Synchronous double primary small cell lung cancer and invasive ductal breast carcinoma: a case report
Junqing Gan, Meiyue Liu, Fei Liu, Junxiu Wen, Wenjuan Fu, Jinghao Jia

TL;DR
A 75-year-old woman was diagnosed with two rare cancers at the same time: small cell lung cancer and invasive breast cancer, making this a unique medical case.
Contribution
This is the first reported case of synchronous primary small cell lung cancer and invasive ductal breast carcinoma.
Findings
The patient had a 4.2 cm lung mass confirmed as small cell lung cancer and a 3.8 cm breast lesion diagnosed as invasive ductal carcinoma.
Immunohistochemistry confirmed distinct markers for both cancers, supporting their independent origins.
Brain metastases were detected, leading to a treatment plan involving radiation and chemotherapy.
Abstract
Although lung and breast cancers are common malignancies, the occurrence of primary synchronous neoplasms involving these organs has been rarely reported in literature. A 75-year-old female patient presented at a local hospital with a ten-day history of dizziness and slurred speech. A CT contrast-enhanced scan revealed a 4.2 cm mass in the lower lobe of the right lung and a 3.8 cm space-occupying lesion in the right breast. Subsequent breast ultrasound identified a hypoechoic lesion measuring5.41 × 4.75 × 3.06 cm in the right breast, and an ultrasound-guided biopsy confirmed the presence of infiltrating ductal carcinoma of the right breast. The immunohistochemistry analysis of the breast mass revealed positive staining for ER, PR, HER-2, AR and Ki67 in the tumor cells, while negative staining was observed for P63, Calponin, CK5/6 and CK14. MR imaging of the head detected abnormal…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
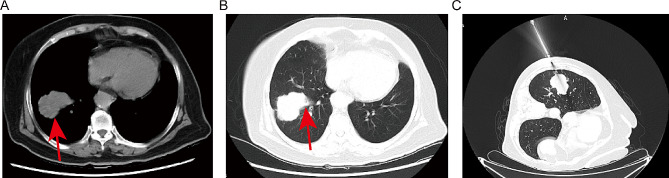 Figure 1
Figure 1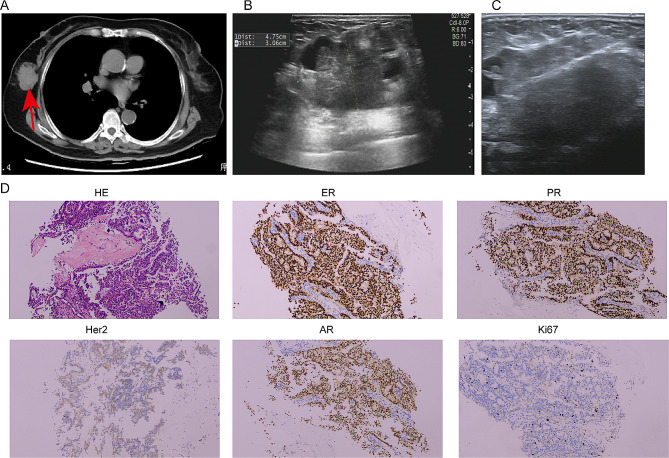 Figure 2
Figure 2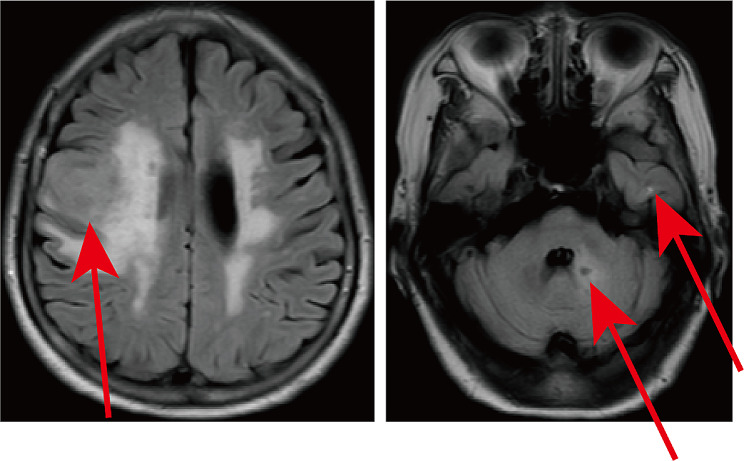 Figure 3
Figure 3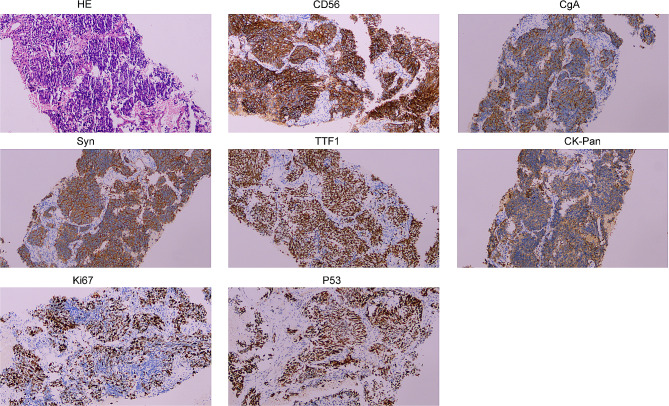 Figure 4
Figure 4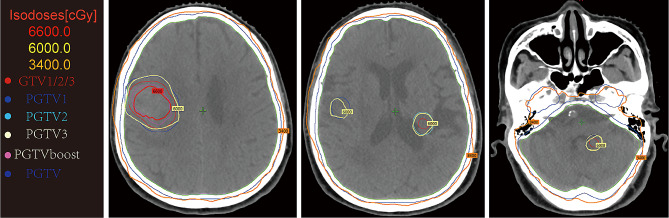 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLung Cancer Research Studies · Lung Cancer Treatments and Mutations · Neuroendocrine Tumor Research Advances
Introduction
Multiple primary malignant tumors (MPMTs) are defined as two or more malignancies with various pathogenic origins detected simultaneously or successively in an individuality [1]. Due to the time interval of diagnosis for the first and second primary tumors, MPMTs can be stratified into synchronous (< 6 months) and metachronous (≥ 6 months) MPMTs [2]. Warren and Gates went a step further by refining diagnostic criteria for MPMTs:(1) each tumor must present malignant, (2) each tumor must be histologically distinct, (3) all tumors must be primary rather than metastases of each other [3]. Much of the increased incidence of MPMTs can be attributed to advances in technology for cancer diagnostics and treatments, which have markedly increased the survival of cancer patients [4]. In a retrospective study that included 1066 patients with breast cancer, 6 were diagnosed with synchronous breast cancer and lung cancer. Among them, 5 cases are lung adenocarcinoma cancers and 1 case is lung squamous cell carcinoma [5]. The present study reports a case of double primary cancer, comprising small cell lung cancer (SCLC), as well as invasive ductal carcinoma of breast (IDC). To our knowledge, a review of literature in PubMed revealed no case similar to ours.
Case presentation
A 75-year-old female patient visited to local hospital with dizziness, slurred speech for 10 days, and then was found to have a space-occupying lesion in right lung by chest CT scanning. For further treatment, the patient was referred to our institution. She lost 5 kg within 10 days, did not smoke and had no family history of malignancy. Physical examination revealed a 5 cm×5 cm mass with tough texture and indistinct borders in right mammary area, while the left nipple and breast showed no abnormal findings grossly. Other systemic examinations were unremarkable. Her past medical history included ten years of cerebrovascular disease and five years of hypertension and coronary heart disease. The vital parameters exhibited values within the established normal range. Laboratory data disclosed complete blood count, liver and kidney function tests were within normal limits. The tumor marker showed raised NSE and CEA while other markers were within normal range (Table 1). CT contrast-enhanced scan showed a mass 4.2 cm in diameter in the lower lobe of the right lung (Fig. 1A-B) and a 3.8 cm space-occupying lesion in right-sided breast (Fig. 2A). The patient underwent CT-guided percutaneous biopsy in the right lung neoplasm (Fig. 1C) and it took a few days to achieve results. Breast ultrasound revealed the presence of 5.41 × 4.75 × 3.06 cm hypoechoic lesion in the right breast and mammary duct ectasia, furthermore, no obvious lymph node enlargement was detected in the two axillary fossa, subclavicular regions and parasternal (Fig. 2B). The histopathological examination of the ultrasound-guided biopsy (Fig. 2C) revealed the presence of tumor cells organized in sheets and nests, exhibiting scant cytoplasm. The nuclei of these cells appeared round or oval, containing granular stippled chromatin and visible nuclear divisions. Notably, no apparent nucleoli were observed, and areas of necrosis were evident. Immunohistochemistry result for breast mass testified strongly positive staining for estrogen receptor (ER) and progesterone receptor (PR) in most tumor cells (3+), 2 + staining for human epithelial receptor 2 (HER-2), 3 + staining for androgen receptor (AR) and 10% positive Ki67 in tumor cells. P63, Calponin, CK5/6 and CK14 was negative in tumor cells (Fig. 2D). Based on the pathological and the immunohistochemical findings, the lesion was regarded as invasive ductal carcinoma (IDC) of the right breast. It was recommended that the patient underwent fluorescence in situ hybridization (FISH) to detect HER-2 status, however, the patient refused the procedure. MR imaging of the head showed abnormal signals in the right frontal lobe (3.6 × 2.9 cm in size), left cerebellar hemisphere, and punctate enhancement in the left temporal lobe, which should be considered for metastasis (Fig. 3). Based on these findings, a provisional diagnosis of IDC with brain metastasis (BM) was made. To alleviate the symptoms, brain focal radiotherapy was delivered. Due to larger right frontal lobe lesion, tumor cells—especially those located in the center of this lesion—often face a severe microenvironment lacking oxygen. Thus, she underwent brain focal radiotherapy, simultaneously high-dose radiotherapy in the center of the foci and prescribed dose was 95%PGTVboost (the center of lesion in right frontal lobe) 66 Gy/3.3 Gy/20fractions; 95%PGTV1(lesion in right frontal lobe) 60 Gy/3Gy/20fractions; 95%PGTV2(lesion in left temporal lobe) 60 Gy/3Gy/20fractions; 95%PGTV3(lesion in left cerebellar hemisphere) 60 Gy/3Gy/20fractions. After 3 days of radiotherapy, pathological findings presented that lung lesions cells were distributed in flaky nest-like shape, arranged densely, with hyperchromatic nuclei, visible areas of focal necrosis, moreover, immunohistochemistry of lung lesions showed positive staining for thyroid transcription factor-1(TTF-1), cytokeratin-PAN (CK-Pan), synaptophysin (Syn), chromogranin A (CgA), CD56, P53 (90%) and Ki67 (70%), and negative staining for NapsinA and P40 in tumor cells (Fig. 4). The findings on pathology and immunohistochemistry suggested SCLC. After discussion, the final diagnosis was SCLC (cT2bN0M1c IVB) with BM, IDC. Whereupon we offered to treat patient with whole-brain radiation (40 Gy/20fractions) and focal radiotherapy (60 Gy/20fractions) and adjuvant concurrent chemotherapy with oral etoposide (50 mg d1-d20). Regretfully, the effect was not observed as the patient refused further therapy and follow-up. Completed dose was 95%PGTVboost 66 Gy/3.3 Gy/20fractions; 95%PGTV1 60 Gy/3Gy/20fractions; 95%PGTV2 60 Gy/3Gy/20fractions; 95%PGTV3 60 Gy/3Gy/20fractions; 95%PTV 34 Gy/2Gy/17fractions (Fig. 5).
Table 1. Laboratory data of tumor markersLaboratory testValueUnitReference rangeAFP2.860ng/ml0–7CA12518.580U/mL0–35CA1537.810U/mL0–25CA1999.540U/mL0–39CA7243.980U/mL0-6.9CEA5.590↑ng/ml0-3.4HCG1.290mIU/mL0–3NSE28.430↑μg/ml0-15.2SCC0.856ng/ml0.5–2.7Note: the arrows indicate the elevated expression
Fig. 1CT scan showed a tumor mass of irregular border in the lower lobe of the right lung. (A) Mediastinal window and (B) lung window showed a right-side lung mass (arrow indicated the location of lesion); (C) The localization needle inserted into the chest wall indicated the needle entry route
Fig. 2. Lesion in the breast. (A) CT scan and (B) breast ultrasound showed a tumor mass in right breast; (C) An ultrasound guided fine needle aspiration (FNA) was performed; (D) Representative HE and IHC positive staining of the primary lesion in right breast. Arrow indicated the location of lesion
Fig. 3MR demonstrated abnormal signals in the right frontal lobe, left cerebellar hemisphere, and punctate enhancement in the left temporal lobe. Arrow indicated the location of lesion
Fig. 4. Representative HE and IHC positive staining of the primary lesion in right lung
Fig. 5. The location of brain tumors from positioning CT images and final excellent dose distribution for each tumor
Discussion and conclusions
Both female breast cancer and lung cancer are highly common malignancies around the world, ranking as the top two cancers in terms of incidence in patients [6]. IDC is the most common type of breast cancer which accounts for 75% of all cases [7]. Furthermore, approximately 15% of lung cancers are SCLC [8]. Wu et al. used the next generation sequencing to detect simultaneous primary lung adenocarcinoma and breast cancer [9]. However, simultaneous detection of SCLC and IDC represents an uncommon event, despite the increasing overall incidence of multiple primary malignant tumors. We present a case of synchronus double primary SCLC and IDC in an old female. To date, no similar case has been reported literature. In the diagnosis of double primary carcinoma, the possibility of tumor metastasis should be excluded. In breast cancer patients with metastatic disease, lung is the common site of metastasis [10]. Moreover, Ali et al. identified 16 metastatic lung tumors to the breast, among which 12 non-small cell lung cancer,1 large-cell neuroendocrine, 1 atypical carcinoid and 2 small-cell carcinomas. Zhao et al. demonstrated a male SCLC with breast mass as the first manifestation [11]. In a number of cases, it is difficult to differentiate between two primary neoplasms or metastatic diseases. In this case study, the malignant features of each tumor were synchronously confirmed by pathological and immunohistochemical examination.
A retrospective cohort study of metachronous second primary cancers demonstrated that uterus, ovary and thyroid were the most frequent sites for developing a second primary cancer after first breast cancer, moreover, thyroid, larynx, mouth/pharynx were the most frequent sites for developing a second primary cancer after first lung cancer [12]. However, a 20-year study verified that lung cancer patients were at higher risk of oesophageal and head and neck cancers comparing to other residents from Queensland [13]. As showed, no exact correlation for predilection site was noted between double primary malignant tumors. Therefore, the possibility of double or multiple primaries should be taken into account when treating patients with multiple tumors.
BM most commonly occur in patients with cancers from the lung and breast, have poor prognosis and high mortality rate, and lack of effective treatment [14]. According to the statistics, BM are a frequent complication in lung cancer patients, presenting in approximately 40% of patients with advanced adenocarcinoma and 50% with SCLC [15]. BM are present at diagnosis in approximately 18% of SCLC at initial diagnosis, and can reach 50–65% of cases within two years [16], moreover, the median survival of SCLC with BM is only 4.9 months [17]. The incidence of BM from breast cancer still following the lung cancer ranks second, accounting for about 10 to 30% [18], and with a median time of BM occurrence 2–3 years after the initial breast cancer diagnosis [19]. SCLC is distinguished by its small size, limited adhesion, and tendency to spread early, resulting in the formation of small primary lesions and significant metastatic lesions [20, 21]. In this particular case, a higher level of ki67 expression (70%) suggests a heightened degree of malignancy within the tumors. Additionally, MR imaging reveals the presence of multiple brain metastases, with larger instances measuring up to 3.6 × 2.9 cm. Shi et al. found that cerebellar hemisphere was a high-risk brain region in the SCLC [22]. Breast ultrasound revealed no obvious lymph node enlargement was detected in the two axillary fossa, subclavicular regions and parasternal. Immunohistochemistry result for breast mass testified strongly positive staining for ER and PR in most tumor cells (3+) and 10% positive Ki67 in tumor cells. The biomarker Ki67 is routinely used for assessing the proliferative index of primary breast cancer tissue and is the single most important prognostic factor for breast cancer brain metastasis [23]. In summary, we consider that the patient has a high possibility of SCLC with BM. The final diagnosis was SCLC (cT2bN0M1c IVB) with BM, IDC.
Currently, no clear and unified clinical treatment guideline for synchronous primary cancers has been developed [17]. Surgery remains the primary treatment option [24]. However, palliative care was ultimately implemented due to the following factors: Firstly, the patient presented a medical history encompassing hypertension, coronary heart disease, and cerebrovascular disease, alongside current symptoms of dizziness and slurred speech, rendering them unsuitable for surgical intervention. Secondly, MR findings indicated the presence of multiple brain metastases and a suboptimal response to dehydration treatment. Lastly, the patient explicitly declined surgical intervention. The aims of palliative therapy were to control local tumor growth and ease and improve symptoms, while improving and preserving the patient’s quality of life. We finally formulated whole-brain radiation (40 Gy/20fractions) and focal radiotherapy (60 Gy/20fractions) and adjuvant concurrent chemotherapy with oral etoposide treatment plan due to following reasons:1) many breast cancers had a slow disease progression and relatively good prognosis [25]; however, SCLC is life-threatening due to its rapid progression [26]. So, the chemotherapy that targets the two tumors and concentrates on the most aggressive seems the most reasonable treatment.2) First-line standard chemotherapy for patients with SCLC is a combination of etoposide with platinum [27]. However, patient may be unable to tolerate intensive chemotherapy due to severe dizziness. Furthermore, the compliance of patients is relatively poor. Meanwhile, etoposide is chemotherapeutic agents extensively used to treat a wide spectrum of solid tumors (including breast cancer) [28]. In addition, oral etoposide increases the sensitivity of tumor cells to radiation therapy [29]. Single-agent etoposide is thus considered a most suited for treatment option.3) Before lung biopsy pathology were reported, we initially diagnosed breast cancer with BM, so focal radiotherapy was given to alleviate dizziness. Due to larger right frontal lobe lesion, tumor cells—especially those located in the center of this lesion—often face a severe microenvironment lacking oxygen. Thus, she underwent brain focal radiotherapy, simultaneously high-dose radiotherapy in the center of the foci. When lung biopsy pathology later confirmed primary SCLC, the diagnosis was revised to SCLC with BM. Whole-brain radiotherapy (WBRT) has remained the standard of care for patients with BM from SCLC [30]. Therefore, we finally proposed a treatment plan of whole-brain radiation and focal radiotherapy.
In summary, this manuscript was reported about an extremely case of simultaneous double primary SCLC and breast cancer. Although the case is very rare, when imaging examination reveals a mass in other organs, the possibility of a new primary tumor rather a metastase of the initial primary tumor for these patients must be seriously considered. The combination of tumor markers analysis, imaging findings and clinical characteristics may be helpful to determine an accurate preoperative diagnosis, but the final diagnosis should be dependent on the pathological and immunohistochemical examination. Given that it is a rare disease, consensus on effective therapy is unavailable and remains to be further investigated.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Liu Z Jin C Zhang Y Jiang Y Wang J Zheng L Identification of BRAF, CCND 1, and MYC mutations in a patient with multiple primary malignant tumors: a case report and review of the literature World J Surg Oncol 202321115810.1186/s 12957-023-03036-337221610 PMC 10207802 · doi ↗ · pubmed ↗
- 2Nyqvist J Parris TZ Helou K Sarenmalm EK Einbeigi Z Karlsson P Nasic S Kovács A Previously diagnosed multiple primary malignancies in patients with breast carcinoma in Western Sweden between 2007 and 2018 Breast Cancer Res Treat 20201841221810.1007/s 10549-020-05822-z 32740808 PMC 7568709 · doi ↗ · pubmed ↗
- 3Zhai C, Cai Y, Lou F, Liu Z, Xie J, Zhou X, Wang Z, Fang Y, Pan H, Han W. Multiple primary malignant tumors - a clinical analysis of 15,321 patients with malignancies at a single center in China. J Cancer. 2018;9(16):2795–801.10.7150/jca.25482 PMC 609636030123347 · doi ↗ · pubmed ↗
- 4Xia Q Zhao LY Yan YD Liao Y Di YS Xiao XYA multiple primary malignancy patient with FANCA gene mutation: a Case Report and Literature Review Front Oncol 202010119910.3389/fonc.2020.0119932850347 PMC 7420727 · doi ↗ · pubmed ↗
- 5Shoji F Yamashita N Inoue Y Kozuma Y Toyokawa G Hirai F Ito K Tagawa T Okamoto T Maehara Y Surgical Resection and Outcome of Synchronous and Metachronous primary lung Cancer in breast Cancer patients Anticancer Res 20173710587162898291410.21873/anticanres.12032 · doi ↗ · pubmed ↗
- 6Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: Cancer J Clin. 2021;71(3):209–49.10.3322/caac.2166033538338 · doi ↗ · pubmed ↗
- 7Chang KC Diermeier SD Yu AT Brine LD Russo S Bhatia S Alsudani H Kostroff K Bhuiya T Brogi E Ma TAR 25 lnc RNA regulates the Tensin 1 gene to impact breast cancer progression Nat Commun 2020111643810.1038/s 41467-020-20207-y 33353933 PMC 7755919 · doi ↗ · pubmed ↗
- 8Alam SK Wang L Ren Y Hernandez CE Kosari F Roden AC Yang R Hoeppner LHASCL 1-regulated DARPP-32 and t-DARPP stimulate small cell lung cancer growth and neuroendocrine tumour cell proliferation Br J Cancer 202012358193210.1038/s 41416-020-0923-632499571 PMC 7463034 · doi ↗ · pubmed ↗