The male-focused marital relationship enrichment and sexual well-being interventions: A scoping review
Solmaz Abdollahzadeh Sardehaei, Effat Merghati Khoei, Beheshteh Niusha, Zahed Rezaei

TL;DR
This review explores interventions aimed at improving men's marital and sexual well-being, highlighting the need for more male-focused programs.
Contribution
The study provides a scoping review of interventions targeting men's sexual and marital health, emphasizing cultural and gender-specific approaches.
Findings
Only 8 studies met the inclusion criteria, with most focusing on sexual and reproductive health programs.
Most studies involved heterosexual couples, suggesting a need for more inclusive male-focused interventions.
Four studies were rated as high quality, indicating some effective methods exist but more research is needed.
Abstract
There is an increasing need for sexual well-being and health promotion strategies that effectively engage men. Researchers have evaluated the efficacy of sexual and reproductive health-related and marital enhancement interventions in male-dominated societies. However, few have focused on culturally appropriate and gender-specific program effects. This review aims to evaluate evidence of existing interventions aimed at enriching marital relationships and sexual well-being in adult men. This scoping review was conducted by searching various databases (CINAHL, PsycINFO, EMBASE, Google Scholar, PubMed, Scopus, SID, and Noormags), and other available resources in both English and Persian languages. We located all publications up to January 2023 with no time restriction. Inclusion criteria were studies targeting men in the enrichment of marital and sexual relationships, which focus on…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
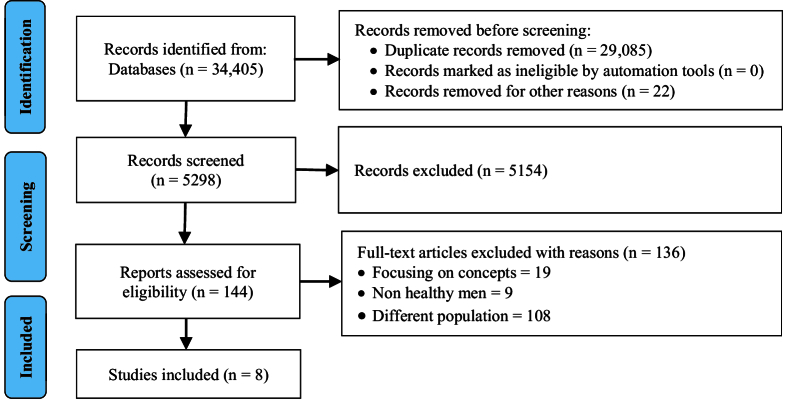 Figure 1
Figure 1|
| |||||
|
|
|
|
|
|
|
|
| A systematic review | Male refugees age | Intervention primary/secondary humanitarian settings IPV prevention. Exploring the effectiveness of existing IPV-related interventions | Primary or secondary IPV | -IPV management policy and associated planning -Decreasing violence against women among refugees, internally displaced persons, and conflict-affected population -Guideline for researchers, policymakers, and strategy developers |
|
| RCT with a control group follow-up after 2 months | 100 Men Age: 45-55 Intervention group #50 Control group#50 | Intervention: Education regarding menopausal health 3 sessions (60-min) sessions Conducted using speech | Men's knowledge of menopausal health Women's marital satisfaction Menopause knowledge and ENRICH marital satisfaction questionnaire | The knowledge of menopausal health and women's marital satisfaction scores were |
|
| A quasi-experimental Non equivalent control group | 80 Married men Age: 20-55 | Intervention: Combination of psycho-physiological therapy (Stretching therapy combined + with breathing exercises) 90-120 min 3 days a week 20 sessions conducted in a clinic at the hospital | Sexual satisfaction The ENRICH questionnaire | -The intervention group post-test scores |
|
| A quasi-experimental 6 month follow up | 780 Men Age: 14-25 | Intervention: Horizons and Institute Promundo Intervention 1: Interactive group education sessions Intervention 2: Community-wide “lifestyle” social marketing campaign to promote the usage of condom Intervention 3: Morro dos Macacos, a delayed intervention that followed the control period 6 group education sessions 2 supervisors held weekly Conducted by the group education sessions | -Key HIV/STI-related topics -Gender norms attitudes -The gender-equitable men scale | -A variety of key HIV/STI-related outcomes improved -Reduced HIV/STI risk was associated with |
|
| Cluster RCT With a control group Follow up: 3-month 9-month | 866 Boys Age: 13-19 | Intervention Manhood 2.0 a gender-transformative program and job-readiness training program for the control group 6 sessions of 3 hr Once or twice a week Conducted by youth-serving organizations and community | Primary outcome: ARA or SV perpetration exploratory outcome: sexual/physical intimate violence for a partner, non-partner SV, any SV, sexual harassment, dating or cyber-sexual abuse, and incapacitated sex. Secondary outcomes: attitudes about gender equality, ARA recognition, intention to intervene with peers, condom negotiation self-efficacy. A scale to measure participants' views on gender norms/A scale to measure the ability of participants to understand harmful actions committed against a partner as abusive/A scale to measure the probability that a participant would intervene when witnessing damaging behaviors in male peers. A scale for assessing participants' confidence in negotiating condom use with a partner. A scale for assessing participants' views on the use of condoms and contraceptives | -Gender-based violence was |
|
| A mixed-methods study with a control group Follow up: Only a post-intervention follow-up group | 110 Men Age: 15-18 IG#56 CG#54 | Intervention: 2.0-an SRH program (group-based+ after-school) targeting young Black and Latino men. (Evaluating the feasibility, quality, and preliminary efficacy) 6 sessions monthly Conducted by: youth center researchers/transcribed recordings (450 min) | Self-efficacy contraception knowledge; SRH information; positive attitudes for supporting partners in the prevention of pregnancy. Gender norms (GEM scale) social competence scale | -The manhood 2.0 program is feasible for delivering unintended pregnancy prevention programming to young men. -SRH information; contraception knowledge; positive attitudes for supporting partners in pregnancy prevention; self-efficacy in partner communication about sex; discussing program content with friends and family; and social competence and support |
|
| Cluster RCT with a control group Follow up 3 months | 2600 Boys Age: | Intervention: Exploring the effectiveness of a prevention program (dating violence perpetration) among young male athletes and coaches. 60-min training for coaches 11 “Training Cards”. (10-15 min) weekly Conducted by a trained violence prevention advocate to introduce the coaches Kit | Primary outcomes: gender-equitable attitudes and intentions to intervene, abusive behaviors recognition. Secondary outcomes: abuse perpetration and explored bystander behaviors, values for intentions to intervene, gender-equitable attitudes, and scales of negative bystander intervention | -Improved intentions to intervene, abusive behaviors recognition, and positive bystander intervention. DV perpetration and abuse perpetration were reduced. -No notable changes in gender-equitable attitudes + identification of abusive behaviors + DV perpetration were observed |
|
| A mixed method study 2 focus groups NO CG | 12 Men Age: 26-50 | Intervention: The ProSAAM a 5-yr study 3 programs + 2 wk of skills practice (between each session) conducted by 2 African American male facilitators At a church | Participants' enthusiasm for taking part in the marriage-strengthening program (ProSAAM) | Hearing the voices of a sample of the recruited population and searching for feedback about participating in a similar marriage enrichment program helped promote potential participants' enthusiasm for this marriage-strengthening program |
| IPV: Intimate partner violence, RCT: Randomized control trial, HIV: Human immunodeficiency virus, STI: Sexually transmitted infections, AIDS: Acquired immunodeficiency syndrome, ARA: Adolescent relationship abuse, SV: Sexual violence, IG: Intervention group, CG: Control group, SRH: Sexual and reproductive health, Gem: Gender-equitable men, DV: Dating violence, ProSAAM: Program for strong African American marriages | |||||
|
| |
|
| Medium |
|
| Low |
|
| Medium |
|
| Medium |
|
| Low |
|
| Low |
|
| Medium |
|
| Non |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAdolescent Sexual and Reproductive Health · Sexual function and dysfunction studies · Attachment and Relationship Dynamics
1. Introduction
“Education is not just the learning of facts, but the training of the mind to think and react”. Sexuality education is NO exception (Albert Einstein).
Men have limited access to sexual and reproductive health (SRH) services, or they are not motivated to use the existing programs offered by the communities, workplace, and social networks (1-5). No question that available male-centered programs throughout the settings are various. Culture and the context which a couple lives through, and the meanings attached to sexuality and reproduction make the variety. This verity also explains the couples' range of marital satisfaction (6, 7). The outcomes of good marital quality result in mental health, which means strength (e.g., sexual assertiveness, positive Adakpa, 2022 #4 expression), marital satisfaction, physical health, positive self-evaluation, fewer depression and mental illness symptoms, flexibility (e.g., positive sexual attitude, supporting the partner, mutual intimate relations), and self-efficacy (8, 9). The efficacy of SRH-related programs has been investigated in male-dominated societies (10, 11) but not focused on the gender-specificity of the program (12-14). Culturally sensitive gender-focused sexuality education can be more efficient when integrated into marital enhancement training programs advocated by professionals, governments, and SRH services (15-21). However, there is a profound gap in the body of knowledge that needs to be filled with more work. In a systematic review of studies examining interventions to improve SRH in men, 21 studies were identified investigating the effectiveness of sexual education and counseling on SRH-related outcomes (22, 23). In a recent comprehensive review of studies, life satisfaction, positive and negative emotions, and psychological well-being were pointed out as the domains of subjective well-being for men (24). The World Health Organization highlighted the impact of gender norms on men's behaviors so that it emphasizes gender-sensitive programs for men as the targets who need specific training programs to enhance their intimate partnership (25).
Considering the importance of SRH in men, we aimed to conduct this scoping review to get answers to our questions of interest: “what does the literature say about male partners' participation in the SRH programs in order to improve their marital and sexual relationships"?
2. Materials and Methods
We conducted this scoping review to identify the span and depth of our topic of study, summarize the evidence, and find gaps in existing literature (11, 16, 26, 27). We did an extensive search using electronic databases and other published resources in English and Persian with no time limitation. We developed a search strategy for MEDLINE, including Medical Subject Headings (MeSH), CINAHL, PsycINFO, EMBASE, Google Scholar, PubMed, Scopus, SID, and Noormags.
Article selection
We included the publications that evaluated the interventions targeting men. These interventions could be aimed either at improving men's sexual well-being or enhancing their marital relationships. 2 independent reviewers (EMK, SAZ) screened articles for inclusion and exclusion criteria using the customized extraction spreadsheets (Excel, Google Sheets). We employed PRISMA to ease transparent and inclusive reporting of this scoping review (Table I). We used the population, intervention, comparison/control and outcome framework to select interventions that directly relate to the marital and sexual matters of adult men. Our focus is on exploring the effectiveness of marital enhancement and sexuality education programs, and how these programs can improve men's sexual well-being and overall marital satisfaction.
Inclusion and exclusion criteria
We selected the studies based on the following criteria: (a) samples: healthy, adult married men; (b) aim of intervention: improving men's marital and sexual relationship and sexual well-being; (c) setting: any countries; (d) outcomes: marital OR sexual commitment, couple's intimacy, passionate relationship, or sexual satisfaction; and (e) study design: according to the goal of this review, all studies regardless of study design the marital relation enhancement and sexual well-being for adult men. We included studies if they introduced any program or intervention to enhance men's marital/sexual relations as well as men's overall sexual well-being. We excluded interventions, offered only to women or couples. We also excluded articles if 1) we could not find a full version of the article to review, and 2) articles in which no English or Persian version was available.
Data extraction and quality assessment
The characteristics of publication, study design, participants, and study concepts and outcomes, were extracted into Excel. The quality of selected articles was assessed independently by SAZ and EMK using the Joanna Briggs Institute (JBI) (28), a tool for assessing the quality of the selected studies, text, and expert opinion before inclusion in the review. We used JBI to reach a consensus decision on selecting the articles. According to the JBI assessment result, 4 articles were moderate (29-32) and 4 were high quality (33-36). In this review, we did not use meta-analysis due to the heterogeneity of the studies.
3. Results
Of 34,405 citations screened, we assessed 5298 articles, and 144 met our inclusion criteria. Consistent with our goal to scope the existing literature to demonstrate the state of interventions in marital and sexual enrichment for men, the study team selected 8 articles for data extraction and summarization (Figure 1).
Findings from the included studies indicated that a variety of strategies were offered within the majority of the articles. SRH program/information, intimate partner violence prevention, human immunodeficiency virus/sexually transmitted infections (HIV/STI)-related topics, gender norms, menopausal health, and prevention programs were the main focus of 6 articles. Marital and sexual enhancements were areas of focus in 2 studies, including marital satisfaction, sexual satisfaction, and marriage enrichment, which show promise for promoting men's sexual health, happiness, and quality of life (Table I). Research methods included 2 semi-experimental studies, 3 clinical trials, 1 systematic review, 1 content analysis, 1 mixed method. Programs included targets from different ethnic/cultural backgrounds. Almost half of the programs were conducted in developed countries 50% and 50% in undeveloped ones. Most often 62.5% of programs focused only on men from American societies and 37.5% from Asian societies.
Among these interventions 37.5% focused on clinical trials. The risk of bias using the Cochrane Collaboration tool: bias due to lack of blinding of study personnel, conflict of interest, and selective reporting of exposures was low. Bias due to exposure misclassification, incomplete exposure data in the selection of participants in the study, and differences in numerator and denominator were medium (Table II).
PRISMA flow diagram.
4. Discussion
In this scoping review, we visually presented the result of complex and limited studies in the field of male-focused marital and sexual well-being interventions. As reflected by the small fraction that was accessible during our review, our findings suggest a prevalent lack of transparency in the conduct and reporting of male-focused programs in enhancing men's marital and sexual relationships, in developing countries. Several explanations have been pointed out for this limitation, such as gender norms that are dismissed in many research contexts. Some reports support our findings. These findings have pointed out gender norm-related beliefs and attitudes as influencing factors on men's participation in research (37). For instance, many family planning programs focus on women's participation, while most contraceptive methods are directly utilized by men (e.g., male condoms, vasectomy, withdrawal) (38).
Others argue that the lack of men's participation is justified because women are considered contraceptive users or must learn more than men because they are the ones falling pregnant. It seems that lack of attention to gender norms in the programs related to SRH or marital satisfaction enrichment makes the intervention ineffective and demotivates men from active participation in the related research.
Most programs, in male-dominated societies in particular, are implemented based on the perspective that women must learn to serve their male partners (38, 39), women should learn how to gratify their husbands sexually (40), or women should learn to elevate the quality of their marital life because women are considered vulnerable than men (41, 42). Other scholars highlighted the gender differences in marital construction (42). In this line, some emphasize gender norms and their powerful influence throughout marital life. In this study with couples, women's roles are significant in marital problem-solving, and somehow men are drawn out of the scene (43). In conservative and androcentric cultures, some connotations affect the societal mindsets and encourage the belief that the man is the breadwinner, and the woman is the counterpart who should learn to perform her duties as the housewife, mother, etc. (44). This paradigm can increase men's feelings of isolation resulting in limited participation of men in research (45). Findings identified that sociocultural and psychological norms are also influencing matters. The Nepali men are not active in implementing SRH programs (46).
The findings of this qualitative study highlighted the absence of education, myths, and domination of women as healthcare providers in most clinical settings as the determinants of the lack of men's involvement in SRH programs. Others explained the lack of men's involvement in SRH programs due to the impact of political, economic, and organizational factors. In a study conducted in Uganda, where men's involvement in SRH implementation is still low, the researcher found some barriers in applying policies driving men's participation in SRH programs such as gaps between practice and policy', skills and resources', inadequate key actor participation', and types of dissemination' (47). The health system, in terms of health providers' unfriendly service delivery and socioeconomic and cultural issues, are also highlighted as the influencing factors in the level of men's participation in mother-to-child transmission of HIV (48), as an important part of SRH programs. In line with others, we also emphasized on having more studies and research-based investments in men as agents of change (49) or high impact on SRH promotion.
5. Conclusion
The profound novelty effect of this review is a combination of the existing data with new knowledge, which is needed to fill the knowledge gap, particularly in male-dominant societies. Ideas from different fields of research in SRH and marital satisfaction enrichment targeting men can lead to completely novel discoveries with potential applications of the relevant program implementation. Translational applications of sexology to psychology will raise enormous advances in the diagnosis and management of numerous problems among couples.
Most reports originate from developed societies, and fewer studies are conducted on men in developing countries. There are some explanations for the limited male-focused research-based pieces of evidence. Our findings reveal the necessity of gender-specific studies in the future and implementing interventions and programs focusing on men's participation in conservative and male-dominated societies.
Conflict of Interest
The authors do not mention any conflict of interest in this article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Martin CE Parlier-Ahmad AB Beck L Jain V Terplan M A comparison of sex-specific reproductive and sexual health needs between addiction medicine and primary care treatment settings Subst Use Misuse 202257122912363560776110.1080/10826084.2022.2076873 PMC 9553303 · doi ↗ · pubmed ↗
- 2Klaman SL Lorvick J Jones HE Provision of and barriers to integrating reproductive and sexual health services for reproductive-age women in opioid treatment programs J Addict Med 2019134224293168925910.1097/ADM.0000000000000519 · doi ↗ · pubmed ↗
- 3Buzi RS Smith PB Access to sexual and reproductive health care services: Young men's perspectives J Sex Marital Ther 2014401491572381953010.1080/0092623 X.2012.736923 · doi ↗ · pubmed ↗
- 4World Health Organization Medical eligibility criteria for contraceptive use Switzerland World Health Organization 2010
- 5Sen G Ostin P Unequal, unfair, ineffective and inefficient gender inequity in health: Why it exists and how we can change it Sweden Karolinska Institute 2007
- 6Newcomb ME Romantic relationships and sexual minority health: A review and description of the Dyadic health model Clin Psychol Rev 2020821019243300279510.1016/j.cpr.2020.101924 PMC 10472923 · doi ↗ · pubmed ↗
- 7Alqashan H Enrichment training program and successful marriage in Kuwait: A field study on Kuwaiti couples Digest Middle East Stud 200817116
- 8Carvalho SA Castilho P Seabra D Salvador C Rijo D Carona C Critical issues in cognitive behavioural therapy (CBT) with gender and sexual minorities (GS Ms)Thwaites R The cognitive behaviour therapist UK Cambridge University Press 2022