A Case Report Emphasizing an Early Approach in a Patient With Diffuse Axonal Injury
Mansee S Dangare, Akshaya Saklecha, Pallavi Harjpal

TL;DR
This case report describes the treatment of a young man with diffuse axonal injury following a bike accident, highlighting physiotherapy's role in improving recovery.
Contribution
The report emphasizes an early integrative physiotherapy approach to improve functional outcomes in diffuse axonal injury patients.
Findings
The patient showed improvement in functional independence through consistent physiotherapy.
Combining techniques like joint approximation and PNF helped enhance recovery.
Outcome measures like FIM and GCS were used to track progress.
Abstract
Diffuse axonal injury (DAI) is a severe and frequently life-altering form of traumatic brain injury that is brought on by forces of rapid acceleration as well as deceleration impacting the brain. DAI primarily stems from mechanical forces that lead to the widespread disruption of axons throughout the brain. Unlike focal injuries that affect a specific brain region, DAI manifests as multifocal axonal damage, often impairing vital neural connections. This injury occurs due to shear and tensile forces during traumatic events, such as car accidents, falls, and sports-related incidents. This current case report includes a 19-year-old male who had a fall from his bike and was hospitalised with brain trauma. A Magnetic resonance imaging (MRI) scan was done, which revealed a case of DAI, and a computed tomography (CT) scan of the brain revealed the extra-calvarial soft tissue swelling in the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
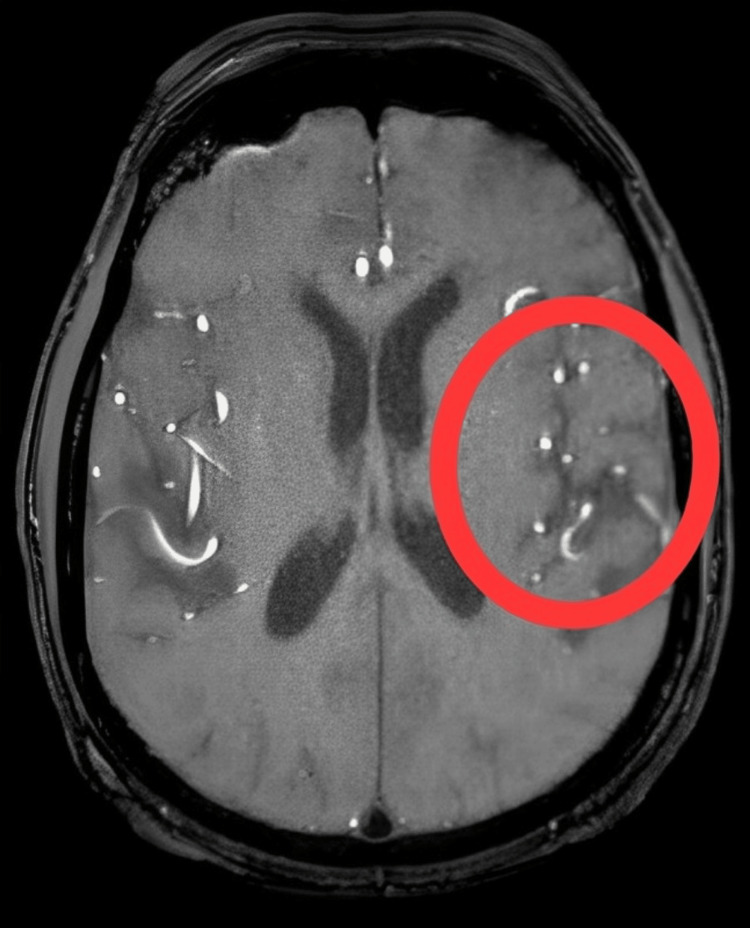 Figure 1
Figure 1 Figure 2
Figure 2| Muscle tone | Right side | Left side |
| Upper limb | 2+ | 1+ |
| Lower limb | 2+ | 1+ |
| Reflexes | Right side | Left side |
| Biceps | ++ | ++ |
| Triceps | ++ | + |
| Supinator | ++ | + |
| Knee | ++ | + |
| Ankle | ++ | + |
| Plantar | Flexors | Flexors |
| Incidents | Occurrence |
| Fall from bike | 04/10/2023 |
| Visited a private hospital in Chandrapur | 04/10/2023 |
| Discharge from a hospital in Chandrapur | 09/10/2023 |
| Date of admission in AVBRH | 09/10/2023 |
| The date of physiotherapy started | 15/10/2023 |
| Serial. No. | Medication | Dosage | Duration |
| 1. | Ascorbic Acid+ Cerebroprotein Hydrolysate +Cholecalciferol +Folic Acid +Methylcobalamin +Piracetam +Pyridoxine +Thiamine +Tocopherol | 20 mg | BD |
| 2. | Tab. Lasix | 15 mg | OD |
| 3. | Tab. Nicardia | 20 mg | TDS |
| 4. | Tab. Levepsy | 500 mg | BD |
| 5. | Tab. Doxycycline | 10 mg | BD |
| Goals | Therapeutic intervention | Treatment protocol |
| Patient education | A patient relative was informed about their disease as well as the importance and advantages of physical rehabilitation. Obtaining the family members' confidence and permission. | Education was given to caretakers regarding the significance of appropriate body alignment. |
| To normalise muscle tone | PNF rhythmic initiation D1 flexion-extension to left upper and lower extremity. | A single set of ten repetitions two times each day. |
| Joint approximation to upper extremity and lower extremity. | ||
| To improve left upper limb and lower limb range of motion exercises | Passive ROM exercises to left upper and lower extremity. | A single set of ten repetitions, two times each day. |
| To improve right upper limb and lower limb range of motion exercises | Active assisted ROM exercises to the right upper extremity and lower extremity. | A single set of ten repetitions, two times each day. |
| To ensure good ventilation | Deep breathing exercises and pursed lip breathing exercises. | A single set of ten repetitions, two times each day. |
| Improve airway permeability | Manual chest techniques (percussion and vibrations), suctioning and positioning. | Changing positions every two to three hours and manual methods for 10 repetitions. |
| Bed mobility | Supine - side lying - bedside sitting with maximal assistance. | 2 times a day for 1 week. |
| To avoid pressure sores resulting from extended immobilisation | Manual positioning, air bed provided. | Positioning for every 2-3 hours. |
| Getting out of bed with a wheelchair | To encourage the patient's mobility and raise their level of attentiveness. | Every day for 1 hour. |
| Serial. No. | Outcomes measured | Pre-intervention | Post-intervention |
| 1. | Glasgow Coma Scale | 11/15 | 13/15 |
| 2. | Tone grading scale | 1+ | 2+ |
| 3. | Functional Independence Measure | 1/7 | 6/7 |
| 4. | RLA scale | 2/10 | 6/10 |
| 5. | ICU mobility scale | 0/10 | 6/10 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTraumatic Brain Injury Research · Traumatic Brain Injury and Neurovascular Disturbances · Cerebral Palsy and Movement Disorders
Introduction
Diffuse axonal damage (DAI), also known as shear injury or traumatic axonal injury, is intracranial damage produced by the brain's neurons, decelerating or accelerating rapidly and repeatedly [1]. It appears to be connected to comatose following traumatic brain injury (TBI) and is believed to be present in almost all individuals who lose consciousness following a vehicle accident [2]. DAI was observed in 69% of overall mild TBI patients, as well as 89% of serious TBI individuals. DAI with a grade 3 traumatic lesion in the brainstem in areas typically of DAI (dorsolateral quadrant of the upper brainstem, superior cerebellar peduncles, with or without lesions in the lobar white matter) was observed in 30% of the people having serious TBI and 20% of individuals with mild TBI [3]. The brain experiences a variety of forces throughout a TBI, including compressive, tensile, and rotational stresses. The brain's inertia causes the cervical column to become dissociated from its relative motion, so when the head moves quickly throughout trauma without suffering a major physical blow, translational, rotational, and angular accelerations can cause damage to axons or blood vessels to expand, primarily in instances of acceleration due to rotation [4,5]. In addition to primary axotomy caused by mechanical forces, DAI is caused by a slow series of pathological modifications in the axon's molecules and cells that follow the first shear stress at the location of injury [6].
Cognitive deficits, diminished memory, disorientation, and agonizing headaches are diagnostic symptoms and signs of DAI. Despite their catastrophic consequences, multiple studies have connected these damages to major neurological conditions [7]. At present, the primary goal of rehabilitation and physical therapy for patients with brain injuries treated in intensive care units (ICUs) is mainly on the body's functions and organization. Examples of these include oxygen therapy, low-dose endurance and power learning, stimulation treatment, breathing treatment, and passive-assistive activity for contraction prevention. Several of the treatments deal with tasks such as performing self-care or activities of daily living (ADL) learning, along with moving into a wheelchair, sitting posture, or standing [8].
Rehabilitation professionals have used a wide range of strategies to aid in the patient’s rehabilitation who suffered traumatic brain injuries. They focus on specific therapeutic concepts that are endorsed by separate physiotherapy [9]. The incorporation of freshly developed technology, such as Nintendo's Wii and Wii Fit virtual reality (VR) gaming systems, which are sold economically, might also have an impact on intervention material. These engaging and easily available VR video game systems employ motion-sensing technology that recognizes direction and velocity, enabling the kid to manipulate gaming through their movements and postures. These games encourage players to extend or intensify their practice sessions by offering information and repeating realistic challenges on a regular basis [10]. The major goals of therapy are frequently muscular improvement, prevention of subsequent injury such as pneumonia or stiffness, and recovery of consciousness and sensorimotor viewpoint. The primary goal is to get the maximum degree of movement and self-care capability [11].
Case presentation
Patient information
A 19-year-old male patient had a fall from a motorbike while he was returning to his home. After the accident, the patient was brought to a local private clinic in Chandrapur, with a GCS score of E1V1M4. He was hospitalized for five days after experiencing a loss of awareness without any prior history of bleeding or vomiting. He underwent a magnetic resonance imaging (MRI) scan, which confirmed it to be a case of DAI, and a CT scan revealed that small haemorrhagic contusions were seen involving the right gangliocapsular region of grade 3. He was managed conservatively and referred to a tertiary healthcare center where the patient was referred to the physiotherapy intensive care unit. The patient was intubated, and he was on a mechanical ventilator with mode-continuous mandatory ventilation, positive end-expiratory pressure (5 cm H20), and a fraction of inspired oxygen (70%) and received further treatment.
Clinical findings
On neurological examination, the patient was conscious with a GCS score of E1VTM4 and disoriented. Before beginning the examination, verbal consent was obtained from the patient's relative. He was examined while lying supine. On inspection, it was observed that the patient was seen in a supine lying position with the head end elevated to 30 degrees. The patient's hands and legs were extended and slightly abducted, abrasions over the bilateral knee joint, and Ryle's tube and Foley's catheter in situ. On the day of examination, the GCS score was 5/15 E1VTM4, and the patient was vitally stable. On palpation, the local skin temperature was raised. The muscle tone is shown in Table 1 and reflexes in Table 2. The complete incident's timeframe is depicted in Table 3.
Diagnostic assessment
MRI reveals multiple foci of blooming on susceptibility-weighted imaging (SWI) noted diffusely scattered through brain parenchyma involving subcortical, cortical regions, deep white matter, bilateral gangliocapsular regions, brainstem, and cerebellum suggestive of DAI, as shown in Figure 1.
MRI of the brainThe circled part indicates multiple foci blooming on SWI noted diffusely scattered through brain parenchyma involving subcortical, cortical regions, deep white matter, bilateral gangliocapsular regions, brainstem, and cerebellum suggestive of diffuse axonal injury.MRI: Magnetic resonance imaging, SWI: Susceptibility-weighted imaging
Medical management
Medicines such as Tab. cognilong plus, Tab. lasix, Tab. flucanazole, Tab. nicardia, Tab. levepsy, Tab. doxycycline and dosage, along with their duration, are given in Table 4.
Therapeutic intervention
The goal-oriented physiotherapy protocol is given in Table 5. Physiotherapy sessions included proprioceptive neuromuscular facilitation (PNF) rhythmic initiation D1 flexion-extension to the left upper and lower extremity (Figure 2A) and the joint approximation to the upper limb and lower limb (Figure 2B).
Physiotherapist performing PNFPNF: Proprioceptive neuromuscular facilitation (A) PNF rhythmic initiation D1 flexion-extension to upper extremity, (B) joint approximation to upper extremity
Follow-up and outcome measures
The pre-intervention outcome taken on day one and follow-up taken on the sixth week of intervention are given in Table 6.
Discussion
In this case, the patient suffered from serious diffuse axonal damage, which was treated conservatively using appropriate drugs, physical therapy, and other supportive therapies. The treatment procedure's goals were defined by first thoroughly teaching the patient and his family about his illness and the necessity of physiotherapy for his recovery.
Sometimes, the physiotherapist may combine various additional active or passive tissue "stretching" methods (such as appropriate posture, passive movements, and weight bearing) with a range of splints, customised orthoses, and plaster casts. Treatment goals usually involve lengthening shortened soft tissues, as well as inhibiting/reducing increasing muscular tone. Thus, in order to achieve this goal, early rehabilitation included chest-clearing activities, mild range-of-motion exercises, and facilitative methods for returning muscle tone to normal. Further, stretching methods were supplied to increase joint flexibility and avoid muscular tightness, and strengthening activities were provided progressively to enhance the endurance and strength of the muscles. Histopathological abnormalities in the lobar white matter, corpus callosum, and dorsolateral parts of the brainstem have been associated with higher trauma damage [12].
Sensorimotor reactions, including neuroplasticity and functional improvements, found throughout therapy after diffuse axonal injuries, are important considerations for physicians to consider. These mechanisms are connected to the level of cardiovascular exercise [13,14]. Neuroplasticity can be useful when it comes to improved functioning or maladaptive when it comes to diminished or abnormal performance. Rehabilitation's job is to steer the nervous system towards responsive neuroplasticity by evaluating and organizing sensorimotor information appropriately [15]. Research results promote the importance of changed axonal calcium homeostasis within the process of axonal secondary destruction, and they indicate that calcium channel blockers, which may reduce secondary harm, in addition to additional mechanisms suggested in secondary damage, may be focused on as treatments [16,17]. Outside the cell, Ca2+ is the primary cause of reactive oxygen species (ROS)-mediated degeneration of axons. Extracellular Ca2+ elimination, instead of blocking mitochondrial Ca2+ discharge, is an effective method for reducing intracellular calcium and limiting spheroid development [18]. Oxidative stress, a condition that damages the natural antioxidant defence systems, plays a crucial role in the subsequent processes that contribute to neuronal degeneration. Increased defence mechanisms by external antioxidants may be neurologically protective, especially if provided during the neuroprotective period frame [19,20].
Conclusions
DAI is a severe and frequently fatal kind of brain injury caused by trauma that causes extensive destruction of axons throughout the brain. DAI can result from various types of accidents and head trauma, and its effects can vary. TBI induces persistent malfunction and apoptosis of neuronal cells both close and far from the area of damage. Physiotherapy is an integral component of the multidisciplinary approach to managing DAI. It plays a significant role in helping the patient regain his physical and cognitive abilities and enhancing the quality of life in DAI.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Prognosis of diffuse axonal injury with traumatic brain injury J Trauma Acute Care Surg Humble SS Wilson LD Wang L 1551598520182946208710.1097/TA.0000000000001852 PMC 6026031 · doi ↗ · pubmed ↗
- 2Current concepts: diffuse axonal injury-associated traumatic brain injury Arch Phys Med Rehabil Meythaler JM Peduzzi JD Eleftheriou E Novack TA 146114718220011158875410.1053/apmr.2001.25137 · doi ↗ · pubmed ↗
- 3Traumatic axonal injury: the prognostic value of lesion load in corpus callosum, brain stem, and thalamus in different magnetic resonance imaging sequences J Neurotrauma Moen KG Brezova V Skandsen T Håberg AK Folvik M Vik A 148614963120142477358710.1089/neu.2013.3258 · doi ↗ · pubmed ↗
- 4Why most traumatic brain injuries are not caused by linear acceleration but skull fractures are Front Bioeng Biotechnol Kleiven S 15120132502232110.3389/fbioe.2013.00015 PMC 4090913 · doi ↗ · pubmed ↗
- 5Incidence of axonal injury in human brain tissue Acta Neuropathol Niess C Grauel U Toennes SW Bratzke H 798410420021207066810.1007/s 00401-002-0525-9 · doi ↗ · pubmed ↗
- 6Biomarkers associated with diffuse traumatic axonal injury: exploring pathogenesis, early diagnosis, and prognosis J Trauma Li J Li XY Feng DF Pan DC 161016186920102115053810.1097/TA.0b 013e 3181 f 5a 9ed · doi ↗ · pubmed ↗
- 7Axonal pathology in traumatic brain injury Exp Neurol Johnson VE Stewart W Smith DH 354324620132228525210.1016/j.expneurol.2012.01.013PMC 3979341 · doi ↗ · pubmed ↗
- 8Effectiveness of physiotherapy and occupational therapy after traumatic brain injury in the intensive care unit Crit Care Res Pract Hellweg S 768456201220122255057010.1155/2012/768456 PMC 3328889 · doi ↗ · pubmed ↗