Percutaneous pulmonary valve implantation in a patient with congenitally corrected transposition of the great arteries: a case report
Michal Kapalka, Michal Galeczka, Michal Krawiec, Roland Fiszer

TL;DR
A 20-year-old man with a rare heart defect successfully received a percutaneous pulmonary valve, marking a first in this specific anatomy.
Contribution
This is the first reported case of percutaneous pulmonary valve implantation in a patient with congenitally corrected transposition of the great arteries.
Findings
Percutaneous pulmonary valve implantation was successfully performed despite anomalous coronary arteries.
The 8-year follow-up showed no complications after the procedure.
Balloon testing confirmed the absence of coronary artery compression before valve implantation.
Abstract
Percutaneous pulmonary valve implantation has become an attractive method of dysfunctional right ventricle outflow tract treatment. We describe a unique case of a 20-year-old Caucasian male patient with a complex cyanotic heart defect, namely pulmonary atresia, with congenitally corrected transposition of the great arteries and ventricular septal defect after Rastelli-like surgery at the age of 5 years with homograft use. At the age of 20 years, the patient needed percutaneous pulmonary valve implantation owing to homograft dysfunction. Despite unusual course of the coronary arteries, balloon testing in the landing zone of the right ventricle outflow tract excluded potential coronary artery compression. Then, after presentation, a Melody valve was implanted successfully in the pulmonary valve position. The 8-year follow-up was uneventful. This is likely the first description of a…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
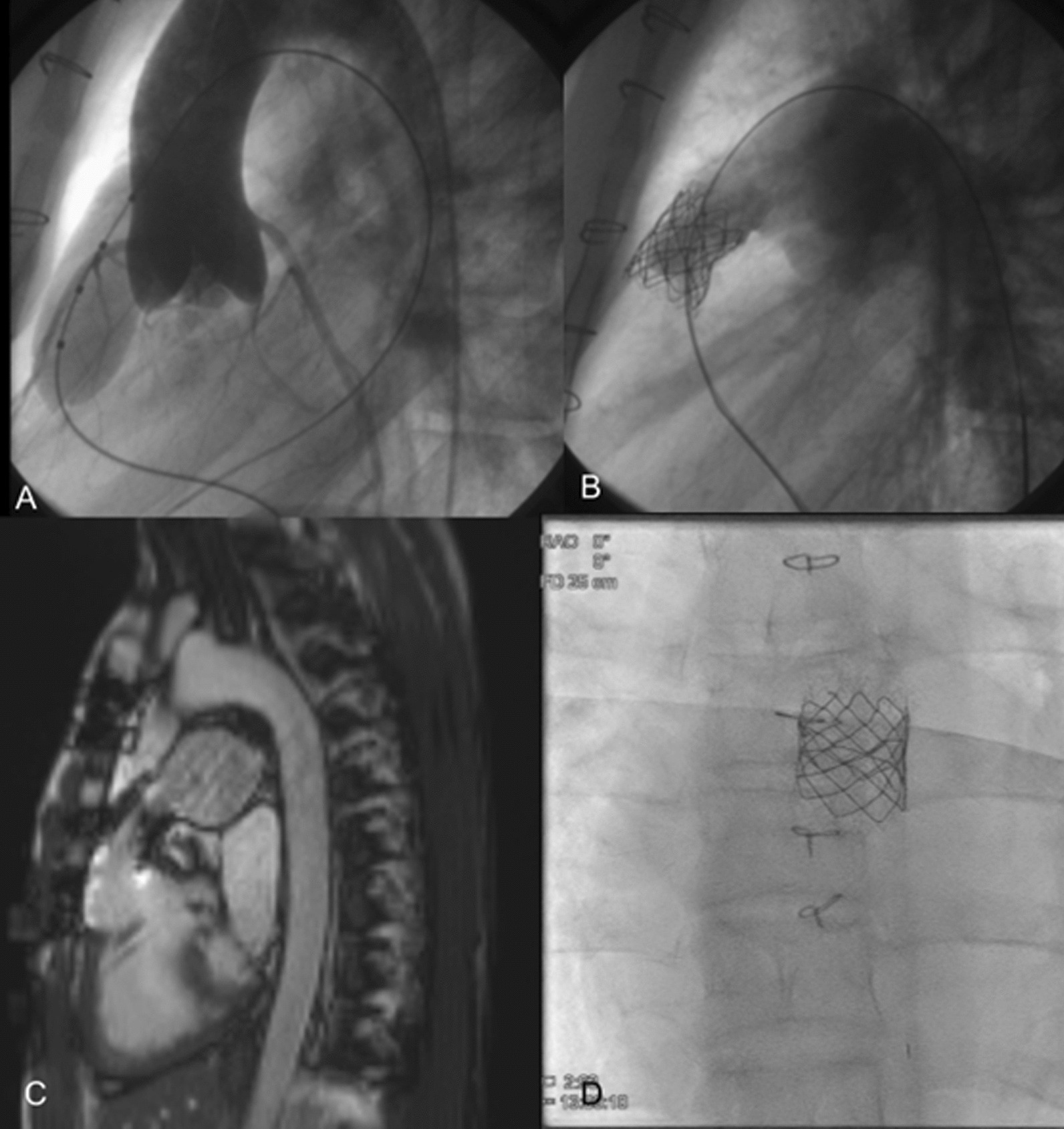 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Coronary Artery Anomalies · Pulmonary Hypertension Research and Treatments
Background
Percutaneous pulmonary valve implantation (PPVI) has become an attractive method of dysfunctional right ventricle outflow tract (RVOT) treatment [1]. We describe a unique case of a patient with a complex cyanotic heart defect, namely pulmonary atresia (PA), with congenitally corrected transposition of the great arteries (ccTGA) and ventricular septal defect (VSD) in whom PPVI was performed. Such a case has not been reported thus far.
Case presentation
A 20-year-old Caucasian male patient with complex cyanotic heart defects, namely, ccTGA, PA, and VSD, underwent left-sided Blalock–Taussig–Thomas shunt palliation at the second day of life, followed by a correction at the age of 5 years. The surgery included ventricular septal defect (VSD) patch closure and subpulmonary outflow tract reconstruction with a 17-mm homograft (Rastelli-type procedure). He was readmitted at 20 years old, with no symptoms in anamnesis and with good exercise tolerance. A loud systolic murmur with a thrill and soft diastolic murmur were found upon physical examination. Echocardiography revealed good function of the systemic ventricle—morphologic right ventricle (mRV) and homograft obstruction with a maximum and mean gradient of 78 mmHg and 45 mmHg, respectively, as well as its' moderate regurgitation. The peak-to-peak gradient of 82 mmHg through the narrowed-to-10-mm homograft was measured in the diagnostic catheterization and the patient qualified for PPVI.
Nonselective coronarography was performed to exclude the possibility of coronary artery (CA) compression assessed by aortography with a 20-mm Mullins-X balloon placed in the potential valve landing zone (Fig. 1A). The test revealed that the right coronary artery (RCA) originated from posterolateral sinus and the left anterior descending artery (LAD), with the circumflex artery (Cx), originated from medial sinus separately. Despite the short distance between the Cx origin and the homograft valve annulus, coronary artery compression was not an issue.Fig. 1A Aortography performed during 20-mm Mullins-X balloon inflation in the potential valve landing zone in lateral projection shows no coronary artery compression. B Angiography performed after successful implantation of AndraStent and 18-mm Melody valve shows good effect of the procedure with trace of a regurgitation. C Magnetic resonance imaging performed 8 years after the procedure shows good performance of the conduit with no regurgitation, no subpulmonary valve enlargement, and preserved subpulmonary ventricle function (EF of 48%). D Fluoroscopy 7 years after implantation of the Melody valve shows small, nonsignificant stent fractures with preserved stent and valve structure
The 35-mm AndraStent XXL (AndraMed GmbH, Reutlingen, Germany) was implanted into the homograft on a 20-mm balloon-in-balloon (BIB). Then, an 18-mm Melody valve (Medtronic Inc., MN) on an 20-mm BIB was expanded (Fig. 1B). Because of the residual peak-to-peak gradient of 30 mmHg, the 22 mm Mullins-X balloon was used for postdilatation, and the final gradient dropped to 15 mmHg (see Additional file 1: Video S1, S2; Additional file 2: Video S3, S4; Additional file 3: Video S5). In the 8-year follow-up, the patient remained asymptomatic with a mean residual gradient through the Melody valve of 22 mmHg on checkup echocardiography. Ejection fraction of the systemic ventricle was assessed to be 39% by magnetic resonance imaging (Fig. 1C). Single and insignificant fractures of the Melody valve stent (Cheatham-Platinum stent) are observed on fluoroscopy (Fig. 1D). No late complications, such as infective endocarditis, have been observed.
Discussion and conclusion
Congenitally corrected TGA with VSD and PA can be surgically treated by closing the VSD and placing mLV-to-pulmonary artery conduit in some cases [2]. Every implanted homograft carries the risk of future dysfunction, mostly due to its calcification and stenosis. After the Rastelli procedure, 51% of patients had reoperations owing to stenosis and insufficiency of the extracardiac conduit [3]. In patients with RV to pulmonary artery conduit stenosis, transcatheter valve implantation in the pulmonary position can be performed effectively [4]. A case series of a PPVI in two patients with ccTGA after Senning surgery was reported [5].
During PPVI, special attention should be paid to the risk of compression of the coronary arteries (CA). Morray et al. reported coronary artery compression in 4.7% of patients observed on preimplant testing [6]. Examined patients had various heart defects, and the majority (71%) of coronary artery compressions were noted in patients with an abnormal course [6]. Haas et al. reported abnormal coronary arteries in 32.8% of patients with dysfunctional right ventricle outflow tract [7].
Exceptional attention should be paid in cases of PPVI in patients with ccTGA, as CA origins are malpositioned, which is directly associated with aortopulmonary rotation [8]. PV is often localized between the ascending aorta and right atrium; therefore, CA may course closely to the potential valve implantation landing zone.
Stent fractures are a common adverse effect after Melody PPVI and occur in 25% of patients [9]. Stent fractures that do not affect its structure are not significant complications; however, the unusual position of the RVOT in patients with ccTGA might result in more frequent occurrence of stent fractures. Despite those precautions, given the correct anatomical foundation, PPVI in patients with ccTGA can be safely performed.
PPVI can be safely performed in patients with ccTGA after Rastelli-like repair. However, it requires exceptional caution due to the anomalous CA course, which can be reason for CA compression.
Supplementary Information
Additional file 1: Video S1, S2. Ventriculography at the level of homograft.Additional file 2: Video S3, S4. Coronary artery testing.Additional file 3: Video S5. Final arteriography after Melody valve implantation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Giugno L Faccini A Carminati M Percutaneous pulmonary valve implantation Korean Circ J 202050430231610.4070/kcj.2019.029132157831 PMC 7067602 · doi ↗ · pubmed ↗
- 2Ungerleider R Meliones JN Mc Millan KN Cooper DS Jacobs JP Critical heart disease in infants and children 2018 Amsterdam Elsevier
- 3Hörer J Schreiber C Dworak E Cleuziou J Zsolt P Long-term results after the Rastelli repair for transposition of the great arteries Ann Thorac Surg 20078362169217510.1016/j.athoracsur.2007.01.06117532417 · doi ↗ · pubmed ↗
- 4Fiszer R Dryzek P Szkutnik M Goreczny S Krawczuk A Immediate and long-term outcomes of percutaneous transcatheter pulmonary valve implantation Cardiol J 201724660461110.5603/CJ.a 2017.002328248409 · doi ↗ · pubmed ↗
- 5Rios R Foerster SR Gudausky TM Melody pulmonary valve implantation in two teenage patients with congenitally corrected transposition of the great arteries status after Senning atrial switch operation Cardiol Young 201727360060410.1017/S 104795111600158 X 27748225 · doi ↗ · pubmed ↗
- 6Morray BH Mc Elhinney DB Cheatham JP Zahn EM Berman DP Risk of coronary artery compression among patients referred for transcatheter pulmonary valve implantation: a multicenter experience Circ Cardiovasc Interv 20136553554210.1161/CIRCINTERVENTIONS.113.00020224065444 · doi ↗ · pubmed ↗
- 7Haas NA Vcasna R Laser KT Blanz U Herrmann FR The standing of percutaneous pulmonary valve implantation compared to surgery in a non-preselected cohort with dysfunctional right ventricular outflow tract—reasons for failure and contraindications J Cardiol 201974321722210.1016/j.jjcc.2019.03.02131230902 · doi ↗ · pubmed ↗
- 8Huang SC Chiu I-S Lee M-L Wu C-S Chang C-I Coronary artery anatomy in anatomically corrected malposition of the great arteries and their surgical implications Eur J Cardiothorac Surg 201139570571010.1016/j.ejcts.2010.09.00620943409 · doi ↗ · pubmed ↗