Does it take two to tango?
Daniel Mol, Erik A. Stel, Irene E. Hof

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
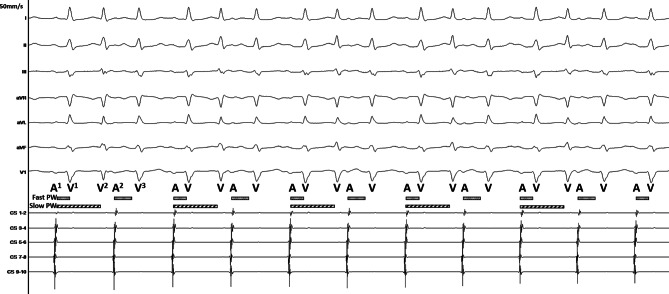 Figure 1
Figure 1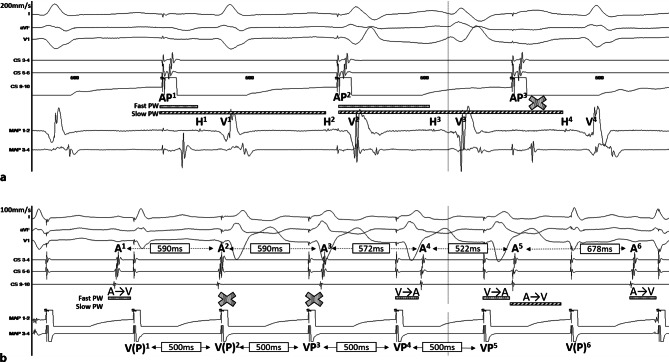 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrhythmias and Treatments · Atrial Fibrillation Management and Outcomes · Cardiac electrophysiology and arrhythmias
Answer
The intracardiac tracing presented in Fig. 1 shows that one atrial beat (A^1^) is followed by two QRS complexes (V^1^ and V^2^) and that the second atrial beat (A^2^) produces only one QRS complex (V^3^). This pattern is repetitive along the tracing. We were able to reproduce this rhythm by atrial pacing (AP) (Fig. 2a) and observed that each V was preceded by a His bundle potential (H), suggesting that the rhythm is supraventricular. Ventricular pacing (VP) at a cycle length of 500 ms repeatedly resulted in a VA Wenckebach: the atrial activation sequence changes (A^4^ and A^5^), the A–A interval decreases (A^3^–A^4^ and A^4^–A^5^), and the VA interval lengthens (VP^4^–A^4^, VP^5^–A^5^) (Fig. 2b). Notably, a narrow QRS complex [V(P)^6^] followed after A^5^. As the activation wavefront was conducted retrogradely from VP^5^ through the fast pathway to the atrium (A^5^), the fast pathway must be refractory. Therefore, the narrow QRS complex has to result from a second AV pathway, which is, in this case, a slow pathway (Fig. 2b; [1]). Thus, Fig. 1 shows a non-reentrant AV-nodal tachycardia (dual AV-nodal response) resulting from anterograde fast and slow pathway conduction [2]. The extremely prolonged slow pathway conduction (A^1^–V^2^) enables the His bundle to conduct the activation wavefront into a second QRS complex. Then, after A^2^, the slow pathway is refractory, and only the fast pathway conducts the activation wavefront (V^3^). In Fig. 2a, the same phenomenon occurred: AP^1^ initiates H^1^ and H^2^. We cannot conclude if H^4^ is a result of slow pathway conduction after AP^2^ or fast pathway conduction after AP^3^. The AP^3^–H^4^ time is shorter than the AP^2^–H^3^ time. Therefore, we assume that this beat also conducts through the slow pathway. However, the AP^2^–H^3^ time might be prolonged because of conduction in the relative refractory period. We successfully eliminated the non-reentrant AV-nodal tachycardia via slow pathway modification.Fig. 1. Intracardiac tracing. For a detailed explanation, please see the text. Fast PW fast pathway, Slow PW slow pathway, A atrial activation, V ventricular activationFig. 2Intracardiac tracing during atrial (a) and ventricular pacing (b). For a detailed explanation, please see the text. AP atrial pacing, H His bundle potential, V ventricular activation, A atrial activation, VP ventricular pacing, V(P) (pseudo) fusion, Fast PW fast pathway, Slow PW slow pathway, A→V conduction from the atrium to the ventricle, V→A conduction from the ventricle to the atrium. Coronary sinus diagnostic catheter (CS), ablation catheter (MAP) located on the His bundle (a) and in the right ventricle (b)
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Veenhuyzen GD Quinn FR Wilton SB Clegg R Mitchell LB Diagnostic pacing maneuvers for supraventricular tachycardia: part 1Pacing Clin Electrophysiol Pace 201134676778210.1111/j.1540-8159.2011.03076.x 21438892 · doi ↗ · pubmed ↗
- 2Wu D Denes P Dhingra R Pietras RJ Rosen KM New manifestations of dual A-V nodal pathways Eur J Cardiol 1975244594661126354 · pubmed ↗