Puzzling Papillomas: A Case of an Intraductal Papilloma Mimicking an Abscess
Siya Patil, Christine Chen

TL;DR
A patient was initially treated for a breast abscess but later found to have a benign tumor called an intraductal papilloma, highlighting the need for careful follow-up and imaging.
Contribution
This case highlights the diagnostic challenge of intraductal papillomas mimicking abscesses and emphasizes the importance of follow-up.
Findings
The patient was initially misdiagnosed with an abscess due to similar symptoms.
A year later, imaging revealed an intraductal papilloma instead of an abscess.
The case emphasizes the need for atypical imaging and close monitoring of breast lesions.
Abstract
Intraductal papillomas (IDPs) are benign tumors found within breast ducts. Clinicians should be familiar with IDPs given their association with atypical and neoplastic lesions. In our case, the patient was initially diagnosed with and treated for an abscess given clinical symptoms of breast pain, erythema, and swelling, but upon returning to the clinic a year later due to persistent symptoms, she was found to have an IDP. This case underscores the importance of atypical imaging features and close follow-up when evaluating breast lesions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
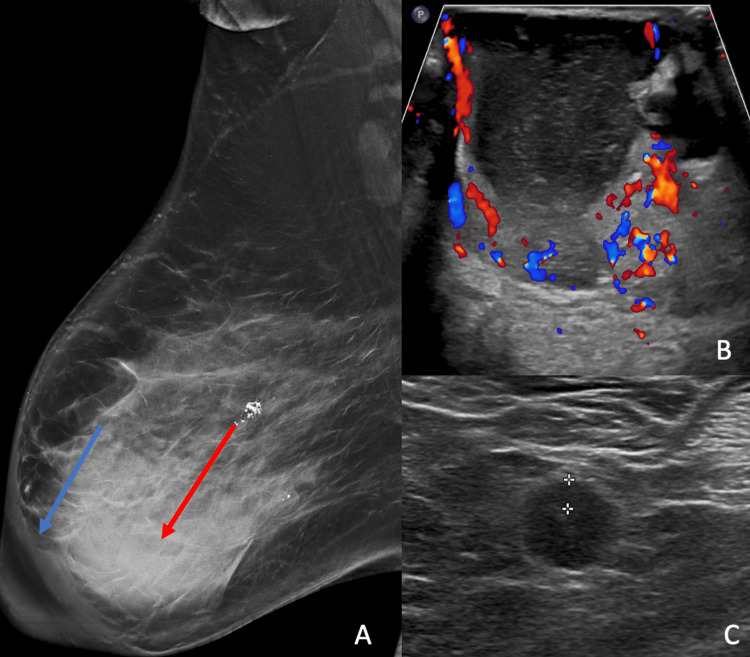 Figure 1
Figure 1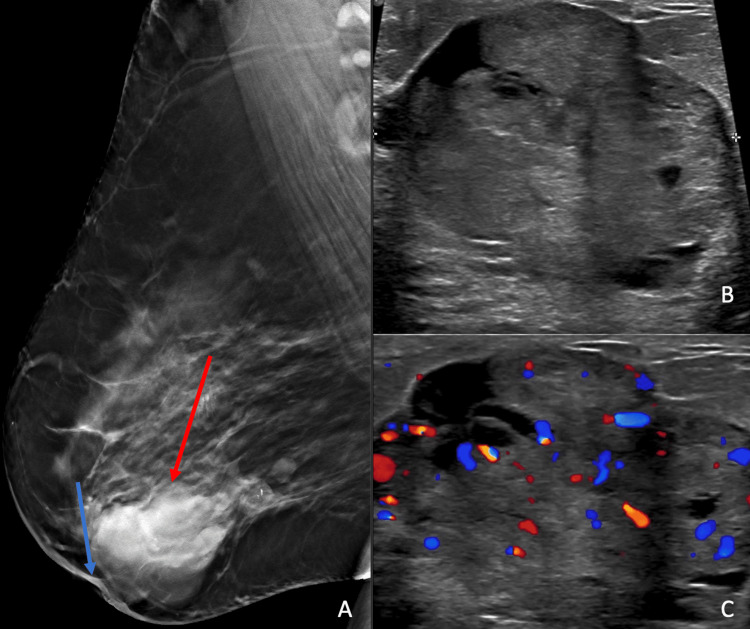 Figure 2
Figure 2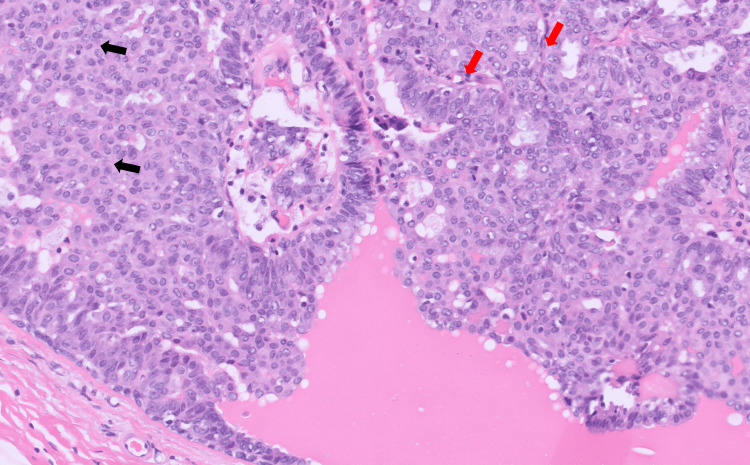 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBreast Lesions and Carcinomas · Cancer and Skin Lesions · Salivary Gland Tumors Diagnosis and Treatment
Introduction
Intraductal breast papillomas are benign tumors that fall within the spectrum of papillary breast lesions [1]. Despite constituting less than 2% of breast lesions [2], they are important as they are high-risk malignancy precursor lesions [3]. Most patients with papillomas are asymptomatic but they can occasionally present with a palpable abnormality and bloody or clear nipple discharge [1]. Timely diagnosis is essential, as upgrade rates to malignant and pre-malignant lesions range from 1.6-20% [3-6]. Our case presents a challenging dilemma of an intraductal papilloma (IDP) initially misdiagnosed as an abscess.
Case presentation
A 57-year-old postmenopausal female presented to the breast surgery clinic with right breast swelling, pain, and bloody nipple discharge for three months. Physical exam revealed diffuse right breast thickening and erythema, but no palpable masses. She was subsequently referred for diagnostic imaging. A diagnostic mammogram revealed a 7.5 cm retroareolar mass with associated skin and trabecular thickening (Figure 1A). The left breast did not reveal any suspicious findings (not shown). On diagnostic ultrasound, there was a hypervascular complex cystic mass with thick, irregular walls measuring 7.5 x 6.8 x 7.1 cm (Figure 1B). A few prominent lymph nodes with concentric cortical thickening were identified in the right axilla (Figure 1C). These findings were suspicious, so the lesion was categorized as BIRADS 4 (Breast Imaging-Reporting and Data System), and an ultrasound-guided core biopsy was recommended.
A: Diagnostic mammogram shows a retroareolar right breast mass (red arrow) and associated skin and trabecular thickening (blue arrow); B: Diagnostic ultrasound revealed a hypervascular, complex cystic mass; C: Prominent lymph nodes with concentric cortical thickening, measuring up to 0.4 cm, in the ipsilateral axilla were also found
The patient opted for a skin punch biopsy of the right breast in the surgeon’s office, which yielded inflammatory changes and neutrophils. Given the high clinical suspicion of breast abscess, incision and drainage of the right breast mass was performed, which yielded purulent fluid. The patient was prescribed oral antibiotics with clinical improvement and instructed to follow up in the clinic in three months.
The patient was lost to follow-up and returned a year later with a new palpable mass in the right breast, new nipple retraction, as well as persistent right-sided bloody nipple discharge. A diagnostic mammogram was performed and revealed a mass in the right central inner breast associated with new nipple retraction (Figure 2A). On ultrasound, there was a corresponding 4.0 x 3.5 x 1.3 cm irregular hypoechoic mass with internal vascularity (Figure 2B and Figure 2C).
A: Right breast mammogram a year later shows skin thickening, new nipple retraction (blue arrow), and a mass (red arrow); B and C: Ultrasound of the right breast revealed a corresponding hypervascular, hypoechoic mass
These findings were deemed suspicious and an ultrasound-guided core biopsy was performed, which yielded a benign intraductal papilloma. Given the large size and nipple retraction, as well as the potential risk of under-sampling, surgical excision was advised.
Wire localized excision of the right breast mass was performed with final surgical pathology revealing a benign intraductal papilloma (Figure 3). The patient will be seen annually in the high-risk screening clinic.
This slide shows the intraductal papilloma with usual ductal hyperplasia (black arrows) and fibrovascular cores (red arrows)
Discussion
Our case demonstrates an unusual imaging appearance and clinical presentation of a benign IDP with abscess formation. Intraductal papillomas are benign, high-risk lesions, which can be categorized as solitary versus multiple intraductal papillomas. Solitary IDPs, as in our case, are located in the retroareolar region and may present with clear or bloody nipple discharge [1,5]. Multiple intraductal papillomas are less common, tend to arise from the terminal ductal lobular unit, and may present as a palpable abnormality [7]. Furthermore, there is an increased risk of coexisting atypical and neoplastic lesions with multiple IDPs, compared with solitary IDPs [7].
On mammography, IDPs may be imaging-occult given dense breast tissue in the retroareolar region [7]. When mammographically evident, IDPs usually present as round or oval masses with circumscribed margins, or less commonly as grouped benign-appearing calcifications [4,5,7]. On ultrasound, IDPs appear as an intraductal mass and may have an associated feeding vessel [7]. On MRI, smaller lesions may be occult while larger IDPs can appear as enhancing masses with variable intraductal components [5,7]. The lesions may enhance irregularly or uniformly and can have washout or plateau kinetics [7]. Finally, on galactography, IDPs appear as mural-based filling defects with smooth or lobulated margins [7]. In terms of management, IDPs are generally surgically excised because they are high-risk precursor lesions [1]. Upgrade rates to malignancy range from 1.6% to 20% [3-6] depending on the presence of atypia. Alternatively, if surgery is not desired, radiologic follow-up may be an appropriate method of surveillance for select cases of IDPs that are small (less than 1.0 cm) and without atypia [8].
To our knowledge, no other examples of an IDP with inflammatory characteristics exist in the literature. The case was challenging as the patient initially presented with symptoms of infection and histopathology from the initial skin punch biopsy confirmed infectious etiology. Furthermore, incision and drainage revealed yellow purulent fluid and the patient clinically improved after a course of oral antibiotics. It is possible that the large size of the mass led to duct obstruction and superimposed infection of the IDP. Unfortunately, the patient was lost to follow-up for one year and the diagnosis of IDP was made via core biopsy more than one year after initial presentation. This case demonstrates the importance of close clinical follow-up for patients suspected of breast abscess while illustrating a highly unusual imaging appearance of an IDP as a retroareolar mass associated with skin thickening and nipple retraction.
Conclusions
IDPs are benign entities with a wide spectrum of imaging appearances. Biopsy should be performed for most cases given the variable imaging appearance and characterization as high-risk precursor lesions. Finally, if a patient is diagnosed with a breast abscess, follow-up imaging to resolution can be beneficial.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Intraductal papilloma 9 2023 Li A Kirk L Treasure Island (FL)Stat Pearls 2022 https://www.ncbi.nlm.nih.gov/books/NBK 519539/
- 2Unusual recurrent metastasizing benign breast papilloma: a case report J Med Case Rep Jain AL Mullins J Smith JR 33142020 https://doi.org/10.1186/s 13256-020-2354-73207043510.1186/s 13256-020-2354-7PMC 7029571 · doi ↗ · pubmed ↗
- 3Audit on intraductal papilloma of the breast: upgrade rate, management pitfalls, and updated guidelines in a tertiary health care center Cureus Esmayil H Abayazeed S Hajaj M 013202110.7759/cureus.18763 PMC 859008634796058 · doi ↗ · pubmed ↗
- 4A case of giant complicated intraductal papilloma of breast on MRI and literature review Cancer Rep (Hoboken) Wang S Lou J 01201810.1002/cnr 2.1136 PMC 794158432729233 · doi ↗ · pubmed ↗
- 5Radiological appearances of papillary breast lesions Clin Radiol Brookes MJ Bourke AG 126512736320081892904410.1016/j.crad.2008.02.012 · doi ↗ · pubmed ↗
- 6Upgrade rate of intraductal papilloma without atypia on breast core needle biopsy: a clinical, radiological and pathological correlation study Am J Surg Genco IS Tugertimur B Manolas PA Hasanovic A Hajiyeva S 67768122020203200723610.1016/j.amjsurg.2020.01.040 · doi ↗ · pubmed ↗
- 7Papillary lesions of the breast: MRI, ultrasound, and mammographic appearances AJR Am J Roentgenol Eiada R Chong J Kulkarni S Goldberg F Muradali D 26427119820122226816710.2214/AJR.11.7922 · doi ↗ · pubmed ↗
- 8Intraductal papilloma on breast biopsy: upstaging rate and implications for practice guidelines Am Surg Jee Y Bakht A Burner JM Coldren DL Howard-Mc Natt M Chiba A 146714708820223542050610.1177/00031348221082276 · doi ↗ · pubmed ↗