Correlation between white blood cell count and intestinal resection in patients with acute mesenteric vein thrombosis
Yu Xu, Shang-Tai Dai, Hong-Qiao Lu, Wei Chen, Zhi-Wei Xiong, Jiang Liu, Yong-Jiang Tang, Shi-Kui Guo, Kun-Mei Gong

TL;DR
Higher white blood cell count at admission predicts the need for intestinal resection in patients with acute mesenteric vein thrombosis.
Contribution
Identified white blood cell count as an independent risk factor for intestinal resection in acute mesenteric vein thrombosis patients.
Findings
White blood cell count (AUC = 0.759) was a strong predictor of emergency intestinal resection.
Patients with higher white blood cell counts were more likely to require surgery due to intestinal necrosis.
Leukocyte and neutrophil counts showed significant differences between resection and non-resection groups.
Abstract
Acute mesenteric vein thrombosis (AMVT) is an acute abdominal disease with onset, rapid progression, and extensive intestinal necrosis that requires immediate surgical resection. The purpose of this study was to determine the risk factors for nosocomial intestinal resection in patients with AMVT. We retrospectively analysed 64 patients with AMVT diagnosed by CTA at the Affiliated Hospital of Kunming University of Science and Technology from January 2013 to December 2021. We compared patients who underwent intestinal resection (42 patients) with those who did not undergo intestinal resection (22 patients). The area under the ROC curve was evaluated, and a forest map was drawn. Among the 64 patients, 6 (9.38%) had a fever, 60 (93.75%) had abdominal pain, 9 (14.06%) had a history of diabetes, 8 (12.5%) had a history of deep vein thrombosis (DVT), and 25 (39.06%) had ascites suggested by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
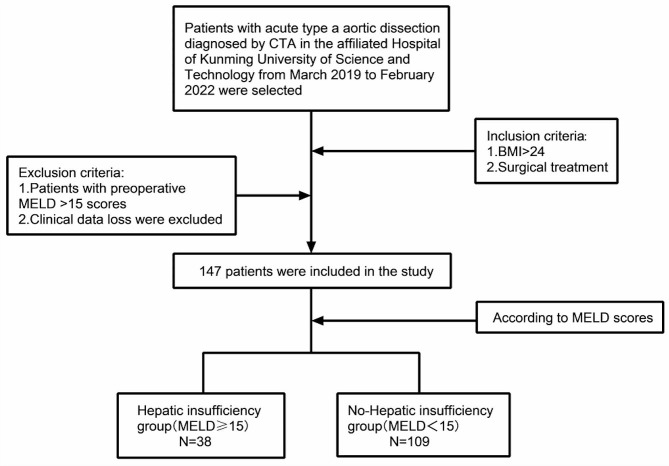 Figure 1
Figure 1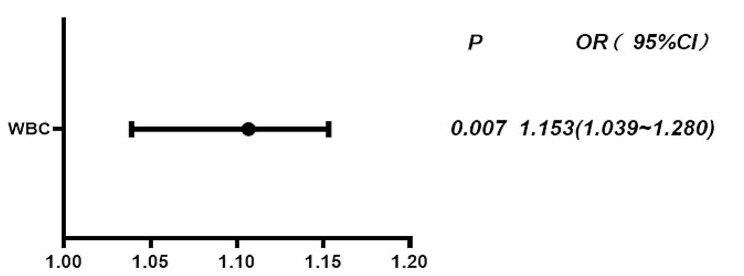 Figure 2
Figure 2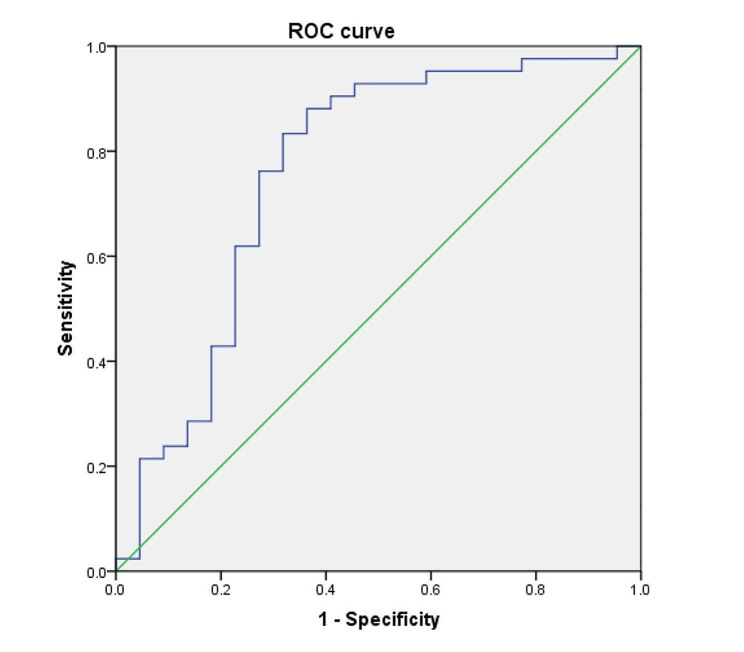 Figure 3
Figure 3- —the Joint Fund of Yunnan Province
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAbdominal vascular conditions and treatments · Liver Disease and Transplantation · Vascular anomalies and interventions
Introduction
Although the mesenteric vein accounts for less than 10% of the intestinal blood supply [1], acute intestinal necrosis is relatively common in the clinic. Septic shock caused by acute mesenteric vein necrosis is still one of the most serious complications, regardless of whether the portal vein is involved in thrombosis [2]. In addition, postoperative intestinal stenosis, short bowel syndrome and other complications also seriously affect the prognosis of patients [3]. According to reports, early active anticoagulation after admission can effectively reduce the incidence of intestinal necrosis [4], and anticoagulation has become a first-line treatment to significantly improve the prognosis of patients with mesenteric vein thrombosis, becoming a necessary condition for successful nonsurgical treatment [5]. The prognosis of patients with acute mesenteric thrombosis is different, and the most important factors leading to death of patients are intestinal necrosis, toxin absorption into the blood, septic shock, and finally death. It is generally believed that intestinal necrosis should be considered when there is an obvious peritoneal stimulation sign, bloody ascites found on abdominal puncture, and general deterioration of the body. Laparoscopic exploration and intestinal resection should be performed immediately to stop the development of the disease. The diagnosis and timely surgical treatment of intestinal necrosis are closely related to the prognosis of patients [6]. The aim of this study was to assess risk factors for patients undergoing emergency enterectomy and to improve survival and outcomes in these patients.
Data and research population
There was a total of 64 patients confirmed by CTA in the Affiliated Hospital of Kunming University of Science and Technology from January 2013 to December 2021, and those who underwent intestinal resection after admission were enrolled as the experimental group (42 patients). A total of 22 patients without intestinal resection (conservative treatment) were used as the control group, the flow chart of the study design is Fig. 1. All patients gave informed consent to the study. The inclusion criteria were as follows: patients confirmed by CTA, and the exclusion criteria was patients with any clinical data loss. This study was approved by the Ethics Committee of the Faculty of Medicine, Kunming University of Science and Technology.
Fig. 1. Flow chart
Data collection
All included patients were divided into the enterectomy group and the conservative treatment group (no enterectomy) according to whether they underwent surgery after admission. The included data included age, fever, abdominal pain after admission, history of hypertension, diabetes, deep vein thrombosis, smoking history, routine blood tests, biochemical tests, and ascites after admission.
Statistical method
SPSS 22.0 was used for data analysis in this study. A t test was used for variables conforming to the normal distribution, a rank-sum test was used for variables not normally distributed, and the chi-square test and Fisher’s probability method were used for categorical variables. The data with P < 0.05 were included in binary logistic regression analysis to obtain the OR value and 95% confidence interval, and a forest map was drawn. An ROC curve was drawn for variables included in the binary logistic regression model to obtain the area under the curve to predict whether patients with mesenteric vein thrombosis need active surgical exploration and enterectomy after admission.
Result
Clinical characteristics
There were a total of 64 patients; 42 patients who underwent enterectomy were included in the experimental group, and 22 patients who received conservative treatment (without enterectomy) were included in the control group. The average age of all patients was 49.85 ± 16.25 years old, 47.71 ± 16.20 years old in the surgery group, and 53.95 ± 15.90 years old in the conservative treatment group. Male patients accounted for 73.44%, 31 patients (48.44%) had smoked before admission, 6 (9.38%) had fever after admission, 60 (93.75%) had abdominal pain, 9 (14.06%) had a history of diabetes, and 8 (12.5%) had a history of deep vein thrombosis (DVT). Twenty-five patients (39.06%) were diagnosed with ascites by B-ultrasound or CT after admission. After admission, a total of 38 patients (59.38%) had white blood cell counts higher than the upper limit of normal value, 6 patients (9.38%) had AST levels higher than the upper limit of the normal value, and 10 patients (15.63%) had abnormal creatinine values. The level of fibrinogen in 42 patients (65.66%) exceeded the upper limit of the normal value, and the DD2 level in 58 patients (90.66%) exceeded the upper limit of the normal value (Table 1).
Table 1. Basic characteristics of all petients included in the studyThe overall(n = 64)Surgery(n = 42)No surgery(n = 22) P Gender (Male/female)47/1729/1318/40.272Age49.86 ± 16.2547.71 ± 16.2053.95 ± 15.900.146Fever (yes/No)6/585/371/220.665Abdominal pain (yes/no)60/439/321/10.574Hypertension (yes/No)8/564/384/180.430Diabetes (yes/no)9/556/363/190.630DVT(yes/no)8/564/384/180.430Smoking history (yes/No)31/3321/2110/120.730WBC (×10^9/L)12.87 ± 7.1316.73 ± 6.679.33 ± 6.760.003Neutrophils (×10^9/L)9.64(4.46, 14.59)11.67(8.19, 14.87)4.43(3.54, 9.62)0.001HGB142(120, 156)143(120, 156)142(120, 155)0.761PLT189(130, 253)189(128, 228)211(137, 270)0.458AST22(16, 29)18(14, 29)24(20, 34)0.048ALT19(14, 32)19(14, 33)18(15, 35)0.635Total bilirubin15.4(11.7, 22.9)16.4(12.6, 27.8)13.4(10.6, 20.3)0.047Direct bilirubin6.8(4.7, 10.6)7.7(5.7, 12.8)6.3(4.3, 7.7)0.064Indirect bilirubin8.8(6.3, 13.0)9.4(7.0, 13.9)7.4(5.4, 11.1)0.066Cr70(61, 89)69(58, 85)72(64, 104)0.164Blood type(A/B/AB/O)21/8/20/1512/4/16/109/4/4/50.337K+4.1(3.8, 4.4)4.1(3.8, 4.4)4.2(3.7, 4.3)0.164Ascites (yes/no)25/3912/258/140.793FIB4.4(3.2, 6.2)5.0(3.9, 6.3)3.9(3.0, 5.2)0.022APTT38.42 ± 4.6638.41 ± 4.7338.43 ± 4.630.984PT14.5(13.6, 153)14.7(13.9, 15.4)13.7(13.5, 15.0)0.090DD212.3(5.1, 19.3)14.5(6.5, 21.8)9.3(2.9, 15.7)0.024
Univariate analysis
The univariate analysis showed that leukocyte count (P = 0.003), neutrophil count (P = 0.001), AST (P = 0.048), total bilirubin (P = 0.047), fibrinogen (P = 0.022), and DD2 (P = 0.024) were significantly different between the enterectomy group and the group without enterectomy.
Multivariate analysis of enterectomy after admission in patients with acute mesenteric vein thrombosis
The multivariate logistic regression analysis showed that admission white blood cell count (OR = 1.153, 95% CI: 1.039–1.280, P = 0.007) was an independent risk factor for enterectomy in patients after admission (Table 2; Fig. 2).
Table 2. Multivariate logistics analysis of emergency enterectomy in AMVT patientsOR95%CI P WBC1.1531.039 ∼ 1.2800.007
Fig. 2. Multivariate logistics analysis -- Forest map
Predictive value of ROC curves and forest map
The ROC curve showed that the AUC of white blood cell count predicting enterectomy for patients after admission was 0.759, the 95% CI was 0.620–0.897, the optimal critical value was 7.815, the sensitivity was 0.881, the specificity was 0.636, and the P value was 0.001. The forest plot showed that the OR value of this study was 1.153, 95% CI: 1.039–1.280, and the P value was 0.007, indicating that white blood cell count was an independent risk factor for enterectomy in patients after admission (Table 3; Fig. 3).
Table 3ROC curve of white blood cell count predicts enterectomy at admission in AMVT patientsAUC95%CI P Optimum critical valueSensitivitySpecificityWBC0.7590.620 ∼ 0.8970.0017.8150.8810.636
Fig. 3ROC curve of white blood cell count predicts enterectomy at admission in AMVT patients
Discussion
The main function of the mesenteric vein is to transport nutrients via small intestine absorption, belonging to the mixed blood. Once there is a mesenteric vein thrombosis, not only is the transportation function damaged, but the patient will also have different degrees of intestinal ischaemia. However, due to the superior mesenteric artery and branch blood vessels that supply the higher intestine [7], patients with intestinal ischaemia have a longer compensatory time. Therefore, the onset of this disease in patients occurs insidiously, and because this disease has the same initial symptoms as other causes of acute abdomen, this condition is often ignored by the first doctor that the patient sees or is even even misdiagnosed, resulting in treatment and diagnostic delay and even death.
At present, overall mesenteric vein thrombosis disease is rare [8] because less than 10% of cases are caused by mesenteric vein thrombosis. The occurrence of intestinal ischaemia in patients with acute mesenteric venous thrombosis requiring emergency surgery mainly lies in whether patients experience peritoneal irritation [9, 10], circulating shock, and bloody ascites [11]. These three aspects, to a certain extent, determine whether patients need surgical treatment after admission. However, no specific biomarkers [12] have been widely used in clinical practice to reflect patients’ systemic inflammation, liver function, kidney function and other biomarkers. This study included 8 years of well-documented clinical data from grade III, GRADE A hospitals and concluded that white blood cell count was an independent risk factor for emergency enterectomy in patients with acute mesenteric venous thrombosis. This feature may have some practical value in future emergency surgical interventions. Thirty-seven of the 42 patients who underwent bowel resection had white blood cell counts above the optimal threshold.
An elevated white blood cell count does not, however, determine the severity of acute abdomen [13]. However, it has been reported that white blood cell count can be an important predictor of intestinal necrosis caused by intestinal ischaemia [14, 15]. In this study, increased white blood cell count was an independent factor associated with intestinal resection in patients with acute mesenteric thrombosis after admission. In the intestinal resection group, 54.76% (23/42) of the patients had an initial WBC count greater than 12.87 × 10^9/L on admission. Although the accumulation of inflammatory factors in the early stage of thrombosis would lead to a slight increase in WBC count, the further increase in WBC count might be caused by further intestinal necrosis and bacterial displacement. An increased WBC count often indicates the further development of the disease, in which the patient would then require emergency exploratory laparotomy or even enterectomy. According to Kim et al. [16], leukocyte levels in MVT patients were associated with intestinal infarction, while Nuzzo et al. [17] also reported that in acute abdomen caused by abdominal pain, an increased leukocyte count should draw attention to intestinal ischaemia and necrosis. In this study, inflammation, blood clotting function, and laboratory indices of liver and kidney function of patients with acute mesenteric venous thrombosis after admission showed no correlation with acute intestinal resection, especially in patients with diabetes who should undergo emergency intestinal resection [18], but these findings have not been confirmed in this study. This may be associated with the research sample size and incorporated into the standard. Further studies are needed to confirm these results.
The arteriovenous reflection principle [19] is confirmed in patients with acute mesenteric venous thrombosis. Venous thrombosis not only leads to bowel ischaemia, which is followed by arterial spasm, but there is a further reduction of the patient’s intestinal blood supply. However, although spasm can prevent the accumulation of interstitial fluid in patients with bowel necrosis, there is an increased amount of insufflate consumption and degradation insufflate blood supply. This principle has been demonstrated in rats [20].
In conclusion, our study found that in patients with acute mesenteric venous thrombosis, the first white blood cell count on admission is closely related to the possibility of intestinal resection surgery. In such patients, bowel and venous ischaemia artery spasm due to irreversible necrosis, as well as bacterial translocation, seems to play a corresponding role in the process, and there should be timely diagnosis to prevent further intestinal necrosis and death.
Conclusions
This study concluded that white blood cell count was an independent risk factor for enterectomy in patients after admission. Early diagnosis, timely detection of intestinal necrosis and timely surgical resection of necrotic bowel are the priorities in the treatment of this disease, which has important positive significance for improvement of life quality of patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bala M Kashuk J Moore EE Kluger Y Biffl W Gomes CA Ben-Ishay O Rubinstein C Balogh ZJ Civil I Coccolini F Leppaniemi A Peitzman A Ansaloni L Sugrue M Sartelli M Di Saverio S Fraga GP Catena F Acute mesenteric ischemia: guidelines of the World Society of Emergency Surgery World J Emerg Surg 2017123810.1186/s 13017-017-0150-528794797 PMC 5545843 · doi ↗ · pubmed ↗
- 2Burch J, Enofe I. Acute mesenteric ischaemia secondary to portal, splenic and superior mesenteric vein thrombosis. BMJ Case Rep. 2019;12(9).10.1136/bcr-2019-230145 PMC 676835531551317 · doi ↗ · pubmed ↗
- 3Lauro A Lacaille F Short bowel syndrome in children and adults: from rehabilitation to transplantation Expert Rev Gastroenterol Hepatol 2019131557010.1080/17474124.2019.154173630791840 · doi ↗ · pubmed ↗
- 4Salim S Zarrouk M Elf J Gottsäter A Ekberg O Acosta S Improved prognosis and low failure rate with anticoagulation as first-line therapy in mesenteric venous thrombosis World J Surg 2018421138031110.1007/s 00268-018-4667-x 29777267 PMC 6182753 · doi ↗ · pubmed ↗
- 5Acosta S Salim S Management of Acute Mesenteric venous thrombosis: a systematic review of Contemporary studies Scand J Surg 20211102123910.1177/145749692096908433118463 PMC 8258716 · doi ↗ · pubmed ↗
- 6Liu D Ye Y Xie Q Yin M Yang X Liang B Wang S[Predictive factors of intestinal necrosis in acute mesenteric vascular occlusive diseases]Zhonghua Wei Chang Wai Ke Za Zhi 20172077879128722092 · pubmed ↗
- 7Corcos O Nuzzo A Gastro-intestinal vascular emergencies Best Pract Res Clin Gastroenterol 20132757092510.1016/j.bpg.2013.08.00624160929 · doi ↗ · pubmed ↗
- 8Kärkkäinen JM Acosta S Acute mesenteric ischemia (part I) - incidence, etiologies, and how to improve early diagnosis Best Pract Res Clin Gastroenterol 2017311152510.1016/j.bpg.2016.10.01828395784 · doi ↗ · pubmed ↗