Cardiol 14117580 doi: 10.1016/j.ijcard.2008.11.11119095321 · doi ↗ · pubmed ↗
- 6Katzenschlager R Ugurluoglu A Ahmadi A Hülsmann M Koppensteiner R Larch E Maca T Minar E Stümpflen A Ehringer H 1995 Incidence of pseudoaneurysm after diagnostic and therapeutic angiography Radiology 1952463466 doi: 10.1148/radiology.195.2.77247677724767 · doi ↗ · pubmed ↗
- 7Mulder EJ van Bockel JH Maas J van den Akker PJ Hermans J 1998 Morbidity and mortality of reconstructive surgery of noninfected false aneurysms detected long after aortic prosthetic reconstruction Arch Surg Chic Ill 196013314549 doi: 10.1001/archsurg.133.1.459438758 · doi ↗ · pubmed ↗
- 8Maskanakis A Patelis N Moris D Tsilimigras DI Schizas D Diakomi M Bakoyiannis C Georgopoulos S Klonaris C Liakakos T 2018 Stenting of subclavian artery true and false aneurysms: a systematic review Ann Vasc Surg 47291304 doi: 10.1016/j.avsg.2017.08.01328887261 · doi ↗ · pubmed ↗