Endoscopic ultrasound-guided choledochoduodenostomy using a novel, ultra-stiff, high-sliding guidewire and a dumbbell-shaped metal stent
Tadahisa Inoue, Mayu Ibusuki, Rena Kitano, Kiyoaki Ito

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
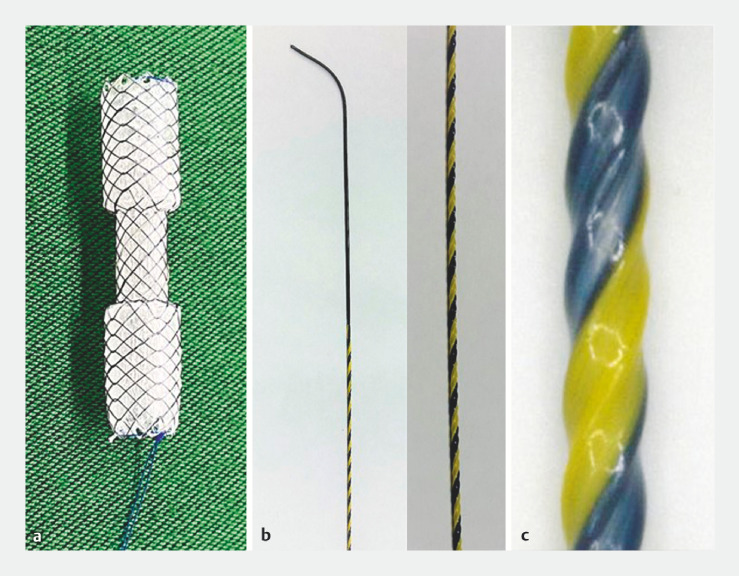 Fig. 1
Fig. 1 Fig. 2
Fig. 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSocial Sciences and Policies
Endoscopic ultrasound-guided choledochoduodenostomy (EUS-CDS) has potential as a first-line drainage method for malignant distal biliary obstruction. Several randomized controlled trials revealed that EUS-CDS with lumen-apposing metal stent (LAMS) have higher technical success rates and shorter procedure times than conventional transpapillary drainage 1 2 . However, thin 6-mm diameter LAMSs are frequently used due to their larger flanges, and these stents are associated with adverse events such as biliary wall compression and duodenobiliary reflux, as well as being expensive 3 . Conversely, EUS-CDS using conventional metal stents is associated with a risk of bile leakage due to the need for fistula dilation, as well as stent migration. Herein, we report a new EUS-CDS technique using a novel, ultra-stiff, high-sliding guidewire and a dumbbell-shaped metal stent.
The dumbbell-shaped metal stent (BONASTENT M-Intraductal; Standard Sci-Tech Inc., Seoul, Korea) has a diameter of 8 mm at the central portion and 12 mm at the proximal and distal portions 4 , providing antimigration properties. The 0.035-inch novel guidewire (SeekMaster Hard; Piolax Medical Devices, Kanagawa, Japan) consists of a thick (0.7 mm in diameter), high-rigidity, nickel-titanium core wire. The polytetrafluoroethylene-coated surface of the wire with “ridge-processing” reduces the contact area and friction with the metal stent delivery system, while increasing the sliding properties and achieving high device followability and insertability, thereby eliminating the need for fistula dilation ( Fig. 1 ).
The stent and guidewire. a The dumbbell-shaped metal stent (BONASTENT M-Intraductal; Standard Sci-Tech Inc., Seoul, Korea) consists of a diameter of 8 mm in the central portion (15 mm length) and 12 mm in the proximal and distal portions (17.5 mm length, each), providing antimigration properties. b The 0.035-inch novel guidewire (SeekMaster Hard; Piolax Medical Devices, Kanagawa, Japan) consists of a thick (0.7 mm in diameter), high-rigidity, nickel-titanium core wire. c The surface of the wire is coated with polytetrafluoroethylene with “ridge-processing,” which reduces the contact area and friction with the metal stent delivery system, increasing sliding properties, and achieving extremely high device followability and insertability, thereby eliminating the need for fistula dilation.
A 73-year-old man with pancreatic cancer developed obstructive jaundice due to malignant distal biliary obstruction. A linear-array echoendoscope was inserted, and the common bile duct was punctured from the duodenum using a 19-G needle. The novel guidewire was inserted through the needle and advanced to the intrahepatic bile duct. The dumbbell-shaped metal stent delivery system was inserted over the guidewire without fistula dilation; the metal stent was deployed from the common bile duct to the duodenum ( Fig. 2 , Video 1 ). The procedure time was 5 minutes, with no adverse events. The stent was patent until the patient’s death, with no stent dysfunction including migration.
Fluoroscopic views. a A linear-array echoendoscope was inserted, and the common bile duct was punctured from the duodenum using a 19-G needle. b The novel guidewire was inserted through the needle and advanced to the intrahepatic bile duct. c Subsequently, the dumbbell-shaped metal stent delivery system was inserted over the guidewire without fistula dilation. d The metal stent was deployed from the common bile duct to the duodenum.
Endoscopic ultrasound-guided choledochoduodenostomy using the novel, ultra-stiff, high-sliding guidewire and the dumbbell-shaped metal stent.Video 1
This technique overcomes the shortcomings of EUS-CDS with LAMS, while allowing the same ease of application.
Endoscopy_UCTN_Code_TTT_1AS_2AD
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Teoh AYB Napoleon B Kunda REUS-guided choledocho-duodenostomy using lumen apposing stent versus ERCP with covered metallic stents in patients with unresectable malignant distal biliary obstruction: a multicenter randomized controlled trial (DRA-MBO Trial)Gastroenterology 20231654734820037121331 10.1053/j.gastro.2023.04.016 · doi ↗ · pubmed ↗
- 2Chen YI Sahai A Donatelli G Endoscopic ultrasound-guided biliary drainage of first intent with a lumen-apposing metal stent vs endoscopic retrograde cholangiopancreatography in malignant distal biliary obstruction: a multicenter randomized controlled study (ELEMENT Trial)Gastroenterology 202316512491.261E 837549753 10.1053/j.gastro.2023.07.024 · doi ↗ · pubmed ↗
- 3Vanella G Bronswijk M Dell’Anna G Classification, risk factors, and management of lumen apposing metal stent dysfunction during follow-up of endoscopic ultrasound-guided choledochoduodenostomy: multicenter evaluation from the Leuven-Amsterdam-Milan Study Group Dig Endosc 20233537738836177532 10.1111/den.14445 PMC 12136247 · doi ↗ · pubmed ↗
- 4Choi HJ Moon JH Lee YN Evaluation of a newly modified nonflared fully covered metal stent, 12 mm in diameter, for intraductal placement in patients with malignant biliary strictures: a feasibility study Endoscopy 20164862563127110694 10.1055/s-0042-105643 · doi ↗ · pubmed ↗