Endoscopic submucosal dissection for esophageal cancer behind a tracheoesophageal voice prosthesis
Yasuhiro Tani, Koji Higashino, Takashi Kanesaka, Kengo Aoki, Takashi Fujii, Tomoki Michida, Ryu Ishihara

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
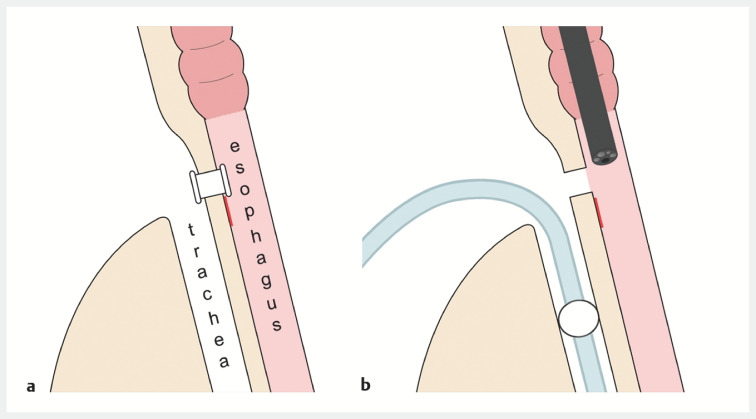 Fig. 1
Fig. 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVoice and Speech Disorders · Dysphagia Assessment and Management · Tracheal and airway disorders
A tracheoesophageal voice prosthesis is used to restore vocal communication after a total laryngectomy 1 2 . This device may interfere with the endoscope during endoscopic treatment of an esophageal lesion. However, its removal poses a risk of aspiration because it is located in a tracheoesophageal fistula. We successfully performed endoscopic submucosal dissection (ESD) for superficial esophageal squamous cell carcinoma behind a tracheoesophageal voice prosthesis.
A 65-year-old man was diagnosed, by means of upper gastrointestinal endoscopy, as having a superficial lesion on his upper thoracic esophagus. The oral part of the lesion was behind a tracheoesophageal voice prosthesis, which was placed after total laryngectomy and jejunal interposition for hypopharyngeal cancer. ESD was planned to be performed under general anesthesia to reduce the risk of aspiration when the tracheoesophageal voice prosthesis was removed.
The patient underwent tracheal intubation, and the intubation balloon was placed caudally to the lesion to prevent aspiration ( Fig. 1 ). After the voice prosthesis was removed, the endoscope was inserted, and markings were made around the lesion ( Video 1 ). ESD was performed using a FlushKnife BT-S (1.5 mm, DK2620J; Fujifilm Medical, Tokyo, Japan) and the lesion was resected en bloc. After replacement of the voice prosthesis, extubation was performed. Histopathological examination revealed squamous cell carcinoma confined to the epithelium. As the lesion was completely removed endoscopically, the patient was followed up without additional treatment. After 8 months, no local recurrence was detected on surveillance endoscopy.
Schematic diagrams. a The oral part of the superficial esophageal lesion behind a voice prosthesis. b The intubation balloon was placed caudally to the lesion and the voice prosthesis was removed.
Endoscopic submucosal dissection for a superficial esophageal lesion, the oral side of which was behind a tracheoesophageal voice prosthesis.Video 1
ESD was successfully performed without any adverse events under general anesthesia by adjusting the cuff position of the intubation tube.
Endoscopy_UCTN_Code_TTT_1AO_2AG
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Terada T Saeki N Toh K Voice rehabilitation with Provox 2 voice prosthesis following total laryngectomy for laryngeal and hypopharyngeal carcinoma Auris Nasus Larynx 200734657117137738 10.1016/j.anl.2006.09.017 · doi ↗ · pubmed ↗
- 2Apert V Carsuzaa F Tonnerre D Speech restoration with tracheoesophageal prosthesis after total laryngectomy: an observational study of vocal results, complications and quality of life Eur Ann Otorhinolaryngol Head Neck Dis 2022139737634140266 10.1016/j.anorl.2021.05.008 · doi ↗ · pubmed ↗