Evaluation after implementation of chemical bowel preparation for surgical site infections in elective colorectal cancer surgery and role of antimicrobial stewardship pharmacist: Retrospective cohort study
Yasuhiro Sasaki, Akira Kurishima, Chieko Miyamoto, Kenichiro Hataji, Toru Tezuka, Hideo Katsuragawa

TL;DR
This study found that chemical bowel preparation and laparoscopic surgery reduced surgical site infections in colorectal cancer patients, with antimicrobial stewardship pharmacists playing a key role in implementing these changes.
Contribution
The study demonstrates the effectiveness of chemical bowel preparation and the impact of antimicrobial stewardship pharmacists in reducing surgical site infections.
Findings
Female sex, laparoscopy, and chemical bowel preparation were associated with reduced surgical site infections.
Modifying the clinical pathway led to a significantly shorter postoperative hospital stay.
Antimicrobial stewardship pharmacists helped implement and validate the effectiveness of chemical bowel preparation.
Abstract
We evaluated the predictive factors for surgical site infections (SSIs) in elective colorectal cancer surgery and the role of antimicrobial stewardship (AS) pharmacists in modifying the clinical pathway. Between February 2017 and January 2022, 414 elective colorectal cancer surgeries were performed. The results of multivariate analysis by SSI incidence were adjusted odds ratio (aOR): 0.45; 95% confidence interval (CI): 0.22–0.96 (P = 0.039) for sex (female), aOR: 0.27; 95% CI: 0.13–0.58 (P < 0.001) for laparoscopy, aOR: 0.42; 95% CI: 0.19–0.91 (P = 0.029) for chemical bowel preparation. The median (interquartile range) postoperative length of stay was 12 (10.0–18.5) vs. 10 (9.0–13.0) days before and after the clinical pathway was modified (P < 0.001). The role of AS pharmacists was primarily to conduct a literature search to explore whether SSIs could be ameliorated by…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
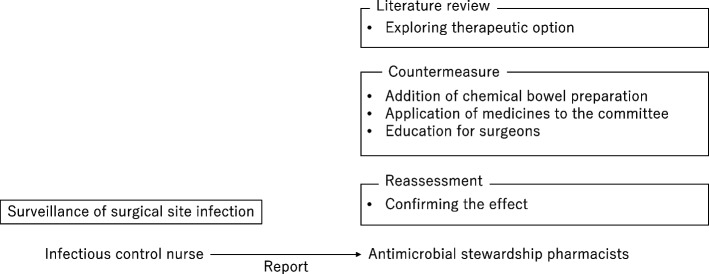 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSurgical site infection prevention · Cardiac, Anesthesia and Surgical Outcomes · Anesthesia and Pain Management
Background
In 2016, the Japanese Society of Chemotherapy and the Japan Society for Surgical Infection jointly published practical guidelines for the use of prophylactic antibiotics to prevent postoperative infections [1]. Although parallel efforts by pharmacists toward appropriate prophylactic antibiotic use have been reported [2], reports on pharmacists’ efforts to prevent surgical site infections (SSIs) are scarce [3].
SSI prevention strategies include blood glucose control, normothermia maintenance [4], appropriate antimicrobial agent selection, timing of administration, and duration of therapy. It is recommended that prophylactic antimicrobial agents be combined with oral antimicrobial agents [1]. However, according to the results of a survey conducted in 2015, few facilities in Japan have adopted this approach [5].
At Tokyo Metropolitan Organization Tama-Nambu Chiiki Hospital, a pharmacist began providing full-time antimicrobial stewardship (AS) services in 2019. Prior to this, the pharmacist sorted out the in-hospital adoption of intravenous antimicrobial agents, post-prescription audits and feedback for broad-spectrum antimicrobial agents [6], as well as actively intervene in blood culture-positive patients [7]. Mid- to long-term intervention with intravenous antimicrobial agents decreases the resistance rate of Pseudomonas aeruginosa [8]. AS pharmacists reconsidered their SSI countermeasures after receiving a report from an infection control nurse (ICN), stating that SSI incidence in patients undergoing colorectal cancer surgery was high.
This study aimed to evaluate the efficacy of additional chemical bowel preparation for SSI prophylaxis in elective colorectal cancer surgery and report the role of dedicated AS pharmacists in modifying the clinical pathway.
Main text
This retrospective cohort study was conducted at Tokyo Metropolitan Organization Tama-Nambu Chiiki Hospital, a 287-bed secondary emergency medical care facility in Tama, Tokyo, Japan, with no infectious disease physicians. Patients who underwent elective colorectal cancer surgery between January 2017 and January 2022 were included. Exclusion criteria included cases involving multiple surgeries. Modifications to the clinical pathway were implemented in June 2019. SSIs were evaluated in 414 cases (224 before and 190 after clinical pathway modification) based on sex, age, diabetes status, smoking status, surgical site (colon or rectum), wound class, American Society of Anesthesiologists physical status (ASA-PS) classification [9], laparoscopic surgery, stoma construction, mechanical bowel preparation, and chemical bowel preparation. SSIs were assessed from medical records by the ICN based on these criteria (Supplement 1) [4].
Potential risk factors associated with SSIs for each procedure type were assessed using univariate modeling analysis. Categorical variables were compared using the x^2^ test. Variables with a p-value < 0.2 in the univariate modeling analysis were considered potential independent variables and were entered into the logistic regression model. A multivariate model was developed using a forward stepwise logistic regression. Variables were retained in the final model if the 2-tailed p-value < 0.05. The Mann–Whitney U test was performed for postoperative hospital stay and total medical fees. Statistical analysis was performed using JMP, version 14.2.0 (JMP). The Institutional Review Board of Tokyo Metropolitan Tama-Nambu Chiiki Hospital approved this study.
Table 1 shows the patient characteristics. SSI incidence during the study period was 9.9% (41 of 414 cases). Univariate logistic regression analysis demonstrated statistical significance for sex (P = 0.018), smoking status (P = 0.025), wound class (P = 0.007), ASA-PS (P = 0.114), laparoscopy (P < 0.001), and chemical bowel preparation (P = 0.012). The results of multivariate logistic regression analysis adjusting for sex, smoking status, wound class, ASA-PS, laparoscopy, and chemical bowel preparation showed sex (female) (adjusted odds ratio [aOR], 0.45 [95% CI, 0.22–0.96], P = 0.039), laparoscopy (aOR, 0.27 [95% CI, 0.13–0.58], P < 0.001), and chemical bowel preparation (aOR 0.42 [95% CI, 0.19–0.91], P = 0.029) (Table 2). The SSI incidence rates were 12.5% (28 of 224 cases) before modification and 6.8% (13 of 190 cases) after. The median (interquartile range [IQR]) postoperative hospital stay was 12 days (10.0–18.5) before modification and 10 days (9.0–13.0) after (statistically significant; P < 0.001). The total medical fee (IQR) was 1,490,620 yen (1,291,080–1,779,790) before modification and 1,390,110 yen (1,291,460–1,676,230) after (P = 0.066). Adverse reactions after mechanical and chemical bowel preparations included anaphylactic shock (1 case). Table 1. Baseline and clinical characteristics of the study population analyzed using Pearson's chi-square testCharacteristics, n (%)Patient undergoing elective colorectal surgery (N = 414)pSSI ( +) (N = 41)SSI (-) (N = 373)Female sex13 (31.7%)191 (51.2%)0.018Age ≥ 6035 (85.4%)322 (77.8%)0.865Diabetes10 (24.4%)64 (17.2%)0.251Smoking11 (26.8%)51 (13.7%)0.025Location Colon31 (75.6%)269 (72.1%)0.635 Rectum10 (24.4%)104 (27.9%)Wound class Clean-contaminated39 (95.1%)371 (99.5%)0.007 Dirty-infected2 (4.9%)2 (0.5%)ASA-PS 11 (2.4%)38 (10.2%)0.114 235 (85.4%)312 (83.7%) 35 (12.2%)23 (6.2%)Laparoscopy26 (63.4%)316 (84.7%) < 0.001Stoma construction8 (19.5%)54 (14.5%)0.391Mechanical bowel preparation30 (73.2%)267 (71.6%)0.830Chemical bowel preparation9 (2.2%)158 (38.2%)0.012SSI surgical site infection, ASA-PS American Society of Anesthesiologists physical statusTable 2Multivariate analysis for factors independently associated with surgical site infection in colorectal surgeryCharacteristicAdjusted odds ratio (95% CI)Female sex0.45 (0.22–0.96)Laparoscopy0.27 (0.13–0.58)Chemical bowel preparation0.42 (0.19–0.91)Bivariate analyses were analyzed using Fisher's exact tests. Variables with a p < 0.20 by bivariate analysis were included in multivariable model selection. Model selection was conducted using stepwise logistic regression and consideration of 2-way interaction terms. The level of significance was set at α = 0.05Abbreviation: CI confidence interval
The role of AS pharmacists was to explore whether SSIs in patients undergoing elective colorectal cancer surgery could be ameliorated with pharmacotherapy, to coordinate with the relevant departments, and to educate surgeons (Fig. 1). Adding chemical bowel preparation to prophylactic antimicrobials in elective colorectal cancer surgery has been reported to decrease SSI incidences [10]. In response, AS pharmacists decided to add chemical bowel preparations (a single dose of kanamycin [1000 mg] and metronidazole [750 mg] administered orally at 18:00 and 22:00 the day before surgery) and shorten the duration of intravenous antimicrobial use from 48–72 h post-surgery to ≤ 1 day post-surgery. The usefulness of the chemical bowel preparation, expected side effects, and modifications in the clinical pathway were explained by the AS pharmacist and approved at the surgical conference. When adding chemical bowel preparation, an application for adopting a new agent for kanamycin was submitted to the Pharmaceutical Affairs Committee and an off-label application to the Ethics Review Committee by an AS pharmacist in advance. Finally, chemical bowel preparation was added in June 2019.Fig. 1. Role of antimicrobial stewardship pharmacists in preventing surgical site infections in elective colorectal surgery
AS pharmacists have led the addition of chemical bowel preparation and shortened intravenous antibiotic administration in the clinical pathway for elective colorectal cancer surgery. Chemical bowel preparation, sex, and laparoscopy were the relevant exploratory factors for SSIs. After modifications, the number of postoperative hospital stays was reduced and SSI incidence was lower. Since shortening the intravenous antibiotic administration time has no effect on SSIs [11], this is unlikely to contribute a lower SSI incidence. The role of AS pharmacists in adding chemical bowel preparation ranged from the exploration of effective pharmacotherapy for SSI prevention to the epidemiological verification of its effectiveness. AS pharmacists taking the initiative to change clinical pathways may contribute to the efficacy of medical therapies.
As pharmacotherapy is the core of treatment, pharmacists should take the initiative to change or evaluate treatment [12]. The clinical pathways through which pharmacists take the initiative have been reported for perioperative thromboprophylaxis [13] and postoperative pain relief [14]. In Japan, reports exist on the clinical pathways taken by pharmacists, including the development of criteria for treatment after surgery to standardize medical care [15] and supportive care for cancer chemotherapy [16]; however, similar efforts for SSI prevention do not exist. The role of pharmacists in clinical pathways for SSIs may not be recognized in Japan, given that the main methods to prevent SSIs are normothermia, appropriate antiseptic use, and postoperative blood glucose control [17]. The AS pharmacist introduced chemical bowel preparation after a literature review was triggered by ICN surveillance reports. AS pharmacists should regularly communicate with other professionals and to determine whether they can contribute to pharmacotherapy. Deciding in advance the appropriate antimicrobial selection and administration timing by pharmacists and educating physicians is the simplest way to resolve the inappropriate selection and timing of perioperative antimicrobials [18, 19] that many institutions experience.
Risk factors for SSIs in elective colorectal cancer surgery include chemical bowel preparation [20], use of laparoscopy [21], and sex [22]. In this study, adjustable chemical bowel procedures decreased the incidence of SSIs. The confirmation of the expected effects is another important task for pharmacists. The use of laparoscopy to reduce SSI incidence has also been reported [23]. Therefore, the appropriateness of laparoscopy should be evaluated for each institution. Similar to the rates in our study, 77.5% of laparoscopic procedures are performed in the rectum and 61.5% in the colon [24]. The association regarding sex is well known, but the reasons are not known [22].
This study has several limitations. First, this was a retrospective cohort study, and confounding factors that have not been investigated may have reduced the efficacy of chemical bowel preparation for SSIs. Certain risk factors associated with SSI, such as perioperative hyperglycemia, hypothermia, and operative time, were not examined in this study. Second, SSIs were assessed from medical records by the ICN, and may be underestimated. However, previous studies have reported similar results [25]. Third, whether the role of AS pharmacists is transferable to other facilities is uncertain because of differences between stakeholders.
Conclusions
AS pharmacists led addition of chemical bowel preparation in the clinical pathway for elective colorectal cancer surgery. Our results showed that sex, laparoscopy use, and chemical bowel preparation were prognostic factors of SSI. This study is the first report of AS pharmacists in Japan improving the SSI rate by modifying the clinical pathway. The role of AS pharmacists was primarily to conduct a literature search to explore whether SSIs could be ameliorated by pharmacotherapy, coordinate the addition of chemical bowel preparation, and epidemiologically confirm their effectiveness.
Supplementary Information
Additional file 1.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1J Infect Chemother. https://www.chemotherapy.or.jp/uploads/files/guideline/jyutsugo_shiyou_jissen.pdf, Accessed 13 Nov 2023
- 2Kohei K Hiroki H Keiji M Hiroaki H Effect of prescription proposal using the electronic medical record by ward pharmacists for proper use of antimicrobial prophylaxis for surgery J Jpn Soc Surg Infect 202017167171
- 3Fésüs A BenkőR Matuz M Kungler-Gorácz OFésüs MÁBazsóT The effect of pharmacist-led intervention on surgical antibacterial prophylaxis (SAP) at an orthopedic unit Antibiotics (Basel)202110150910.3390/antibiotics 1012150934943721 PMC 8698705 · doi ↗ · pubmed ↗
- 4Berríos-Torres SI Umscheid CA Bratzler DW Leas B Stone EC Kelz RR Centers for Disease Control and Prevention guideline for the prevention of surgical site infection, 2017 JAMA Surg 201715278479110.1001/jamasurg.2017.090428467526 · doi ↗ · pubmed ↗
- 5Makoto W Masahiko M Takeshi A Keiichi T Masamichi Y Tadahiko M The current perioperative care in elective colorectal surgery in Japan: A questionnaire survey of members of the Tokyo colon seminar committee J Jpn Soc Coloproctol 20156839140210.3862/jcoloproctology.68.391 · doi ↗
- 6Yasuhiro S Ayumi K Akiko Y Masataka Y Impact of an antimicrobial stewardship program Introduced Pharm Jpn J Infect Prev Control 20173236937310.4058/jsei.32.369 · doi ↗
- 7Yasuhiro S Misato A Ayumi K Akiko Y Hirobumi T Masataka Y Impact of an antimicrobial stewardship pharmacist’s intervention on blood culture-positive patients Japanese J Infect Prev Control 20203515716210.4058/jsei.35.157 · doi ↗
- 8Sasaki Y Kurishima A Amano M Kanamaru A Yamakuchi A Takayasu H Impact of pharmacist initiated antimicrobial stewardship program ~Evaluation of antimicrobial resistance rate at three years after intervention~Jpn J Infect Prev Control 20203520120510.4058/jsei.35.201 · doi ↗