Severe acute respiratory coronavirus virus 2 (SARS-CoV-2) RNA and viable virus contamination of hospital emergency department surfaces and association with patient coronavirus disease 2019 (COVID-19) status and aerosol-generating procedures
Scott C. Roberts, Elliana S. Barbell, Douglas Barber, Suzanne E. Dahlberg, Robert Heimer, Karen Jubanyik, Vivek Parwani, Melinda M. Pettigrew, Jason M. Tanner, Andrew Ulrich, Martina Wade, Anne L. Wyllie, Devyn Yolda-Carr, Richard A. Martinello, Windy D. Tanner

TL;DR
This study found that hospital emergency department surfaces are often contaminated with SARS-CoV-2, especially in rooms where patients with COVID-19 did not undergo aerosol-generating procedures.
Contribution
The study identifies a link between patient COVID-19 status and surface contamination levels, independent of aerosol-generating procedures.
Findings
SARS-CoV-2 RNA contamination was most common in rooms of COVID-19 patients who did not undergo aerosol-generating procedures.
Emergency department surfaces are at high risk for SARS-CoV-2 contamination.
The presence of viable virus was confirmed on contaminated surfaces.
Abstract
Emergency departments are high-risk settings for severe acute respiratory coronavirus virus 2 (SARS-CoV-2) surface contamination. Environmental surface samples were obtained in rooms with patients suspected of having COVID-19 who did or did not undergo aerosol-generating procedures (AGPs). SARS-CoV-2 RNA surface contamination was most frequent in rooms occupied by coronavirus disease 2019 (COVID-19) patients who received no AGPs.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1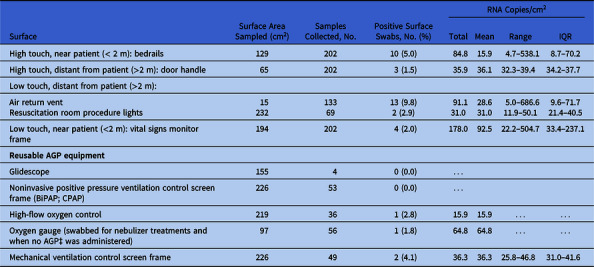 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInfection Control and Ventilation · COVID-19 and healthcare impacts · Infection Control in Healthcare
The emergency department (ED) serves as the gateway for hospital admission for severe coronavirus disease 2019 (COVID-19). Many of these patients require respiratory aid via aerosol-generating procedures (AGPs), which can contaminate environmental surfaces through aerosol deposition. Severe acute respiratory coronavirus virus 2 (SARS-CoV-2) environmental contamination after procedures carries implications for transmission, and characterizing this contamination can guide infection prevention practices. We determined the occurrence and viability of SARS-CoV-2 on ED surfaces when COVID-19 patients did and did not receive AGPs.
Methods
Patients presenting to the Yale New Haven Hospital Adult ED, composed of 101 beds across 2 campuses, were evaluated for COVID-19. From January through December 2021, environmental swabs were collected from a convenience sample of rooms housing patients actively infected with or under investigation for COVID-19. Sampling was prioritized for rooms of patients receiving AGPs. AGPs were classified as endotracheal intubation or extubation, manual bag-valve-mask (BVM) ventilation, cardiopulmonary resuscitation, noninvasive positive-pressure ventilation (NPPV), high-flow oxygenation, bronchoscopy, and nebulizer therapy.^ 1 ^
From each room, 5 samples were collected while occupied by the patient or immediately following discharge or transfer, but prior to cleaning. Among these samples, 4 were from fixed surfaces, selected based on touch frequency and aerosol source proximity: high-touch surfaces within and farther than 2 m (6 feet) from the patient (bedrail, door handle, respectively), and low-touch surfaces within and farther than 2 m (6 feet) from the patient: vital signs monitor frame, air return vent (standard rooms) or procedure light (resuscitation rooms), respectively. A fifth sample was taken from the reusable AGP equipment or oxygen gauge behind the bed. Surface swabs underwent RNA extraction and RT-qPCR using N1 primers, and RNA copies were quantified via a standard curve using controls of known copy number. Positive samples were cultured using Vero E6 cells and were examined for cytopathic effect. Severity was classified using a previously validated COVID-19 ordinal severity index.^ 2 ^ Differences between AGP and non-AGP room SARS-CoV-2 RNA contamination frequency were analyzed with the Fisher exact test and concentrations were analyzed with the Kruskal-Wallis test. Additional methods are in the Supplementary Material (online).
Results
Sample collection yielded 1,010 environmental specimens from 202 rooms. Room types included resuscitation bays (n = 69, 34.2%), airborne-infection isolation rooms (n = 56, 27.7%), and standard rooms (n = 77, 38.1%). AGPs were performed in 157 rooms (77.7%), and included intubation (n = 52), NPPV (n = 47 BiPAP and 2 CPAP), high-flow oxygenation (n = 34), nebulizer therapy (n = 13), and BVM ventilation (n = 1), or multiple AGPs (n = 8). Of 202 rooms, 87 housed SARS-CoV-2–positive patients (43.1%), approximately half of whom received AGPs (n = 42, 48.3%). These included high-flow oxygenation (n = 28), NPPV (n = 4), nebulizers (n = 4), intubation (n = 4), or multiple (n = 2).
In total, 36 swabs (3.6%, n = 1,010) from 29 rooms (14.4%, n = 202) were positive for SARS-CoV-2 RNA (Table 1). Of 87 COVID-19 patient rooms, 19 (21.8%) had SARS-CoV-2 RNA on at least 1 surface, including 13 rooms (28.9%, n = 45) where AGPs were not performed and 6 rooms (14.3%, n = 42) where AGPs were performed (P = .123). Patients spent more time in the room prior to environmental swab collection when surfaces were SARS-CoV-2 RNA-positive (mean, 295.4 minutes; n = 19) versus negative (mean, 223.8 minutes; n = 68), but this was not statistically significant (P = .213). SARS-CoV-2 RNA was detected in 10 rooms (8.7%, n = 115) occupied by SARS-CoV-2–negative patients. The mean estimated concentration of SARS-CoV-2 RNA on contaminated surfaces was 24.1 (median, 20.2) copies per 100 cm^2^ in rooms housing SARS-CoV-2–negative patients, 52.1 (median, 48.1) copies per 100 cm^2^ in rooms housing COVID-19 patients who underwent AGPs, and 147.6 (median, 43.7) copies per 100 cm^2^ in rooms housing COVID-19 patients who did not undergo an AGP (P = .239).
Table 1.Percentage of Rooms and Surface Swabs Testing Positive for SARS-CoV-2 RNA or Infectious Virus by RT-qPCR or CultureCOVID-19 StatusAerosol-Generating Procedure (AGP)Rooms Sampled,No.Rooms (%) Positive for SARS-CoV-2 RNA,No. (%)Swabs Collected, No.Swabs Positive for SARS-CoV-2 RNA,No. (%)Average SARS-CoV-2 RNA Copies per 100 cm^2^ Swabbed Surface Area^ a ^ Swabs Positive by Viral Tissue Culture, No.PositiveYes426 (14.3)2108 (3.8)52.10PositiveNo4513 (28.9)22516 (7.1)147.61NegativeYes11510 (8.7)57512 (2.1)24.10Total20229 (14.4)1,01036 (3.6) 1 Note. RT-qPCR, reverse-transcription quantitative polymerase chain reaction. a Mean copies, as determined by RT-qPCR curve determined from known quantities of PCR.
Of the 6 SARS-CoV-2 RNA-contaminated rooms of SARS-CoV-2–positive patients where AGPs occurred, high-flow oxygenation occurred in 5 rooms (n = 28), and nebulizer therapy occurred in 1 room (n = 4). No SARS-CoV-2–positive patient room surfaces were contaminated after intubation (n = 4) or NPPV (n = 4).
SARS-CoV-2 RNA was most frequently detected on air-duct return vents (13 of 133, 9.8%), followed by bedrails (10 of 202, 5.0%), reusable equipment (4 of 202, 2.0%), monitors (4 of 202, 2.0%), door handles (3 of 202, 1.5%), and procedure lights (2 of 69, 2.9%) (Table 2). SARS-CoV-2 RNA contamination ranged from 5–687 copies per 100 cm^2^ on vents, 6–74 copies per 100 cm^2^ on bedrails, 32–39 copies per 100 cm^2^ on door handles, 16–65 copies/100 cm^2^ on reusable equipment, and 22–504 copies per 100 cm^2^ on the monitor frame (Table 2 and Supplementary Table 1 online). Most contaminated rooms had only 1 SARS-CoV-2–positive surface; however, 6 rooms had multiple positive surfaces. A higher percentage of nonresuscitation rooms were positive (17.9%, n = 24 of 134) than resuscitation rooms (7.4%, n = 5 of 68; P = .055).
Table 2.Emergency Department Room Surfaces Positive for SARS-CoV-2 ContaminationRNA Copies/cm^2^ SurfaceSurface Area Sampled (cm^2^)Samples Collected, No.Positive Surface Swabs, No. (%)TotalMeanRangeIQRHigh touch, near patient (< 2 m): bedrails12920210 (5.0)84.815.94.7–538.18.7–70.2High touch, distant from patient (>2 m): door handle652023 (1.5)35.936.132.3–39.434.2–37.7Low touch, distant from patient (>2 m):Air return ventResuscitation room procedure lights152321336913 (9.8)2 (2.9)91.131.028.631.05.0–686.611.9–50.19.6–71.721.4–40.5Low touch, near patient (<2 m): vital signs monitor frame1942024 (2.0)178.092.522.2–504.733.4–237.1 Reusable AGP equipment Glidescope15540 (0.0)…Noninvasive positive pressure ventilation control screen frame (BiPAP; CPAP)226530 (0.0)…High-flow oxygen control219361 (2.8)15.915.9……Oxygen gauge (swabbed for nebulizer treatments and when no AGP‡ was administered)97561 (1.8)64.864.8……Mechanical ventilation control screen frame226492 (4.1)36.336.325.8–46.831.0–41.6Note. BiPAP, bilevel positive airway pressure; CPAP, continuous positive airway pressure; AGP, aerosol-generating procedure.
Of the 36 SARS-CoV-2 RNA-positive samples (bedrail, non-AGP COVID-19 patient), 1 sample was positive by viral tissue culture, exhibiting extensive cytopathic effect. SARS-CoV-2 RNA copy number in pre- and post-incubation tissue culture medium went from undetectable to 3.5 × 10^8^ copies, respectively.
COVID-19 patients occupied 13 of the 202 sampled rooms (6.4%) immediately preceding the occupant present during sampling. One of these rooms had an equipment surface positive for SARS-CoV-2 RNA while occupied by the subsequent SARS-CoV-2–negative patient.
The median severity of patient illness on arrival was 5.0 (IQR, 2.5–6.0) in rooms with SARS-CoV-2 contamination compared to 6.0 (IQR, 4.75–6.0) in rooms without contamination (P = .259). The median number of days from symptom onset to ED presentation was 4.0 (IQR, 3.0–7.0) in rooms with detectable SARS-CoV-2 contamination compared to 7.0 (IQR, 3.0–8.5) in rooms without (P = .507) (Supplementary Fig. 1A and B online).
Discussion
SARS-CoV-2 RNA contamination was detected on at least 1 surface in >20% of rooms housing patients with COVID-19. Surface contamination was detected more frequently in rooms of COVID-19 patients who did not have an AGP. We suspect that this finding is due to the natural progression of COVID-19 in which viral loads peak around symptom onset, and more severe disease occurs later in the hyperinflammatory phase of illness when viral load is diminished.^ 3,4 ^ This carries infection control implications; mitigating transmission earlier in the disease course when viral transmission potential is greatest may be more impactful, regardless of aerosol deposition.
We observed SARS-CoV-2 contamination in 9% of SARS-CoV-2–negative patient rooms. Given the rapid turnover of ED rooms, prior patients could have contributed to contamination, especially on air-return vents because these are not disinfected between patients. This finding also highlights the ability of upward airflow, even in rooms maintained without negative pressure, to move SARS-CoV-2 aerosols to surfaces unlikely to be implicated in viral transmission.
One sample grew SARS-CoV-2 in tissue culture. Infectious virus has rarely been recovered from hospital surfaces, and positive surfaces are typically within close range of the patient.^ 5–7 ^ SARS-CoV-2 remains viable on surfaces up to 21 days, with a half-life of ∼2–5 days,^ 8 ^ whereas SARS-CoV-2 RNA exhibits a 1-log reduction over the same period.^ 9 ^ Therefore, failure to detect viable virus in more samples with high viral concentrations is not unexpected and supports the evidence of a minimal role of surface and fomite transmission in SARS-CoV-2 spread.^ 10 ^ Study limitations include observations at a single emergency department and limited comparisons between AGPs due to small sample sizes. It is unclear whether these findings would be replicated in asymptomatic COVID-19 populations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical questions about COVID-19: questions and answers. Centers for Disease Control and Prevention website. https://www.cdc.gov/coronavirus/2019-ncov/hcp/faq.html. Accessed May 2, 2022.
- 2Beigel JH , Tomashek KM , Dodd LE , et al. Remdesivir for the treatment of COVID-19—final report. N Engl J Med 2020;383:1813–1826.32445440 10.1056/NEJ Moa 2007764 PMC 7262788 · doi ↗ · pubmed ↗
- 3Jones TC , Biele G , Mühlemann B , et al. Estimating infectiousness throughout SARS-Co V-2 infection course. Science 2021;373:eabi 5273.34035154 10.1126/science.abi 5273 PMC 9267347 · doi ↗ · pubmed ↗
- 4Junqueira C , Crespo  , Ranjbar S , et al. FcγR-mediated SARS-Co V-2 infection of monocytes activates inflammation. Nature 2022;606:576–584.35385861 10.1038/s 41586-022-04702-4PMC 10071495 · doi ↗ · pubmed ↗
- 5Warren BG , Nelson A , Barrett A , et al. Severe acute respiratory syndrome coronavirus 2 environmental contamination in hospital rooms is uncommon using viral culture techniques. Clin Infect Dis 2022;75:e 307–e 309.35023553 10.1093/cid/ciac 023PMC 8807208 · doi ↗ · pubmed ↗
- 6Nagle S , Tandjaoui-Lambiotte Y , Boubaya M , et al. Environmental SARS-Co V-2 contamination in hospital rooms of patients with acute COVID-19. J Hosp Infect 2022;126:116–122.35569577 10.1016/j.jhin.2022.05.003PMC 9098885 · doi ↗ · pubmed ↗
- 7Geng Y , Wang Y. Stability and transmissibility of SARS-Co V-2 in the environment. J Med Virol 2023;95:e 28103.36039831 10.1002/jmv.28103 PMC 9537778 · doi ↗ · pubmed ↗
- 8Baker CA , Gibson KE. Persistence of SARS-Co V-2 on surfaces and relevance to the food industry. Curr Opin Food Sci 2022;47:100875.35784376 10.1016/j.cofs.2022.100875 PMC 9238272 · doi ↗ · pubmed ↗