Managing Ventricular Wall Rupture as a Complication of Late Presentation MI in a Complex Patient with Ankylosing Spondylitis
Waleed Shaker, Ahsan A. Khan, Michael K. O. Boateng, Mahmoud Abdelziz, Lampson Fan

TL;DR
This case report describes the successful surgical management of a rare heart complication in a patient with ankylosing spondylitis during the post-COVID-19 era.
Contribution
The paper presents a rare case of ventricular wall rupture managed successfully in a complex patient with ankylosing spondylitis.
Findings
Ventricular wall rupture was diagnosed early and treated surgically with a good outcome.
The patient had ankylosing spondylitis, complicating the surgical approach and recovery.
The case highlights the importance of considering this complication in late-presenting heart attacks.
Abstract
Ventricular free wall rupture is an infrequent but serious complication of myocardial infarction with high mortality despite surgical intervention. In recent years with the COVID-19 pandemic, observational studies have reported a rise in this complication most likely due to patient hesitation in seeking urgent medical assistance for fear of contracting COVID-19 in a hospital setting. This case report highlights the early recognition and diagnosis of ventricular wall rupture by the heart team with a good surgical outcome in a complex patient with ankylosing spondylitis. Ventricular rupture should be considered in deteriorating patients presenting with suspicion of late presentation myocardial infarction. Clinicians in the post-COVID-19 era should expect to see these complications more frequently.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
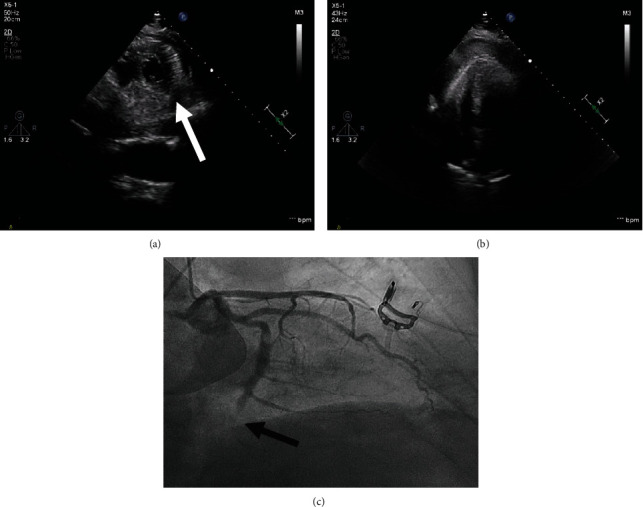 Figure 1
Figure 1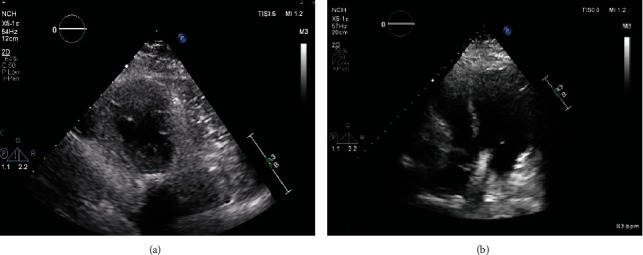 Figure 2
Figure 2- —Joint Information Systems Committee
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Structural Anomalies and Repair · COVID-19 and healthcare impacts · Pericarditis and Cardiac Tamponade
1. Introduction
Ventricular free wall rupture is an infrequent but serious complication that occurs within the first 96 hours post-MI with mortality rates as high as 88.2% [1]. Cardiac surgery is the mainstay of treatment [2], but despite surgical intervention, patients who undergo successful repair have a 58.9% survival rate after 3 years [3]. In recent years, the COVID-19 pandemic has had a dramatic effect on life in the world and has significantly impacted and burdened the medical community. This is especially concerning for patients who may be suffering from myocardial infarctions, as a delay in treatment can lead to devastating consequences [4, 5]. Since the onset of the COVID-19 pandemic in 2020, there has been a much higher incidence of mechanical complications, such as valvular or ventricular wall ruptures, from myocardial infarctions due to delay in treatment [6, 7] most likely due to patient hesitation in seeking urgent medical assistance for fear of contracting COVID-19 in a hospital setting [8].
2. Case
A 54-year-old gentleman was admitted to our hospital following a collapse in public. He had no cardiac history but has a history of ankylosing spondylitis with severe kyphosis. He reported chest pain five days prior to presentation. On arrival at the hospital, he was haemodynamically unstable with a blood pressure of 63/48 mmHg. 12-lead electrocardiogram showed ST-segment elevation in inferior leads with established Q waves consistent with late presenting inferior ST-elevation MI (Supplementary Figure 1). A bedside echocardiogram showed a moderately impaired ventricle with an ejection fraction of 40% and suspected LV wall rupture at the apical inferior wall with a moderate-size pericardial effusion mainly around the LV apex with clots (Figures 1(a) and 1(b); Supplementary video 1-3). A provisional diagnosis of cardiac tamponade due to LV rupture was made. Following discussion with cardiac surgeons, a coronary angiogram was performed which showed an occluded dominant distal left circumflex artery (Figure 1(c)) and confirmed that this is likely an ischaemic ventricular rupture. An intra-aortic balloon pump was inserted in an attempt to stabilize the patient which improved his systolic blood pressure to 90/50 mmHg and brought him sufficient time to have emergency surgery.
The patient was transferred to the theatre for emergency surgery. He was unable to be intubated due to the severe kyphosis, so cardiopulmonary bypass was established peripherally under local anesthetic with femoral-femoral bypass whilst the patient was awake. Opening of the chest wall revealed a contained pericardial effusion around the LV apex with clots. The LV wall rupture was visualized along with evidence of acute MI laterally. The rupture was successfully repaired on beating heart bypass. Postsurgery TTE confirmed resolution of pericardial effusion and repair of the LV wall (Figure 2; Supplementary Video 4, 5; Supplementary Figure 2). The patient's postoperative course was uneventful, and he was subsequently discharged home. At 10 months, the patient remained well, and his TTE showed EF of 40% with no pericardial effusion.
3. Summary
In summary, ventricular rupture should be considered in deteriorating patients presenting with suspicion of late presentation myocardial infarction. Early recognition, diagnosis, and involvement of the surgical team can achieve a good outcome for ventricular rupture especially in complex patients. An early bedside echo was a crucial step in the management of our patient and allowed serial assessment of the LV pre- and postsurgery. Clinicians in the post-COVID-19 era should expect to see these complications more frequently.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Purcaro A. Costantini C. Ciampani N. Diagnostic criteria and management of subacute ventricular free wall rupture complicating acute myocardial infarction The American Journal of Cardiology 199780439740510.1016/S 0002-9149(97)00385-82-s 2.0-00308659069285648 · doi ↗ · pubmed ↗
- 2Panesar G. Bhende V. V. Sharma T. S. Perioperative management of a patient with left ventricular free wall rupture after myocardial infarction: a rare case scenario Cureus 2022149, article e 2936810.7759/cureus.29368 PMC 948886036159358 · doi ↗ · pubmed ↗
- 3Matteucci M. Kowalewski M. De Bonis M. Surgical treatment of post-infarction left ventricular free-wall rupture: a multicenter study The Annals of Thoracic Surgery 202111241186119210.1016/j.athoracsur.2020.11.01933307071 · doi ↗ · pubmed ↗
- 4De Rosa S. Spaccarotella C. Basso C. Reduction of hospitalizations for myocardial infarction in Italy in the COVID-19 era European Heart Journal 202041222083208810.1093/eurheartj/ehaa 40932412631 PMC 7239145 · doi ↗ · pubmed ↗
- 5Abramo D. M. Saltarocchi S. Vignaroli W. Increased incidence of postmyocardial infarction ventricular septal defects during Covid-19 pandemic: a case series Journal of Cardiac Surgery 20223761759176310.1111/jocs.1643035315186 PMC 9115124 · doi ↗ · pubmed ↗
- 6Otero D. Singam N. S. V. Barry N. Raheja P. Solankhi A. Solankhi N. Complication of late presenting STEMI due to avoidance of medical care during the COVID-19 pandemic JACC Case Report 20202101610161310.1016/j.jaccas.2020.05.04532835260 PMC 7269918 · doi ↗ · pubmed ↗
- 7Primessnig U. Pieske B. M. Sherif M. Increased mortality and worse cardiac outcome of acute myocardial infarction during the early COVID-19 pandemic ESC Heart Failure 20218133334310.1002/ehf 2.1307533283476 PMC 7835606 · doi ↗ · pubmed ↗
- 8Nasr G. H. Glovaci D. Mikhail A. Left ventricular free wall rupture as a result of delayed presentation of an inferior ST-elevation myocardial infarction due to fear of COVID-19: case report Journal of Cardiothoracic Surgery 2021161 p. 10610.1186/s 13019-021-01495-x PMC 806188333888133 · doi ↗ · pubmed ↗