Waldenström Macroglobulinemia-Associated Peripheral Neuropathy in the Brachial Plexus With Bing-Neel Syndrome Diagnosed Through Repeated Cerebrospinal Tests
Misaki Hatasa, Naoto Imoto, Shota Komori, Yasunobu Nosaki, Shingo Kurahashi

TL;DR
A patient with Waldenström macroglobulinemia developed peripheral neuropathy and Bing-Neel syndrome, which was diagnosed through repeated cerebrospinal fluid tests and successfully treated with tirabrutinib.
Contribution
This case highlights the importance of diagnosing Bing-Neel syndrome in Waldenström macroglobulinemia patients using repeated CSF tests and the effectiveness of tirabrutinib.
Findings
Tirabrutinib effectively treated Waldenström macroglobulinemia-associated peripheral neuropathy with Bing-Neel syndrome.
Bing-Neel syndrome was confirmed through repeated cerebrospinal fluid tests despite initially negative results.
Neurological symptoms subsided after tirabrutinib treatment and remained stable for 25 months.
Abstract
In Waldenström macroglobulinemia (WM), confirming the presence of Bing-Neel syndrome (BNS) is important because drugs that penetrate the central nervous system (CNS) must be selected. We report the case of a 75-year-old man for whom tirabrutinib, a second-generation Bruton’s tyrosine kinase inhibitor (BTKi), was useful in treating WM-associated peripheral neuropathy (PN) with BNS. Numbness and muscle weakness in the fingers occurred three years after the initial treatment of WM. WM-associated PN due to demyelinating disease was diagnosed based on the results of a nerve conduction study and magnetic resonance imaging showing bilateral symmetric swelling of the brachial plexus. The cerebrospinal fluid (CSF) cytology results were initially negative; however, the CSF test was repeated because of extremely high protein levels (984 mg/dL) and slightly elevated leukocyte counts (14/µL). The…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
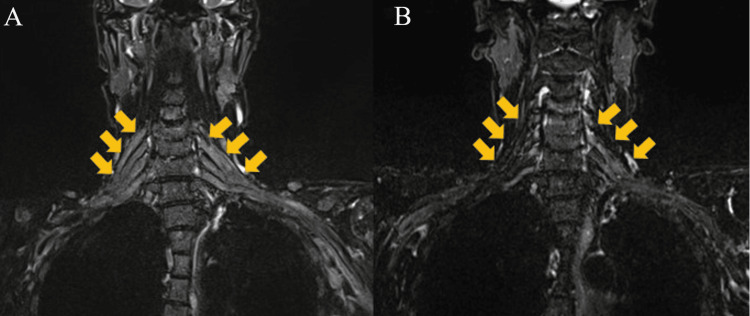 Figure 1
Figure 1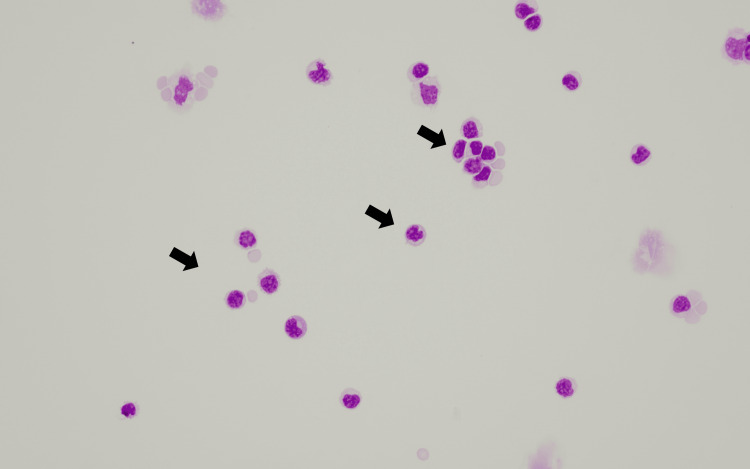 Figure 2
Figure 2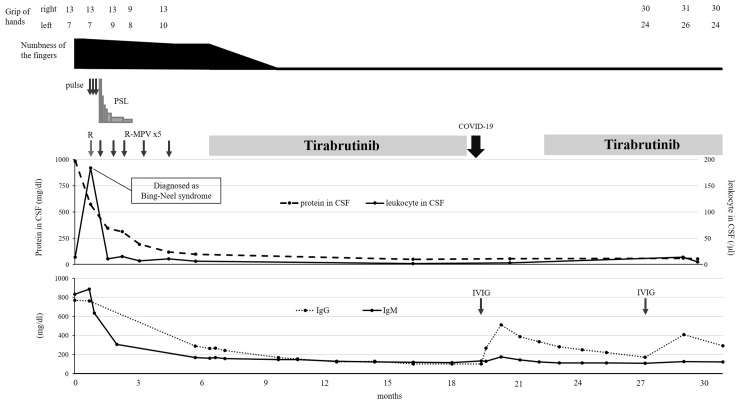 Figure 3
Figure 3| Variable | At diagnosis of peripheral neuropathy | At diagnosis of Bing-Neel syndrome | After two courses of R-MPV | At the completion of R-MPV | 24 months after administration of tirabrutinib | Reference range |
| Complete blood cell count | ||||||
| White blood cell (/μL ) | 5390 | 5470 | 10380 | 6520 | 4770 | 3300–8600 |
| Neutrophil (%) | 56 | 64.7 | 78 | 66.6 | 52.2 | 38.5–80.5 |
| Lymphocyte (%) | 25.4 | 19.2 | 11 | 16.6 | 36.7 | 16.5–49.5 |
| Monocyte (%) | 16.9 | 14.8 | 9 | 14.1 | 9 | 2.0–10.0 |
| Hemoglobin (g/dL) | 11.8 | 10.9 | 10.6 | 12.3 | 13 | 13.7–16.8 |
| Platelet count (×104/μL) | 29 | 26.6 | 22.7 | 15.8 | 14.2 | 15.8–34.8 |
| Blood chemistry | ||||||
| LDH (U/L) | 130 | 123 | 130 | 158 | 149 | 124–222 |
| CRP (mg/dL) | 2.58 | 2.81 | 0.04 | 0.51 | 0.1 | 0–0.14 |
| IgM (mg/dL) | 832 | 885 | 306 | 168 | 120 | 33–183 |
| Cerebrospinal fluid | ||||||
| Red blood cell (×104/μL) | 0.01 | 0.01 | 0 | 0.02 | 0.01 | - |
| Leukocytes (/μL) | 14 | 184 | 15 | 6 | 5 | - |
| Mononuclear cells (/μL) | 14 | 183 | 15 | 5 | 5 | - |
| Unclassifiable cells (/μL) | 1 | 6 | 1 | 0 | 1 | - |
| Protein (mg/dL) | 984 | 572 | 312 | 98 | 54 | - |
| Glucose (mg/dL) | 38 | 88 | 63 | 45 | 50 | - |
| IgM (mg/dL) | 58.9 | N/A | 12.8 | 1 | 0.2 | - |
| M protein (IFE) | N/A | IgM-κ M protein | N/A | N/A | N/A* | - |
| Cytology | negative | Plasma-cell-like lymphocytes positive | Negative | Negative | Negative | - |
| Reference | Age at tirabrutinib administration (years)/sex | WM-related therapy before BNS diagnosis | Lesion at tirabrutinib administration | BNS therapy | Response of tirabrutinib | AEs of tirabrutinib | EFS months (from tirabrutinib administration) | Discontinuation of tirabrutinib |
| Yokoyama et al. [ | 46M | Cyclosporin, PSL, steroid pulse (treated as membranous nephropathy and inflammatory demyelinating disease | CSF, periventricular, full spine, bone marrow, kidney | Steroid pulse+ PSL → BR+ IT → [PD] → steroid pulse+ PSL → tirabrubinib | PR | (–) | 15 months (no relapse) | (–) |
| Hagihara et al. [ | 62F | Rituximab monotherapy | CSF, Th2-6 thoracic spinal cord, left iliopsoas, and bilateral femurs | HDMTX → R-MPV → [SD] → HDAC → [remission] → relapse as BNS after 1.5 years→ HDAC → [SD] → BR → [remission] → relapse as BNS after 3 months → tirabrutinib | PR or CR | Herpes zoster (grade unclear) | 12 months (no relapse) | (–) |
| Oyama et al. [ | 62M | R-CHOP, BR | Leptomeninges and cauda equina roots, bone marrow, axillary lymph node | Tirabrubinib | PR or CR | (–) | 3 months (no relapse) | (–) |
| Saburi et al. [ | 66F | R-COP, R-CHOP | C2-4 cervical spinal cord, Th2-3 thoracic spinal cord | Tirabrubinib | CR | Pruritus (grade1) | 10 months (no relapse) | (–) |
| Saburi et al. [ | 73M | R-CHOP, BR | Medulla, bilateral basal ganglia | R-MPV → [PD] → craniospinal irradiation (30.6 Gy) → progression to BNS after 2 years → tirabrutinib | CR | (–) | 3 months (no relapse) | (–) |
| Hatasa et al. (current report) | 75M | DRC, BD | Brachial plexus and nerve roots at C4-Th1 (cytology of CSF become negative before start of tirabrutinib) | Rituximab + steroid pulse, R-MPV → tirabrutinib | PR | Eczema (grade 1), decreased IgG level | 25 months (no relapse) | Transient discontinuation due to COVID-19 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Lymphocytic Leukemia Research · CNS Lymphoma Diagnosis and Treatment · Peripheral Neuropathies and Disorders
Introduction
Peripheral neuropathy (PN) occurs in approximately 20% of patients with Waldenström macroglobulinemia (WM) at diagnosis and in up to 50% of patients at some point during the progression of the disease [1]. In contrast, Bing-Neel syndrome (BNS) is a rare form of WM with lymphoplasmacytic infiltration of the central nervous system (CNS), accounting for approximately 1% of all WM cases [2,3].
Despite several treatment options available for WM-associated PN, there is no trial data specifically assessing the efficacy of these options [1]. Although ibrutinib has been reported to be effective against WM-associated PN [4,5], the efficacy of second-generation Bruton’s tyrosine kinase inhibitors (BTKi) in WM-associated PN remains unclear. Determining the occurrence of BNS is important for treatment selection because BNS is treated with drugs that need to penetrate the CNS. Case reports have suggested that tirabrutinib is effective against BNS [6-10].
Herein, we report a patient diagnosed with WM-associated PN who also presented with BNS based on several modalities, including repeated cerebrospinal fluid (CSF) tests. Following rituximab, high-dose methotrexate, procarbazine, and vincristine (R-MPV) therapy, the patient's symptoms were resolved with tirabrutinib treatment. We also reviewed five previously reported cases of BNS treated with tirabrutinib [6-10].
Case presentation
A 75-year-old man developed numbness and muscle weakness in the fingertips of both hands during follow-up after treatment for WM. Four years ago, he was diagnosed with WM owing to high serum levels of immunoglobulin (Ig) M and IgM-κ type M-protein and increased numbers of MYD88 L265P mutation-positive plasma cell-like lymphocytes in the bone marrow. Therapy with dexamethasone, rituximab, and cyclophosphamide was initiated due to progressed pleural effusion, but no treatment response was observed. Bortezomib was subsequently administered, and a complete response was achieved.
His neurological symptoms gradually worsened over a period of three months, at which point we started the assessment. Physical examination revealed intrinsic muscle atrophy in both hands and decreased deep tendon reflexes in the upper extremities. The hand grip was also reduced in both hands (right, 13 kg; left, 7 kg). A nerve conduction study revealed proximal conduction velocity delay and conduction block in the median and ulnar nerves, suggesting extensive demyelinating disease. CSF tests showed increased levels of CSF protein (984 mg/dL), slightly increased leukocyte count (14/µL), unclassifiable cells (1/µL), and increased immunoglobulin levels (IgG: 70.3 mg/dL, IgM: 58.9 mg/dL); however, cytology was negative. The presence of anti-myelin-associated glycoprotein (anti-MAG) antibodies was not tested because this examination is not covered by health insurance in Japan.
In Figure 1, magnetic resonance imaging (MRI) revealed diffuse bilateral symmetric swelling of the nerve root to the brachial plexus at the C4-Th1 level (Figure 1A) with normal brain, cervical, and thoracic spines. Although these findings were consistent with inflammatory demyelinating disease, we considered that the slightly elevated numbers of leukocytes and extremely high levels of the CSF protein were not indicative of immune-mediated neuropathy. A repeat CSF test three weeks after the first test revealed the presence of the IgM-κ type M protein and an increase in the number of abnormal lymphoplasmacytic cells (189/µL) (Figure 2).
T2-weighted coronal magnetic resonance imaging (MRI) of the cervical area after diagnosis of Waldenström macroglobulinemia (MW)-associated peripheral neuropathy (PN)Yellow arrows indicate the brachial plexus. (A) Before treatment for PN and (B) 15 months after treatment with tirabrutinib.
Cerebrospinal fluid (CSF) image at the diagnosis of Bing-Neel syndrome (BNS) (Giemsa staining, ×400)
However, the red blood cell counts and sugar levels were normal. In addition, the levels of serum IgM (885 mg/dL, reference range: 33-183 mg/dL) and C-reactive protein (2.81 mg/dL, reference range: 0.0-0.14 mg/dL) were also increased. Table 1 shows the most relevant test results for each phase after the diagnosis of WM-associated PN.
Neither a CSF MYD88 mutation test nor flow cytometry (FCM) were performed. The patient was diagnosed with WM-associated PN accompanied by BNS.
Four months after symptom onset, the patient was administered steroid pulse therapy (methylprednisolone 1000 mg/d for three days) and rituximab (375 mg/m2) to treat BNS complicated by inflammatory demyelinating disease, followed by R-MPV (day 1, rituximab, 375 mg/m2; day 2, methotrexate, 3.5 g/m2; and vincristine, 1.4 mg/m2; days 2-8; and procarbazine, 100 mg/m2 per day, administered during odd cycles). After two courses, the neurological symptoms of the patient were slightly improved, although the MRI revealed no improvement in brachial plexus swelling. However, a repeat CSF test showed a decrease in the levels of CSF protein and cell counts (protein, 312 mg/dL; leukocytes, 15/µL), suggesting a treatment response, and thus R-MPV therapy was continued. Evaluation of the treatment response after completion of the fifth course showed negative CSF cytology results and improved biochemical data (protein, 98 mg/dL; leukocytes, 6/µL; and serum IgM levels, 168 mg/dL). As the peripheral nerve symptoms persisted, tirabrutinib therapy (480 mg/d) was initiated. The patient showed improvement in his symptoms one week after starting tirabrutinib treatment. However, he developed grade 1 eczema two weeks after the initiation of tirabrutinib therapy, which was resolved after treatment with a steroid ointment. Before starting tirabrutinib, the patient had difficulty with movements requiring dexterity and muscle strength, such as buttoning, using chopsticks, and wringing towels. However, the patient was able to perform these activities normally for several months after the administration of tirabrutinib. Tirabrutinib was administered for 12 months but was discontinued when the patient developed a COVID-19 infection. The levels of serum IgG in the patient were gradually decreased to <100 mg/dL after treatment initiation. To prevent the worsening of the COVID-19 infection, an immunoglobulin preparation was administered. Tirabrutinib treatment was subsequently resumed. Re-evaluation before the resumption of tirabrutinib treatment (15 months after the initial treatment with tirabrutinib) confirmed a reduction in the pretreatment swelling of the nerve root and brachial plexus (Figure 1B). The patient was followed up for 25 months from the start of tirabrutinib therapy, exhibiting improved hand grip and no deterioration of neurological symptoms compared with before treatment (right: 13 kg → 30 kg, left: 10 kg → 24 kg). The clinical course of the patient is shown in Figure 3.
Clinical course of the patient after the diagnosis of Bing-Neel syndrome (BNS)CSF: cerebrospinal fluid; Ig: immunoglobulin; IVIG: intravenous immunoglobulin; PSL: prednisolone; R: rituximab; R-MPV: rituximab-methotrexate-procarbazine-vincristine; WBC: white blood cell
Discussion
In the present case, we diagnosed coexisting WM-associated PN and BNS, despite the initial negative results for BNS. The patient had motor and sensory dysfunction of the upper extremities with symmetric symptoms mainly localized to the fingertips, which are typical PN symptoms. Diffuse bilateral symmetric swelling of the nerve root to the brachial plexus, with a normal brain and cervical and thoracic spine on MRI, was also consistent with PN [1]. Thus, we assumed that these symptoms were due to WM-associated PN, with the patient being asymptomatic for BNS. To the best of our knowledge, the present case may represent the first report of repeated CSF tests revealing WM-associated PN accompanied by BNS.
Various factors might cause WM-associated PN, including anti-MAG antibodies, rare autoantibodies, neurotoxicity due to direct tumor infiltration, amyloidosis caused by WM, cryoglobulinemia, vasculitis, and chemotherapy [11]. Unfortunately, we were restricted by regulations in the measurement of anti-MAG and other antibodies related to PN due to the insurance system in Japan. We assumed that the immune-mediated mechanism was mainly attributed to diffuse, symmetric, and demyelinating patterns [1]. However, nerve root swelling and BNS suggested the possibility of direct infiltration of tumor cells into the nerves, which subsequently extended into the CSF.
The incidence of BNS could be underestimated because WM-associated PN is common, whereas the clinical symptoms of BNS are variable [2,3]. To prevent underestimation, it is important to consider atypical findings of WM-associated PN. Asymmetrical distribution, predominant motor dysfunction, balance disorders, gait abnormalities, cognitive impairment, and cranial nerve deficits are signs of suspected BNS [12]. As for the laboratory findings, inflammatory demyelinating disease is characterized by normal leukocyte counts of <10 mm2 [13], which in our case were slightly higher at 14/µL. In addition, inflammatory demyelinating disease is generally characterized by elevated levels of the CSF protein; however, a level of approximately 1000 mg/dL is not typical [14]. The difference in the value between the first and second CSF tests may be attributed to disease progression or a false negative in the first CSF. False-negative CSF cytology results are common, especially with small volumes (<10.5 mL) or a limited number of tests (<2) [15].
Once a diagnosis of BNS is suspected, it is recommended to have brain and entire spine MRI scans with gadolinium (Gd) administration. The MRI protocol should include fluid-attenuated inversion recovery and T1-weighted sequences before and after Gd injection. Lumbar puncture should be performed after MRI evaluation to avoid obstructive hydrocephalus and non-specific enhancement. The standard diagnosis of BNS is the demonstration of WM cells in the CSF, or less frequently, on brain tissue biopsy. FCM tests of the CSF, which are characterized by positive expression of CD19, CD20, CD22, CD79a, CD27, and CD52 and usually negative expression of CD5, CD10, and CD23, along with tests for immunoglobulin heavy chain gene rearrangement and MYD88 L265P gene mutation, are all important in supporting the diagnosis of BNS [12].
The diagnosis of BNS in our patient was limited to CSF cytology findings only, whereas FCM and genetic testing of CSF, which are required for diagnosing BNS [12], were not performed. However, considering the presence of lymphoplasmacytic cells in the CSF, the normal red blood cell count in the CSF, and the lack of WM cells in the peripheral blood at that time, a diagnosis of BNS would be appropriate [3]. Our case demonstrated that a careful evaluation of progression or coexistence with BNS is important when lesions are close to the CNS in PN or when the initial CSF findings are atypical in patients with WM-associated PN.
The goal of the treatment in BNS should be to reverse the patient’s clinical symptoms and prolong progression-free survival. However, it is unclear whether asymptomatic patients with BNS should receive treatment. The standard treatment for BNS has not been established, and several options, including high-dose methotrexate, high-dose cytarabine, bendamustine, cladribine, fludarabine, and ibrutinib, are present [12]. Some experts recommend reserving a high-dose regimen until relapse owing to its toxicity and setting ibrutinib in a frontline setting [12]. The treatment effect of BTKi for BNS has been previously reported with ibrutinib [2]. However, other studies reported the occurrence of some adverse events (AEs), such as atrial fibrillation and hemorrhagic events [4]. Tirabrutinib is a second-generation BTKi with a low affinity for kinases other than BTK that was designed to improve the efficacy and reduce the toxicity of BTKi [16]. Tirabrutinib was well tolerated in patients, with the most frequent AE being exanthema of grade 2 or lower, whereas no arrhythmia was observed [17]. Furthermore, preclinical data showed that among second-generation BTKi, tirabrutinib was transferred to the CNS more favorably than zanubrutinib [18], suggesting that tirabrutinib is a potent option for patients with central nervous lesions. This drug was first approved in Japan for the treatment of primary central system lymphoma [19] in 2020 worldwide, followed by its approval for use against WM [17].
In this case, preventing the relapse of BNS was possible due to the poor age-related prognosis and treatment for WM prior to BNS diagnosis [20]. A search for "Bing-Neel syndrome" and "tirabrutinib" in PubMed on December 3, 2023, identified five studies on tirabrutinib for treating BNS (Table 2) [6-10].
Tirabrutinib demonstrated therapeutic effects in all cases, despite variations in BNS lesions. None of the patients experienced relapse during the follow-up period after the start of tirabrutinib treatment (median, 11 months; range, 3-25 months), suggesting persisting effects. Of the five reported patients, three had BNS refractory to chemotherapy prior to tirabrutinib treatment. One patient responded to bendamustine-rituximab but relapsed at three months, and subsequent tirabrutinib treatment exhibited a response lasting >12 months. These results suggested that tirabrutinib is effective even in patients who are resistant to other regimens, further suggesting that the duration of response may be longer than that for other therapies. Moreover, no tirabrutinib-associated AEs or only grade 1 AEs were recorded. Overall, these results suggest that tirabrutinib may be a promising treatment option for patients with BNS. Further comprehensive studies are needed to confirm the efficacy of tirabrutinib for the treatment of BNS.
Our case had some limitations in terms of diagnosis. We did not confirm the detailed etiology of PN because of the lack of anti-MAG antibodies or rarer autoantibodies. These tests are crucial for selecting the appropriate treatment for WM-related PN [1]. Therefore, they should be performed, regardless of whether they are covered by insurance. For the diagnosis of BNS, an MRI was performed only for the brain and cervical spine and not for the full spine. CSF tests based solely on cytological evaluation should be discouraged, and FCM and molecular tests should be evaluated. Because situations where BNS is suspected are rare, the diagnostic algorithm should be kept in mind in advance.
Finally, it is worth reconsidering the suitability of steroid pulse therapy and five courses of R-MPV for the current patient. Importantly, R-MPV contains vincristine, which is a neurotoxic agent, whereas corticosteroids have little or no effect on WM-associated PN [1]. We believe that it is reasonable to select a regimen with good CNS penetration for BNS; however, the main complaint in our patient was WM-associated PN. For BNS only, the goal of treatment is to clear the symptoms of the patient, while for asymptomatic BNS only observation is recommended [3]. Therefore, to provide symptom-oriented therapy rather than targeting the CSF findings, we should have considered changing the treatment in light of the "refractory" evaluation after two courses of R-MPV based on the lack of improvement in symptoms and MRI findings rather than the evaluation of "response" based on CSF findings.
Conclusions
The possibility of concurrent BNS should be carefully investigated in patients with WM-associated PN. Repeated evaluations should be performed when lesions are close to the CNS or when the initial CSF findings are atypical, such as extremely high protein levels or slightly high leukocyte counts in patients with WM. Tirabrutinib may be the preferred treatment for WM-associated PN accompanied by BNS.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Investigation and management of Ig M and Waldenström-associated peripheral neuropathies: recommendations from the IWWM-8 consensus panel Br J Haematol D'Sa S Kersten MJ Castillo JJ 72874217620172819899910.1111/bjh.14492 · doi ↗ · pubmed ↗
- 2Ibrutinib for the treatment of Bing-Neel syndrome: a multicenter study Blood Castillo JJ Itchaki G Paludo J 29930513320193052311910.1182/blood-2018-10-879593 · doi ↗ · pubmed ↗
- 3Guideline for the diagnosis, treatment and response criteria for Bing-Neel syndrome Haematologica Minnema MC Kimby E D'Sa S 435110220172775881710.3324/haematol.2016.147728 PMC 5210231 · doi ↗ · pubmed ↗
- 4Ibrutinib in previously treated Waldenström's macroglobulinemia N Engl J Med Treon SP Tripsas CK Meid K 1430144037220152585374710.1056/NEJ Moa 1501548 · doi ↗ · pubmed ↗
- 5Mutational profile in 75 patients with anti-myelin-associated glycoprotein neuropathy: clinical and hematologic therapy response and hints on new therapeutic targets Neurol Neuroimmunol Neuroinflamm Castellani F Visentin A Schirinzi E 010202310.1212/NXI.0000000000200122 PMC 1015577837137530 · doi ↗ · pubmed ↗
- 6Bing-Neel syndrome successfully treated with tirabrutinib (Article in Japanese)Rinsho Ketsueki Yokoyama K Ohigashi H Miyajima T 8708756320223605885710.11406/rinketsu.63.870 · doi ↗ · pubmed ↗
- 7Complete response with tirabrutinib for relapsed and refractory Bing-Neel syndrome (Article in Japanese)Rinsho Ketsueki Hagihara M Ide S Ohara S Imai Y Uchida T Inoue M 7707756320223592294610.11406/rinketsu.63.770 · doi ↗ · pubmed ↗
- 8Bing-Neel syndrome successfully treated with tirabrutinib Intern Med Oyama T Taoka K Chiba A Matsuda K Maki H Masamoto Y Kurokawa M 357535796120223556998910.2169/internalmedicine.9545-22PMC 9790791 · doi ↗ · pubmed ↗