Pharmacists’ Attitudes towards Medically Assisted Dying
Lun Shen Wong, Shane L. Scahill, Emma Barton, Bert Van der Werf, Jessica Boey, Sanyogita (Sanya) Ram

TL;DR
This study explores New Zealand pharmacists' attitudes and willingness to support medically assisted dying under the End of Life Choice Act.
Contribution
The study provides new insights into pharmacists' perspectives on medically assisted dying, highlighting key factors influencing their support and participation.
Findings
Most pharmacists supported legally assisted medical dying (58%), while 29% did not support it.
Religion was identified as the most significant factor influencing lack of support or willingness to participate.
Participants cited legal and ethical considerations as primary influences on their attitudes.
Abstract
Aims: We aimed to explore pharmacists’ attitudes and support toward medically assisted dying (MaiD) through the End of Life Choice Act 2019 (EOLC), their willingness to provide services in this area of practice, and the influences on their decisions. Methods: The study was conducted via an anonymous, online QualtricsTM survey of pharmacists. Registered New Zealand pharmacists who agreed to receive surveys from the two Schools of Pharmacy as part of their Annual Practicing Certificate renewal were invited to participate through an email with a Qualtrics URL link. The survey contained questions regarding demographics, awareness, knowledge, support for, and attitudes and willingness to participate. Results: Of the 335 responses received, 289 were valid and included in the analysis. Most participants supported legally assisted medical dying (58%), almost a third of participants did not…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
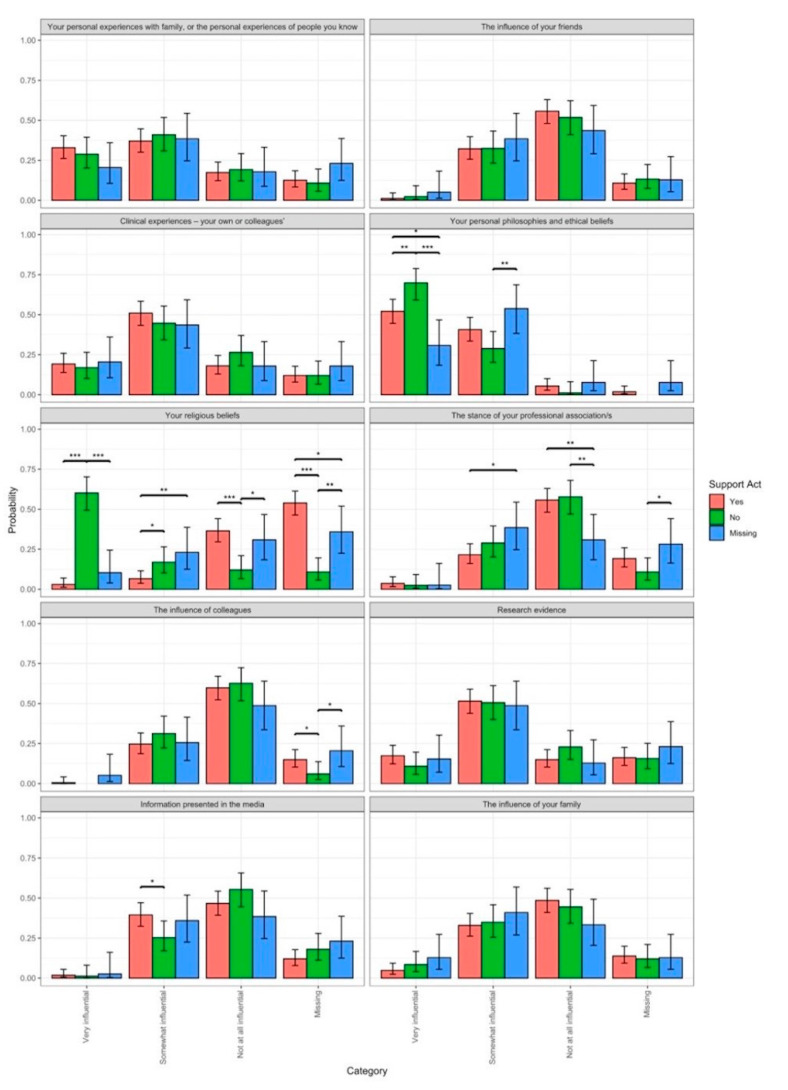 Figure 1
Figure 1- —New Zealand Pharmacy Education Research Foundation (NZPERF)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPalliative Care and End-of-Life Issues · Grief, Bereavement, and Mental Health · Patient Dignity and Privacy
1. Introduction
Pharmacists are expected to play an integral role in optimising medication therapy, improving health literacy and access to medication to improve health outcomes. Pharmacists can play a vital role in improving quality of life at the end of a patient’s life. Pharmacists’ roles have extended to being involved in the provision of medically assisted end-of-life care in a number of jurisdictions, including the Netherlands, Canada, and Australia [1,2,3].
In New Zealand, the End of Life Choice Act 2019 (EOLC) came into effect on the 1st November 2021. This is the first legislative change of its kind in the New Zealand context, so its application across the health sector, implementation, and analysis of uptake are still in their infancy stages; much is unknown, including the level and expectation of pharmacist participation. The EOLC requires health professionals and all New Zealanders to navigate implementation and reflect changes in societal norms. This legislation gives a person suffering from a terminal illness the ability to lawfully request medical assistance to end their life [4]. In the Act, assisted dying, in relation to a specific person, is defined as “the administration by an attending medical practitioner or an attending nurse practitioner of medication to the person to relieve the person’s suffering by hastening death; or the self-administration by the person of medication to relieve their suffering by hastening death” [4].
Societal norms and the acceptance of medically assisted dying (MaiD) in a multi-cultural society highlight the potential for ethical tensions surrounding conscientious objection (CO) and the rights of healthcare professionals to determine the care they envision they will provide. While officials contend with establishing and implementing the safeguards and processes outlined in the Act, healthcare professionals have also grappled with the practicalities of implementing the law within their realm of practice and navigating the intricacies of balancing CO with reasonable limits, both individually and as a profession [5,6].
The Act ensures that any practitioner who is authorised or needed to do anything under the requirements can conscientiously object and is not required to provide the service [7]. However, they must inform the person being assisted of their objection and refer them to an alternative practitioner who can provide the service in a timely manner. Personal autonomy, private conscience, morals, and personal values are not usurped, as individuals still take responsibility for their decisions. This decision-making process should be supported by their profession’s frameworks, professional standards, and accepted norms [7]. Pharmacists, like other healthcare professionals, are not devoid of personal conscience [8] and may opt out of providing end-of-life service. Person-centred care helps provide a way forward in balancing the duality of private conscience and public role expectations, where patients and healthcare providers tolerate each other’s diverse viewpoints [9]. Since the implementation of MaiD in New Zealand, pharmacist engagement with this service has been limited due to legislative boundaries; however, as further implementation occurs and learnings materialise and professional scopes proliferate, this may not remain so.
The professional guidance for navigating CO, particularly in the context of MaiD, varies between countries. The Pharmacy Council of New Zealand (PCNZ) Code of Ethics does not include a definition of CO; however, the expected approach to service provision is outlined under Principle 4 [10]. The Pharmaceutical Society of Australia Code of Ethics defines conscientious objection as “a practitioner’s refusal to engage or provide a service primarily because the action would violate their deeply held moral or ethical value about right or wrong”. Both regulatory bodies expect those with a CO to ensure that patients are able to access the required care [8,11].
A mapping review of the literature, conducted by Woods et al., reported that most of the research exploring pharmacist involvement in MaiD focused on pharmacists’ attitudes, and opinions concerning assisted dying [12]. Few studies have focused on pharmacists’ experience with MaiD or their willingness to participate. This study aims to explore pharmacists’ attitudes towards MaiD, their willingness to provide services in this area of practice, and what the influences on their decisions are.
The aims of the study are to:
- Investigate NZ pharmacists’ awareness of and influences on their attitudes toward legalising medically assisted dying under the End of Life Choice Act 2021.
- Investigate pharmacists’ willingness to provide services consistent with the End of Life Choice Act 2021.
2. Methods
The study was conducted via an online Qualtrics^TM^ (Sydney, Australia) survey of pharmacists in New Zealand. Registered New Zealand pharmacists working in the pharmacy sector who have agreed to receive surveys from the Schools of Pharmacy as part of their Annual Practicing Certificate renewal were invited to participate through an email with a Qualtrics™ URL link. There were approximately 3000 pharmacists on this list. The survey was also circulated through pharmacy professional leadership organisations from the end of September until November 2021. This was prior to the EOLC Act coming into force. At this time, the role of pharmacists was ambiguous in how the proposed service would translate into practice.
The survey contained five sections. Section A collected participant demographics, Section B focused on awareness of the End of Life Choice Act 2019, Section C explored attitudes towards MaiD and factors that influenced participants’ views. Section D explored willingness to participate in the provision of EOLC services. Section E explored the psychosocial variables that affect the behaviours of pharmacists in relation to facilitating MaiD. Section C was adapted from a questionnaire exploring physicians’ and nurses’ experiences of MaiD [13,14]. These questions were adapted from a survey of nurses using the framework of the Theory of Planned Behaviour (TPB) to explore responses to requests for assisted dying, with permission from the researchers [14]. The survey was adapted for pharmacists and to suit the New Zealand environment and regulations. The survey was reviewed by three pharmacists with knowledge of the Act and piloted amongst eight pharmacists.
This manuscript is focused on sections A to D of the survey by presenting results on attitudes towards, influences, and willingness to participate in MaiD.
The study was approved by the University of Auckland Human Participants Ethics Committee on 10 September 2021. Reference Number: UAHPEC22554.
Data analysis was undertaken using the IBM Statistical Package for the Social Sciences (IBM SPSS^TM^ version 19) analytical software and R version 4.3.0 [15]. Descriptive statistics were generated to explore frequency data according to participant characteristics [16]. The multinomial answers were analysed with a logistic regression using the R package lme4 [17]. The assumptions behind the regression were checked with the R package DHARMa [18]. Different models were compared using the Akaike Information Criterium (AIC) [19]. Subsequent pairwise comparisons were made using the parameter estimates and covariances of the best-fitting model. To hypothesise causality between the variables, the R package bnlearn was used to conduct a Bayesian network analysis [20].
Participants’ open text comments were reviewed and categorised into themes using an inductive method [21]. The process involved becoming familiar with the data, then producing codes methodically across the dataset, searching for overarching themes, and creating an index of subthemes. These were tabulated and appraised in investigation team meetings to assess consistency across the dataset. Themes were justified by the investigation team via peer debriefing and critique in research team meetings [21].
3. Results
Of the surveys disseminated via the pharmacist regulator emailing list (n = 3039), 335 responses were received (11% return rate). Of these, 289 responses (9.5% response rate) were valid due to full survey completion and included in the analysis. The distribution of respondents by role and sector included: community pharmacists (n = 120, 35.8%), community pharmacy owners (n = 62, 18.5%), hospital pharmacists (n = 63, 18.8%), and community pharmacy managers (n = 27, 8.1%). In 2021, community pharmacists comprised the majority of pharmacists (78%), and hospital pharmacists were the minority (1%) [22]. These are reflected in the results of this study.
Just over half (58%) supported legalising medically assisted dying; almost a third of participants did not support (29%), and 13% of respondents were unsure (see Table 1). Just over half of the participants by gender, 55% (n = 109) female and 65.9% male (n = 33), supported the EOLC Act.
Around half (51%) reported having “skim read” the Act. Less than one-fifth (16%) stated that they had read the Act in some detail. Participants reported being somewhat knowledgeable (51%) on the Act, with 22% rating their knowledge as knowledgeable or very knowledgeable. Most participants (83%) had not attended any training related to the Act or its service provision; nevertheless, they had read generally about the proposed medically assisted dying services.
Participants first learned of the EOLC Act mostly through the media (n = 131, 45.3%) and the promotion of the EOLC referendum (n = 100, 34.6%). Less than 10% were notified about the EOLC Act by their professional pharmacy organisations (n = 22, 7.60%) or by the internet (n = 11, 3.80%). Participants also learned about the EOLC Act through family members (n = 4, 1.4%), friends (n = 8, 2.8%), or social media (n = 1, 0.30%). Some participants learned about the Act through scientific literature (n = 2, 0.70%) and through other means (n = 10%, 3.5%).
Participants were asked how influential a list of factors, such as religious beliefs, clinical experiences, personal philosophies and ethical beliefs, the stance of professional organisations, and the influence of colleagues, family, and friends, had been in shaping their views towards medically assisted dying. Figure 1 outlines the perceived influences compared to their support for legalising MaiD.
A multinomial logistic regression was conducted to explore whether the factors of influence differ across levels of support for legalising medically assisted dying (MaiD). There was significant evidence to support differences in mean factors of influence (p < 0.05). Post hoc comparisons showed that participants who stated that their personal beliefs and ethical beliefs were very influential were more likely not to support legalising MAiD. There were differences among those participants who found their religious beliefs influential, somewhat influential, or not at all influential. Those who were influenced by religious beliefs did not support legalising MAiD; however, those who were not influenced by religion were supportive of legalising MAiD. There was much missing information or participants who were unsure, and these participants presumably did not identify with being religious and indicated support for legalising MAiD. Those participants who were not influenced by the stance of a pharmacy professional organisation differed from those who were missing information and unsure, presumably due to not belonging to a professional organisation. Those that were somewhat influenced by the media were more likely to support legalising MAiD than those who responded with no to this question.
The decision to not support legalising medically assisted dying was influenced by religious beliefs. A Bayesian network analysis indicated that pharmacists’ willingness to participate in the provision of medically assisted dying consistent with the EOLC was influenced by religious beliefs. The influence of friends, professional leadership organisations, the media, and colleagues was not statistically significant. Pharmacists also noted that organised religion and suicide were emerging concerns relating to legalising medically assisted dying. Pharmacists commented that their religion or beliefs could shape their view of the legislation, and many were not able to separate this bias from their views.
3.1. Other Factors Shaping Participants’ Views towards Legalising Medically Assisted Dying
A diverse range of factors were reported to shape participants’ views of EOLC service provision. Themes of influence around service provision include criminality, palliation, vulnerability, suffering and indignity, and autonomy, as shown in Table 2.
Text analysis of pharmacist quotes demonstrated that professional pharmacy organisations and indemnity providers could influence pharmacist views around this service, despite there being no statistically significant difference through pairwise comparison. Participants’ experience as health professionals and the context of the types of patients they worked with could also affect their perception of medically assisted death.
Some respondents noted that culture and access to appropriate services could affect indigenous populations, such as Māori, disproportionately. The role of equity in access to this service is a consideration some pharmacists contemplated when forming their views about legalising end-of-life care.
3.2. Main Concerns around Legalising Medically Assisted Dying in New Zealand
Pharmacists presented a range of issues that have been thematically derived into five main concerns (see Table 3) when legalising medically assisted dying in New Zealand.
3.3. Willingness to Provide EOLC-Based Services
Under half of pharmacist participants (n = 118, 40.8%) would support providing medically assisted dying consistent with the EOLC Act. Just under one-quarter of pharmacists were undecided (n = 71, 24.6%), and just over one-quarter of pharmacists (n = 77, 26.6%) would not provide the service.
Pharmacists that were undecided in their willingness to support EOLC services consistent with that Act tended to have a background in hospital (n = 18, 25.4%) or community pharmacy (n = 43, 60.6%) practice. They had an average of 11 to 30 years of experience, with a preference noted to be higher in those with 30 and above years of experience within the pharmacy profession. The mean age of this practitioner was either 31–35 years or 46–50 years of age.
Table 4 outlines a thematic analysis of free text responses when asked what services pharmacists would be willing to provide to support the provision of legally assisted dying. Pharmacists reported that they would comply with their scope of practice and provide whatever service they could within that scope. They would engage in obtaining informed consent and referring patients to an appropriate practitioner. Regarding professionalism, pharmacists discussed being comfortable providing counselling and support for patients and their whānau and providing information when requested. Respondents saw themselves as part of a wider multi-disciplinary team and would support increasing awareness of an EOLC service.
Regarding access and services, pharmacists highlighted they would accept providing compounding, dispensing, and medication review services. They were happy to provide a delivery service and procure medicines for this service. Pharmacists also expressed interest in running education sessions and upskilling for this service provision. Table 4 summarises sample quotes from participants regarding possible service provision.
The analysis showed some pharmacists disagreed with taking part in any aspect of this service due to personal or religious beliefs, as demonstrated by the quote below:
“I do not wish to assist on ethical grounds and should have the choice not to do so without repercussion” (Pharmacist 126).
Some participants also reported this service falling outside their scope of practice.
In such cases, some pharmacists noted they would provide a referral service to hospice or palliative care. Some pharmacists also noted with uncertainty that their involvement would depend on other pharmacist peers and professional risk, suggesting that further guidance from a professional pharmacy organisation could be useful in exemplifying the conduct that regulators wish to see. This is consistent with quantitative data whereby those in the “maybe” category (n = 21, 74.6%) accounted for a proportion of pharmacists that could support medically assisted dying consistent with the EOLC act, but require further information to make an informed choice about future service engagement.
4. Discussion
This study investigated New Zealand pharmacists’ awareness of, support for, and influences on their attitudes toward the End of Life Choice Act and their willingness to provide services consistent with the EOLC Act.
A study from 2019 (n = 475) indicated that 67% of nurses (n = 318) supported medically assisted dying service provision, whereas only 37% of doctors (n = 110) supported medically assisted dying services [23,24]. The public referendum indicated that 65.1% (n = 1,893,290) supported the End of Life Choice Act 2019, and 33.7% (n = 979,079) indicated that they did not [25]. Just over half (58%) of the pharmacists that responded to the survey supported legalising medically assisted dying; almost a third of participants did not support it (29%), and 13% of respondents were unsure. A small proportion of pharmacists (16%) reported having read the Act in full, and most participants had not attended relevant training courses. This is understandable, as the survey was conducted prior to the Act being implemented. However, it raises the question of the need to provide pharmacists with timely, relevant, and targeted training opportunities. The media played an important role in promulgating information, as 45% of participants first learned of the EOLC Act through the media.
It is clear that role clarification, education, and training are needed for the pharmacy profession. At the time of the Act passing legislation, there was ambiguity in translating the Act into practice and little guidance on the role of the pharmacist in this process [26,27]. Furthermore, less than one-quarter (22%) of pharmacists reported being knowledgeable or very knowledgeable about the Act. In the absence of media, just over one-third of pharmacists (34.6%) reported learning about the Act through the referendum and 7.6% through a professional pharmacy organisation. The Ministry of Health has acknowledged that pharmacists have important roles in the community setting, and that it is important for pharmacy staff to have an understanding of the law and know where to find information should they be asked about the service [28].
A few participants referred to the emotional distress that could come from handing out assisted dying medication to patients. This is a practice that happens abroad and demonstrates role ambiguity that may have occurred earlier in the implementation phase where the pharmacist role was not clear with regard to what they would or could do within this service provision [1,2].
Moral sensitivity is known to be a key factor in attitudes towards assisted dying. In context, this is the ability of pharmacists to look past their personal belief systems, identify the moral problems associated with assisted dying, and understand the consequences of their decisions as health professionals [29]. There are some pharmacists who would not wish to access assisted dying themselves but feel strongly about people having a choice to end unbearable suffering. There are other pharmacists who believe that assisted dying is wrong, would not access the service themselves, and are unwilling or unable to explore perspectives beyond their own personal belief system. Moral sensitivity appears to be influenced by an individual’s capacity for empathy [30]. Strong themes of empathy toward unbearable suffering emerged in the qualitative data.
The decision to not support the EOLC Act and not be willing to provide related services was significantly correlated with religious beliefs. Participants who stated their personal and ethical beliefs were very influential were more likely not to support the legalisation of services related to medically assisted dying.
There was a large proportion of participants who responded with “maybe” or “unsure”. The assumption is made that these participants did not identify with a religion but indicated that they supported the legalisation of medically assisted dying services. Those participants that were unaffected by the attitude of a professional pharmacy organisation differed from those that lacked information in addition to being unsure; presumably because they were not affiliated with a professional pharmacy organisation. Those who indicated that they were somewhat influenced by the media were more likely to support medically assisted dying services than those who answered no to this question. Overall, participants were not significantly influenced by their friends, the stance of professional pharmacy organisations, the media, or colleagues.
Personal belief systems and religion serve as one of the most significant influences on the acceptability of medically assisted dying. This investigation has highlighted the dichotomy that can occur while working as a health professional and holding their own personal beliefs, which drive behaviour. As health professionals, pharmacists are held accountable for fulfilling the minimum competency standards outlined by the New Zealand Pharmacy Council [10]. Humans are highly socialised. Our philosophy of the world around us is largely shaped by our early upbringing, life experiences, cultural or religious norms, and values held by our loved ones or those we spend the most time around [31]. CO clauses are what acknowledge this dichotomy, allowing for compromise when professional obligations tangle with personal belief systems. Religion is the only statistically significant influence on pharmacists’ attitudes toward the assisted dying service in New Zealand. These findings are similar to those of our Australian pharmacist colleagues [1]. Personal belief systems are deeply ingrained in our schema, which highlights the requirement to further explore the perspectives of those undecided pharmacists as a means to improve patient access and experience in this area of healthcare. Being able to recognise one’s conscientious bias with regard to this topic and continuing to provide health services appropriate to patients needs requires further consideration.
4.1. Implications for Policy Makers, Pharmacy Leaders, and Universities
This research highlights the need for tailored continuing education on this topic, aligning with international findings from Australia and Canada [1,4,32]. It raises the important role of professional regulatory bodies in maintaining well-informed health professionals within this evolving healthcare climate. There is a need for guidance documents to be developed and distributed to all pharmacists, and to include how to navigate CO within the community pharmacy context. Continuing education to facilitate the communication skills required for responding to requests, ensuring safe access to the service, and reducing cultural, societal, and existential issues could be considered. Further education around equity and the response of indigenous populations and their views could also be considered [33].
There are a number of pharmacists whose responses suggest the implementation of assisted dying could perpetuate under-investment in downstream palliative care options. This is consistent with concerns about inequity in the quality of palliative care in New Zealand [34]. Additionally, some stated that inequitable access to palliative care could lead to inappropriate uptake of assisted dying.
4.2. Implication of the Findings for Practitioners
A portion of the profession reported they would be better able to participate in assisted dying if there were more precise guidance or codes of conduct from professional pharmacy organisations to allow them to be prepared to handle assisted dying scenarios. Pharmacists commented that there was positive interest in providing dispensing of medications or medication procurement in addition to the delivery of medications, which were traditional aspects of service delivery that pharmacists are familiar with. Pharmacists also noted an interest in participating in continuing education in this area and developing specialty skills or a scope. Nevertheless, clearer direction about definitions of activity within this scope and the provision of such services in a legislatively compliant framework are needed to decrease ambivalence and uncertainty about participation. Furthermore, pharmacists highlighted the need for a protocol for practice to help pharmacists comply with laws surrounding medically assisted dying [1,35].
Whilst the management of CO and the health practitioner’s religion have been issues that have been present in practice, it is important for pharmacies to have systems in place to follow legislative requirements, and to ensure patients can navigate this pathway safely and that professionalism and respect for patient autonomy are upheld [1,35,36,37,38,39,40].
4.3. Implications of the Findings for Future Research
The regional locations of participants were not gathered as part of the demographic data. Further investigation should determine whether conscientious-objection-related service and access problems are primarily an urban or regional problem, allowing service providers and health officials to ensure there is adequate geographical overlap and access to practitioners to ensure parity and equity-related access to suitable health services [4]. Further exploration of the one-quarter of undecided pharmacists (n = 71, 24.6%) to better understand drivers behind their decision-making regarding service provision could better inform regulatory policy and management around codes of conduct and clarify ambiguity in professional delivery of services. Further investigation into health practitioner personality traits could also be explored to understand the decision-making process with health service provision offerings in comparison to the religion of health practitioners.
5. Limitations
Not all pharmacists practicing within New Zealand responded to the survey, making it difficult to generalise with confidence these findings to the wider pharmacist population. The low response rate makes it challenging to arrive at considered decisions regarding pharmacy practice. Non-responder bias was not assessed, and neither was a power calculation.
It is challenging to ascertain the factors influencing pharmacists’ support or otherwise of the Act. Their perspective has the potential to be influenced by having access to authoritative information about the reality of service provision and how its implementation is proceeding in New Zealand, and further exploration of this could help better inform policy makers on aiding health professionals in decision making in the future. At the time of survey distribution, the Act had not come into effect, so pharmacy organisations and management may not have had time to address concerns raised by pharmacists regarding expectations around service provision.
Responses may have also been influenced by participants’ assumed likelihood of working in a pharmacy providing the service, or their likelihood of having to converse about assisted dying, rather than the perspective of widening access to end-of-life care to New Zealand society. In this instance, those pharmacists would be required to disclose their CO, and such disclosure can realistically create discontent or discomfort within the workplace. Among these participants, it is likely this has shifted some focus of their responses from access to a health service, and instead, toward their discomfort in working within a health system that has legalised assisted dying.
Overall, the nature of this topic has led to responses being based on personal experience and opinion, rather than factual occurrences in the workplace or the realistic implementation of the service.
6. Conclusions
The willingness of pharmacists’ to accept and participate in the process of medically assisted dying is multifactorial. Its nature and complexity have lent themselves to a myriad of attitudes that pharmacists hold towards its implementation. The influences on the decision by pharmacists to support and willingness to participate in the provision of services consistent with the End of Life Choice Act are complex. Diverse factors may influence attitudes, of which religion is the most significant factor in not supporting the Act or willingness to participate in assisted dying. Clarity of process and practice and standardised guidance to ensure that assisted dying queries are appropriately managed in practice would help to address any potential access issues in pharmacy.
Further research exploring how assisted dying has unfolded in New Zealand since the implementation of the End of Life Choice Act is required to help better inform health professionals to make decisions around their involvement in this process.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isaac S. Mc Lachlan A. Chaar B. Australian pharmacists’ perspectives on physician-assisted suicide (PAS): Thematic analysis of semistructured interviews BMJ Open 20199 e 02886810.1136/bmjopen-2018-02886831666261 PMC 6830588 · doi ↗ · pubmed ↗
- 2Berard G. Walker J. C Ph A surveys pharmacists on physician-assisted dying Can. Pharm. J. CPJ 2016149545510.1177/1715163515621879 PMC 471389826798378 · doi ↗ · pubmed ↗
- 3Naafs N.J. Pharmaceutical care until the end: The role of pharmacists in euthanasia in The Netherlands Pharm. World Sci. PWS 20012312913110.1023/A:101182050971711599197 · doi ↗ · pubmed ↗
- 4End of Life Choice Act 2019 No 67 (as at 28 October 2021), Public Act Contents—New Zealand Legislation Available online: https://www.legislation.govt.nz/act/public/2019/0067/latest/DLM 7285905.html(accessed on 20 March 2023)
- 5White B.P. Jeanneret R. Close E. Willmott L. The impact on patients of objections by institutions to assisted dying: A qualitative study of family caregivers’ perceptions BMC Med. Ethics 2023242210.1186/s 12910-023-00902-336915087 PMC 10009962 · doi ↗ · pubmed ↗
- 6Mac Leod R.D. Wilson D.M. Malpas P. Assisted or Hastened Death: The Healthcare Practitioner’s Dilemma Glob. J. Health Sci.20124879810.5539/gjhs.v 4n 6p 8723121745 PMC 4776959 · doi ↗ · pubmed ↗
- 7End of Life Choice Act 2019 No 67 (as at 28 October 2021), Public Act 13 First Opinion to be Given by Attending Medical Practitioner—New Zealand Legislation. (n.d.)Available online: https://www.legislation.govt.nz/act/public/2019/0067/latest/DLM 7285958.html(accessed on 20 March 2023)
- 8Isaac S. Pro B.C. Con J.S. Should Pharmacists Be Allowed to Conscientiously Object to Medicines Supply on the Basis of Their Personal Beliefs?Can. J. Hosp. Pharm.20187114910.4212/cjhp.v 71i 2.186629736049 PMC 5931075 · doi ↗ · pubmed ↗