Superior vena cava coil left alone in the innominate vein: successful removal by a combined approach via jugular and femoral veins
Kenji Kuroki, Yukio Sekiguchi, Kazutaka Aonuma, Akira Sato

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
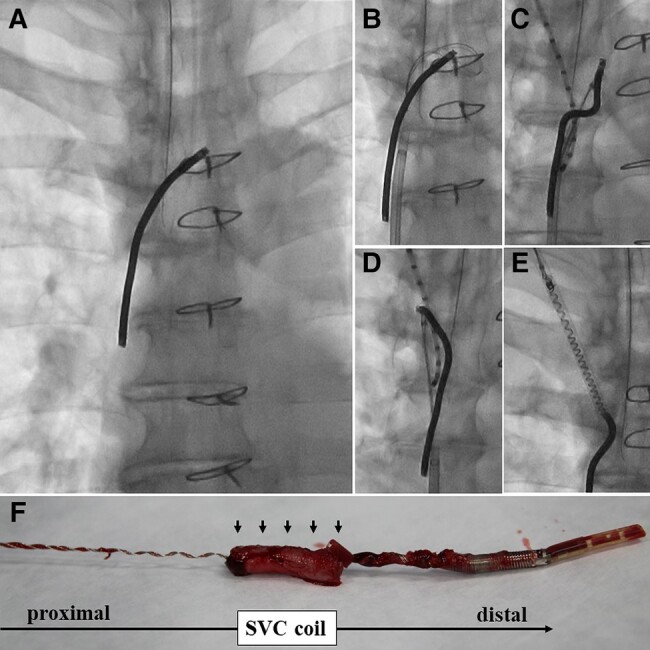 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCentral Venous Catheters and Hemodialysis · Vascular anomalies and interventions · Venous Thromboembolism Diagnosis and Management
The extraction of migrating leads is technically challenging, especially when a superior vena cava (SVC) coil was left alone in the innominate vein.
A 56-year-old man with Brugada syndrome developed a delayed cardiac tamponade due to perforation of the right ventricle (RV) defibrillation lead (Riata 1580, Abbott) implanted 10 years ago. The RV was surgically repaired, and the RV lead was resected at the right atrium (RA) level. One year later, he was referred to our hospital to undergo lead extraction due to pocket infection. A locking stylet was developed at the lead’s distal end, which could not be captured by a snare catheter inserted via the femoral access because the distal end was resected just below the level adherent to the RA. A 14-Fr laser sheath was advanced to one-third of the SVC coil when the lead was broken (Panel A). The snare catheter was advanced to the innominate vein to grab the proximal end of the SVC coil (Panel B). The proximal coil was seized using the snare with the support of the deflectable catheter inserted from the internal jugular vein (Panel C), and the coil was moved into the jugular vein (Panel D; Supplementary material online, Video S1). The coil was grabbed with the snare catheter advanced via the internal jugular access, but the coil was easily untied gradually by pulling it (Panel E; Supplementary material online, Video S2). With continuous mild traction, the entire coil was finally pulled out of the body. The SVC coil with massive adhesion (arrows) had been untied almost entirely (Panel F).
Supplementary Material
ytae077_Supplementary_DataClick here for additional data file.