A Triad of Shoulder Injuries Following Cardioversion: A Case Report
Eng Kee Tan, Khairil Anwar Ahmad Hanif, Siti Munira Seri Masran, Fahrudin Che-Hamzah

TL;DR
A patient developed a shoulder injury after a cardioversion procedure, which has not been reported before.
Contribution
Reports a previously unobserved supraspinatus tear complication following cardioversion in a middle-aged Chinese patient.
Findings
A supraspinatus tear occurred in a patient after cardioversion for ventricular tachycardia.
The patient had no prior trauma history, suggesting the injury was caused by the procedure.
Abstract
Transthoracic defibrillation and cardioversion are commonly used techniques to resuscitate a patient during acute cardiac arrhythmic events. There are numerous complications associated with these procedures. We report a previously unreported complication where a patient suffered from a supraspinatus tear after cardioversion for ventricular tachycardia. There are numerous complications associated with these procedures. We report a previously unreported complication where a middle-aged Chinese patient with no previous trauma history suffered from a supraspinatus tear after cardioversion for ventricular tachycardia.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
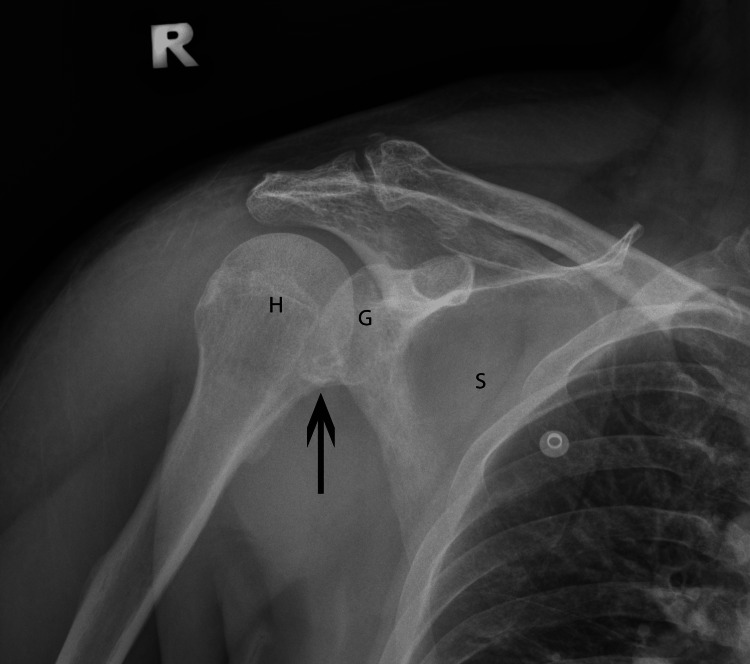 Figure 1
Figure 1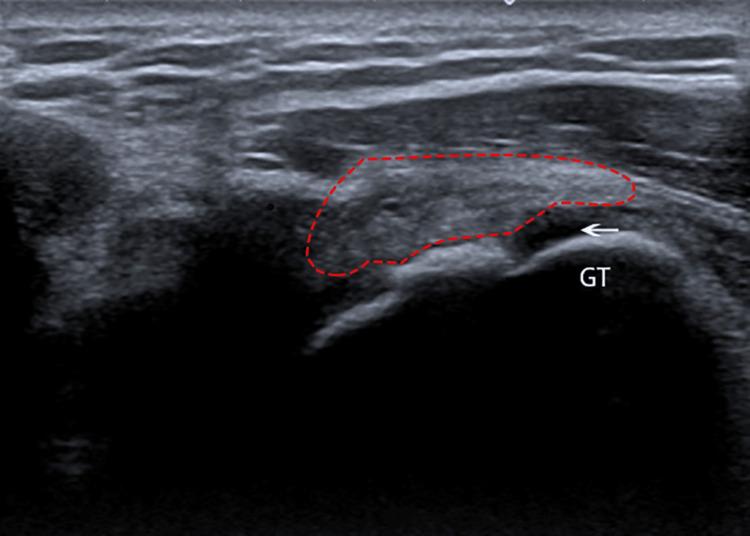 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Cardiac Arrhythmias and Treatments · Trauma Management and Diagnosis
Introduction
Transthoracic defibrillation and cardioversion are commonly performed during acute cardiac arrhythmias. Energy and current requirements depend on the arrhythmia type. For ventricular tachycardia (VT), the recommended level ranges between 70 and 200 Joules [1].
Cardioversion is associated with various complications. These include cardiac arrhythmias, pulmonary edema, and burns. During cardioversion, the electrical stimulation may cause skeletal muscle contraction. If these contractions are too vigorous, they can cause musculoskeletal injuries.
This case report highlights a triad of shoulder injuries consisting of anterior shoulder dislocation (humerus head displaced anteriorly relative to glenoid fossa of scapula), Bankart lesion (injury to the anteroinferior aspect of glenoid labrum), and partial supraspinatus tendon tear as another possible complication of cardioversion. Such a phenomenon is previously unreported.
Case presentation
The patient is a 45-year-old Chinese male who initially presented with an acute onset left-sided chest pain. He had no known underlying illness prior to presentation and had no preceding trauma or injury. He was diagnosed with a Killip IV acute inferior myocardial infarction and was thrombolyzed with streptokinase. He then developed VT and underwent cardioversion.
Upon resolution of the initial acute event, the patient complained of right shoulder pain, which was absent prior to admission. It was associated with weakness of the affected shoulder and swelling over the superior-lateral aspect, just distal to the acromion process. Abduction of the shoulder was limited with tenderness over the supraspinatus insertion area and a positive Dugas test. Plain radiographs revealed a Bankart lesion over the right glenoid (Figure 1).
Plain radiograph of the right-shoulder anterior-posterior view demonstrating a Bankart lesion over the glenoid fossa of the right scapula.H: Humerus head; G: Glenoid fossa; S: Scapula; Black arrow: Bankart lesion
An ultrasound of the right shoulder revealed a partial tear of the supraspinatus tendon with a long head of biceps tendonitis (Figure 2). He was placed on an armsling for his right shoulder and recovered well during follow-up after physiotherapy without the need for surgical intervention.
Ultrasound of the shoulder revealing a partial tear of the supraspinatus tendon from the greater tubercle of the humeral head.GT: Greater tubercle of humerus; Red outline: Supraspinatus tendon; White arrow: Partial tear of supraspinatus tendon from its attachment
Discussion
The shoulder joint is a ball and socket joint articulating the scapula and proximal humerus. It relies on multiple stabilizers, one of which is the rotator cuff that comprises four muscles - supraspinatus, infraspinatus, teres minor, and subscapularis [2].
Rotator cuff injuries tend to be disabling for the patient, as they lead to shoulder dysfunction due to secondary weakness caused by pain. Supraspinatus tears are the most common form of rotator cuff injuries and commonly result from a traumatic incident or a sports-related injury, and they are a well-known complication of shoulder dislocations [3].
Anterior shoulder dislocations are also commonly associated with Bankart lesions. Widjaja et al. reported an incidence of up to 85% in their study. They concluded that Bankart lesions are more likely to occur in anterior shoulder dislocations [4].
Transcutaneous cardioversion, though life-saving, can be associated with numerous complications. The more commonly encountered adverse events include transient ventricular dysfunction, arrhythmia, pulmonary edema, thromboembolism, and skin complications, such as erythema, burns, and pain [5].
Uncommonly, shoulder injuries can result as a complication of cardiopulmonary resuscitation, cardioversion, and seizure-like disorders. Gosens et al. reported two incidents of posterior shoulder dislocations following epileptic seizures. They stated that these injuries can be caused by uncontrolled muscular contractions, such as seizures or electric shock therapy [6]. In cardioversion, the electrical current involved in the usage of the device can potentially cause increased levels of muscular contractions, leading to potential musculoskeletal injuries.
Ould-Ahmed et al. reported one such incident of shoulder dislocation after cardioversion. The patient in this report had received cardioversion under propofol-induced general anesthesia for atrial fibrillation. It is likely that the vigorous muscle contractions from cardioversion caused the shoulder dislocation when it occurred in a generalized hypotonic state caused by anesthesia [7].
This complication is not limited to external cardioverters and can occur in subcutaneous implantable cardioverter-defibrillator devices (S-ICD). Two incidents of shoulder dislocation were reported after S-ICD testing. The electrical current generated by the S-ICD causes increased pectoralis major contraction, leading to adduction and internal rotation of the humerus, resulting in an increased risk of anterior shoulder dislocation [8].
Kam et al. also reported on a patient who sustained scapula and proximal humerus fractures after cardiopulmonary resuscitation and cardioversion. There was no direct trauma to the affected region during CPR, and it was postulated that the fractures occurred due to the cardioversion causing sustained muscle contraction of the shoulder girdle muscles [9].
Our case demonstrated an occurrence of an anterior shoulder dislocation, which was associated with a Bankart lesion and partial supraspinatus tendon tear. The dislocation was postulated to occur during the cardioversion. Although the dislocation had reduced spontaneously, the presence of a Bankart lesion and partial supraspinatus tear supports the diagnosis of an anterior shoulder dislocation. The triad of shoulder injuries sustained by the patient following cardioversion had never been reported before.
Conclusions
In conclusion, cardioversion from an acute cardiac event can be associated with numerous complications. In this case, we reported a triad of injuries to the shoulder following transthoracic defibrillation. The triad consists of an anterior shoulder dislocation, a Bankart lesion, and a partial supraspinatus tendon tear. These injuries had never been reported before following cardioversion.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ventricular tachycardia rate and morphology determine energy and current requirements for transthoracic cardioversion Circulation Kerber RE Kienzle MG Olshansky B 158163851992172844510.1161/01.cir.85.1.158 · doi ↗ · pubmed ↗
- 2Risk factors for supraspinatus tears: a meta-analysis of observational studies Orthop J Sports Med Zhao J Luo M Liang G 9202110.1177/23259671211042826 PMC 851638934660827 · doi ↗ · pubmed ↗
- 3Primary anterior shoulder dislocation and rotator cuff tears J Shoulder Elbow Surg Berbig R Weishaupt D Prim J Shahin O 220225819991038907610.1016/s 1058-2746(99)90132-5 · doi ↗ · pubmed ↗
- 4Correlation between Bankart and Hill-Sachs lesions in anterior shoulder dislocation ANZ J Surg Widjaja AB Tran A Bailey M Proper S 4364387620061676876310.1111/j.1445-2197.2006.03760.x · doi ↗ · pubmed ↗
- 5Randomized trial comparing the effectiveness of internal (through implantable cardioverter defibrillator) versus external cardioversion of atrial fibrillation J Interv Card Electrophysiol Elayi CS Parrott K Etaee F 2612675820203192766510.1007/s 10840-019-00689-7 · doi ↗ · pubmed ↗
- 6Posterior dislocation fractures of the shoulder in seizure disorders—two case reports and a review of literature Seizure Gosens T Poels PJ Rondhuis JJ 446448920001098600510.1053/seiz.2000.0418 · doi ↗ · pubmed ↗
- 7[Shoulder dislocation after cardioversion]Ann Fr Anesth Reanim Ould-Ahmed M Martinez JY Lions C Wey PF Dulac C Bernard F 2172520061641424010.1016/j.annfar.2005.10.014 · doi ↗ · pubmed ↗
- 8Shoulder joint dislocation as an unusual complication of defibrillation threshold testing following subcutaneous implantable cardioverter-defibrillator implantation Indian Pacing Electrophysiol J Noheria A Cha YM Asirvatham SJ Friedman PA 2973001420142560989710.1016/s 0972-6292(16)30818-x PMC 4286953 · doi ↗ · pubmed ↗