Bleeding From a Ruptured, Extraluminally Growing Gastric Gastrointestinal Stromal Tumor Treated by Transcatheter Arterial Embolization: A Case Report
Hiroshi Okano, Atsuhiro Nakatsuka, Masaomi Ogura, Katsumi Mukai, Akira Nishimura, Kana Asakawa, Youichirou Baba, Tetsuya Murata, Seiichi Hirota

TL;DR
A man with a ruptured stomach tumor was successfully treated with a procedure to stop internal bleeding before surgery.
Contribution
Highlights the use of transcatheter arterial embolization for rare cases of ruptured extraluminally growing gastric tumors.
Findings
Transcatheter arterial embolization effectively stopped intra-abdominal bleeding from a ruptured tumor.
The tumor was later surgically removed and diagnosed as a gastric gastrointestinal stromal tumor.
TAE is a viable emergency treatment for such rare cases before definitive surgery.
Abstract
A 49-year-old man with abdominal pain was referred to our hospital. Abdominal computed tomography showed an extraluminal tumor near the gastric anterior wall and intra-abdominal fluid collection. A ruptured intra-abdominal tumor was suspected, and emergency abdominal angiography was performed. Hemorrhage into the abdominal cavity was seen, and transcatheter arterial embolization (TAE) was performed, which stopped the bleeding. The tumor was surgically resected, and a diagnosis of an extraluminally growing gastric gastrointestinal stromal tumor was made. TAE should be considered for rare cases of extraluminally growing tumors with intra-abdominal hemorrhage.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1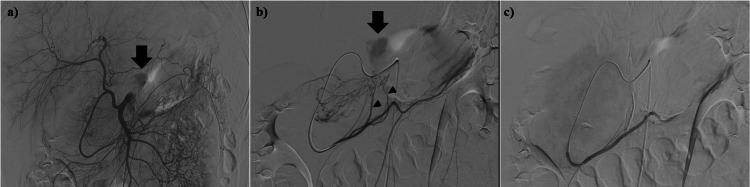 Figure 2
Figure 2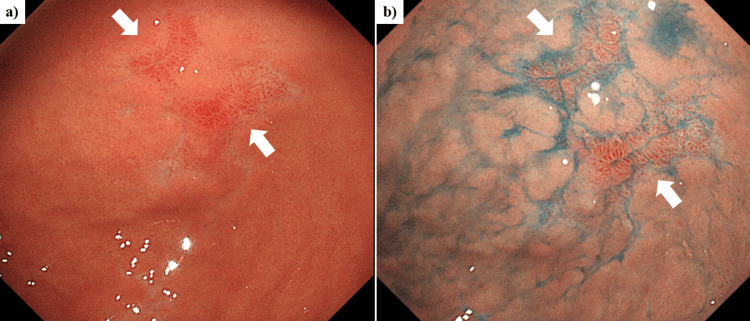 Figure 3
Figure 3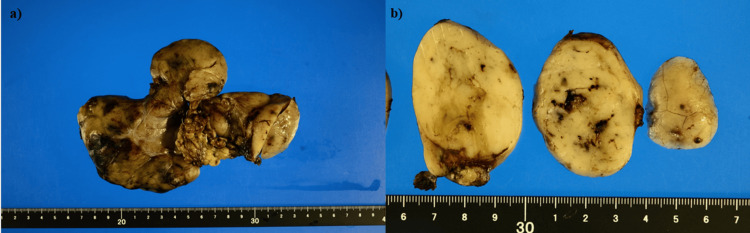 Figure 4
Figure 4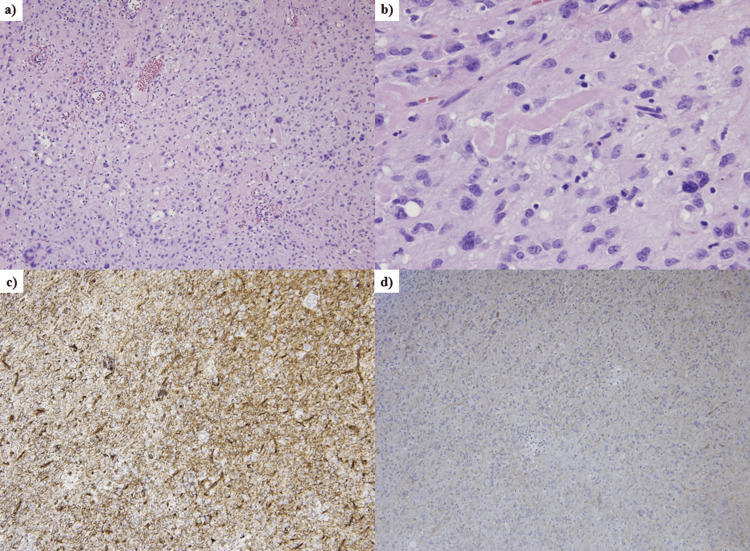 Figure 5
Figure 5| Reference range | On admission | |
| CBC | ||
| WBC (/mL) | 3900-9800 | 7400 |
| RBC (/mL) | 427-570 | 387 × 104 |
| Hemoglobin (g/dL) | 13.5-17.6 | 12.3 |
| Hematocrit (%) | 39.8-51.8 | 35.4 |
| Platelets (/mL) | 130-369 | 23.0 × 104 |
| Coagulation | ||
| PT (%) | 70-130 | 94 |
| PT-INR | 0.8-1.2 | 1.04 |
| APTT (s) | 25-45 | 26.7 |
| Fibrinogen (mg/dL) | 200-400 | 521 |
| Chemistry | ||
| TP (g/dL) | 6.5-8.5 | 7.3 |
| Alb (g/dL) | 4.1-5.3 | 4.2 |
| AST (IU/L) | 10-35 | 14 |
| ALT (IU/L) | 10-35 | 14 |
| LDH (IU/L) (IFCC) | 124-222 | 112 |
| ALP (IU/L) (IFCC) | 72-113 | 78* |
| g-GT (IU/L) | 8-60 | 27 |
| T-Bil (mg/dL) | 0.2-1.3 | 0.9 |
| T-Chol (mg/dL) | 150-219 | 150 |
| BUN (mg/dL) | 9.6-22.0 | 15.5 |
| UA (mg/dL) | 2.0-6.9 | 6.1 |
| Crea (mg/dL) | 0.50-1.10 | 0.76 |
| CRP (mg/dL) | 0.00-0.30 | 7.37 |
| Viral markers | ||
| HBsAg (COI) | 0.00-0.99 | 0.37 |
| HCVAb (COI) | 0.0-0.9 | 0.0 |
| HIV | (-) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal Tumor Research and Treatment · Gastrointestinal disorders and treatments · Gastrointestinal Bleeding Diagnosis and Treatment
Introduction
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumors involving the gastrointestinal (GI) tract, with an incidence of ~1.2 per 105 individuals per year [1]. Localized GISTs are curable, and surgery is the standard treatment [1]. However, some GISTs and their metastatic lesions may cause acute symptoms, such as GI or intra-abdominal bleeding, requiring urgent surgical resection, endoscopic intervention, or transcatheter arterial embolization (TAE) [2-11]. Though acute bleeding is one of the complications associated with GISTs, the most common mode of bleeding is GI bleeding, and extraluminal bleeding is rare [12-14]. In Japan, 21 cases of extraluminal bleeding from GISTs have been reported, and of the 21 cases, only two cases underwent emergency TAE for the bleeding [13]. Thus, it is assumed that most cases of extraluminal bleeding from GISTs have undergone emergency surgical resection so far. However, TAE is a less invasive procedure than surgery and is effective for other gastric malignant tumor-related GI bleeding [15,16]. This report describes a case of intra-abdominal bleeding from a ruptured, extraluminally growing gastric GIST in which TAE stopped the bleeding, and the tumor was then later resected surgically. We staged GISTs using Fletcher’s and Miettinen’s classification systems. And we determined a conversion factor of 0.34 to convert serum ALP levels measured by the Japan Society of Clinical Chemistry (JSCC) method to corresponding values measured by the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) method.
Brief summary
We experienced hemostasis achieved through TAE for an extraperitoneally ruptured gastric GIST presenting with intra-abdominal hemorrhage. This case highlights the potential of transcatheter arterial angiography and embolization for rapid diagnosis of the bleeding site and effective hemostasis in GISTs with intra-abdominal bleeding.
Case presentation
A 49-year-old man was referred to our hospital complaining of epigastralgia, right-sided abdominal pain, and shoulder pain. His epigastralgia had started two days earlier and had continued. On admission, his pulse rate was 80 beats/minute, and his blood pressure was 159/100 mmHg. His palpebral conjunctivae were normal in color, and there was no yellowish discoloration of his bulbar conjunctiva. His abdomen was flat and soft, but he had tenderness in both the epigastric region and the right hypochondrium. On abdominal palpation, there was no clear abdominal mass lesion. He had no history of abdominal trauma or abdominal bruises.
Contrast-enhanced abdominal computed tomography (CT) showed a large heterogeneous tumor with a non-uniform enhancement pattern in the extraluminal space of the gastric anterior wall and intra-abdominal peri-hepatic fluid collection (Figures 1a-1c). Though a ruptured intra-abdominal mass lesion with intra-abdominal bleeding was suspected, the primary lesion of the mass could not be diagnosed. Because the patient was hemodynamically stable and the laboratory data on admission showed mild anemia and an increased C-reactive protein (CRP) level (Table 1), abdominal angiography was performed to diagnose the mass lesion and to treat it with arterial embolization if bleeding from it continued.
Abdominal computed tomography (CT) on admission showing an intra-abdominal peri-hepatic fluid collection with high density, which could suggest hemoperitoneum. (a) Early phase. (b) Portal phase. (c) Delayed phase.Contrast-enhanced abdominal CT shows a large heterogeneous mass with a non-uniform enhancement pattern (white arrow) at the extraluminal space of the gastric anterior wall and intra-abdominal peri-hepatic fluid collection.
Abdominal angiography showed extravasation of contrast in the abdominal cavity (Figures 2a-2c). The blood supply of the tumor was from the epiploic branch of the right gastroepiploic artery, and the angiography showed extravasation from the epiploic branch. Based on the angiographic findings, the tumor appeared to be of gastric or greater omental origin. Because of the extravasation from the tumor-feeding artery, TAE was performed to the epiploic branch with a porous gelatin sponge (Serescue®: Astellas Pharma Inc., Tokyo, Japan). After embolization, selective right gastroepiploic artery angiography showed no extravasation from the tumor-feeding artery. Following the procedure, the patient had no abdominal symptoms, and his vital signs were stable.
Abdominal angiography of the tumor.(a) Supra-mesenteric artery angiography. The arrow shows extravasation of contrast.(b) Selected right gastroepiploic artery angiography. The arrow shows extravasation of contrast. The arrowhead points to the epiploic branches of the right gastroepiploic artery, which supplies blood to the tumor.(c) Selective right gastroepiploic artery angiography post-embolization. Tumoral arterial extravasation is absent following embolization.
Several days later, the patient underwent esophagogastroduodenoscopy (EGD), and a mild erosion was seen surrounding the normal mucosa at the antrum (Figures 3a, 3b). The patient declined both endoscopic ultrasound (EUS) surveillance and preoperative tissue diagnosis by EUS-guided fine needle aspiration (EUS-FNA). Following TAE, the tumor underwent surgical resection (Figures 4a, 4b). The tumor was successfully dissected from the stomach, duodenum, and gallbladder, allowing for a tumorectomy. Interestingly, the hemorrhage point of the tumor could not be identified in the surgically resected specimen. The pathological findings showed myxomatous stroma with cells having epithelioid features (Figures 5a, 5b). Immunostaining of the tumor showed that the cluster of differentiation 34 (CD34) was positive and discovered GIST 1 (DOG1) was weakly positive (Figures 5c, 5d). In addition, the platelet-derived growth factor receptor alpha (PDGFRA) mutation (D842V) was detected within the tumor. Finally, the diagnosis was extraluminally growing gastric GIST with pathological findings of PDGFRA mutation in a GIST derived from gastric parietal cells and intra-abdominal hemorrhage from the GIST.
Esophagogastroduodenoscopy (EGD) showing a mild erosive lesion at the antrum (arrow).(a) Regular white light endoscopic image.(b) Chromoendoscopic image with indigo carmine staining of the gastric mucosal surface.
(a) Surgical intervention to remove the yellowish mass. (b) The cut surface of the tumor shows a heterogeneous yellowish area and includes the hemorrhagic or necrotic regions.
Histopathological findings.(a) Histopathological findings of the tumor stained with hematoxylin-eosin in a low-power view (×10). The tumor consists of a high density of hyperplastic tumor cells. (b) The nuclei of the tumor cells appear oval or spindle-shaped in a high-power view (×40). (c) The tumor shows positive staining for a cluster of differentiation 34 (CD34) in a low-power view (×10). (d) The tumor shows weakly positive staining for DOG1 in a low-power view (×10).
In this case, the ruptured GIST in the abdominal cavity posed a risk of disseminating tumor cells throughout the peritoneal cavity. The resected tumor, a 160 × 110 × 35 mm mass, classified as high-risk according to Fletcherʼs classification and Miettinenʼs classifications, could have also led to this outcome. However, due to the known resistance of GISTs harboring PDGFRA D842V mutations to imatinib, the patient was closely monitored without receiving adjuvant chemotherapy after surgery. Notably, even with this high-risk profile, the patient remains free of recurrent disease two years post-resection.
Discussion
Abdominal vascular emergencies, especially intra-abdominal hemorrhage, are frequently catastrophic and highly lethal [17]. Therefore, early diagnosis and treatment of vascular emergent diseases are important. Though surgery is effective for tumor-related intra-abdominal bleeding, it is invasive and a burden for the patient. TAE offers a less-invasive alternative to surgery for tumor-related hemorrhage [15,16]. Its effectiveness stems from its ability to rapidly achieve hemostasis, even in hemodynamically unstable patients, due to its precise targeting and potent hemostatic effects. Thus, it was possible to provide prompt treatment to stop the hemorrhage in the present case by TAE. On CT imaging at admission, GIST could not be diagnosed; it could only be diagnosed after surgical resection. However, abdominal angiography was performed for the intra-abdominal bleeding from this undiagnosed tumor, and effective hemostasis was obtained. Transcatheter arterial angiography may be considered first for intra-abdominal bleeding from a cryptogenic mass lesion.
In the present case, the tumor’s origin could not be determined on contrast-enhanced abdominal CT. However, it could be assumed that the tumor was of gastric or greater omental origin because of the existence of a tumor-feeding artery from the epiploic branch of the right gastroepiploic artery. Knowing which organ is the origin of the tumor is important for surgical resection after hemostasis by embolization. Other than for GI bleeding cases, for which other useful and effective treatment procedures, such as endoscopic intervention, are indicated, TAE should be performed for bleeding from a tumor lesion as an emergency procedure.
The complications of TAE include organ ischemic injury, access site arterial trauma, contrast-induced nephropathy, and embolization of nontarget vessels [18]; therefore, TAE treatment should not be considered the only first-line option for intra-abdominal bleeding from a tumor lesion instead of surgery. However, for patients in an unstable condition, such as those with continuing hypotension or hypovolemic shock, transcatheter arterial angiography with embolization is one of the useful procedures for intra-abdominal bleeding to avoid the risks of emergency surgery and then perform elective surgery when the patient has been stabilized.
Conclusions
Although hemorrhage is a common complication of GISTs, the intra-abdominal bleeding presented in our case differed from the typical type of GI bleeding. While endoscopic procedures may be suitable for GIST-related GI bleeding, for cases of intra-abdominal bleeding from any tumor, including GISTs, even with stable vital signs, emergency transcatheter arterial angiography and embolization should be considered as a potential approach for rapid diagnosis of the bleeding site, precise tumor localization, and effective hemostasis.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gastrointestinal stromal tumours Nat Rev Dis Primers Blay JY Kang YK Nishida T von Mehren M 22720213373751010.1038/s 41572-021-00254-5 · doi ↗ · pubmed ↗
- 2A gastrointestinal stromal tumor with acute bleeding: management and nursing Medicine (Baltimore) Shi X Yu S Wang F Zhao Q Xu H Li B 097201810.1097/MD.0000000000009874 PMC 585172329489686 · doi ↗ · pubmed ↗
- 3A rare case of a ruptured metastatic hepatic lesion from a jejunal gastrointestinal stromal tumor (GIST) treated by arterial embolization Am J Case Rep Salame H Issa M Nicolas G 148014871920183054204910.12659/AJCR.910061 PMC 6302770 · doi ↗ · pubmed ↗
- 4A ruptured large extraluminal ileal gastrointestinal stromal tumor causing hemoperitoneum World J Gastroenterol Hirasaki S Fujita K Matsubara M 292829311420081847342510.3748/wjg.14.2928 PMC 2710742 · doi ↗ · pubmed ↗
- 5A ruptured recurrent small bowel gastrointestinal stromal tumour causing hemoperitoneum Front Med Lai EC Chung KM Lau SH Lau WY 108111920152500110210.1007/s 11684-014-0344-0 · doi ↗ · pubmed ↗
- 6Acute diffuse peritonitis due to spontaneous rupture of a primary gastrointestinal stromal tumor of the jejunum: a case report Int J Surg Case Rep Sato K Tazawa H Fujisaki S 2882923920172888891410.1016/j.ijscr.2017.08.041PMC 5596258 · doi ↗ · pubmed ↗
- 7Diagnostic and therapeutic approach to obscure gastrointestinal bleeding in a patient with a jejunal gastrointestinal stromal tumor: a case report BMC Res Notes Yuval JB Almogy G Doviner V Bala M 695720142528711910.1186/1756-0500-7-695PMC 4197232 · doi ↗ · pubmed ↗
- 8Efficacy and clinical outcomes of transcatheter arterial embolization for gastrointestinal bleeding from gastrointestinal stromal tumor J Vasc Interv Radiol Koo HJ Shin JH Shin S Yoon HK Ko GY Gwon DI 129713042620152619018610.1016/j.jvir.2015.06.005 · doi ↗ · pubmed ↗