Deadly Aspiration Pneumonia Secondary to Superior Mesenteric Artery Syndrome
Rhea Akel, Iskandar Daou, Dany Jamal, Elham Hobeika, Rany Aoun, Georges Nawfal

TL;DR
A rare case of Superior Mesenteric Artery Syndrome led to fatal aspiration pneumonia due to delayed diagnosis.
Contribution
Highlights the importance of early diagnosis of SMAS to prevent life-threatening complications.
Findings
SMAS can cause upper gastrointestinal obstruction leading to aspiration pneumonia.
Delayed diagnosis of SMAS can result in severe complications and death.
Clinical and radiological correlation is essential for accurate SMAS diagnosis.
Abstract
Superior mesenteric artery syndrome (SMAS) is a rare and unusual disease, suspected clinically and confirmed radiologically. It represents a duodenal obstruction secondary to the impingement of the third portion of the duodenum between the abdominal aorta (AA) and the superior mesenteric artery (SMA) due to decreased intraabdominal fat. High morbidity and mortality rates are linked to missed or late diagnosis that can lead to complications, such as gastric perforation and gastric hemorrhage. We present the case of a 33-year-old man who was not previously known to have a SMAS, who presented to the emergency department with signs of septic shock, complaining of fever and respiratory symptoms for several days. Investigations showed aspiration pneumonia secondary to an upper gastrointestinal obstruction with signs of SMAS on a computed tomography (CT) scanner. Acute and rapid deterioration…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1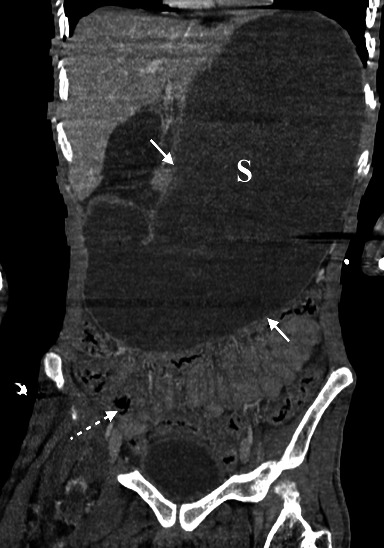 Figure 2
Figure 2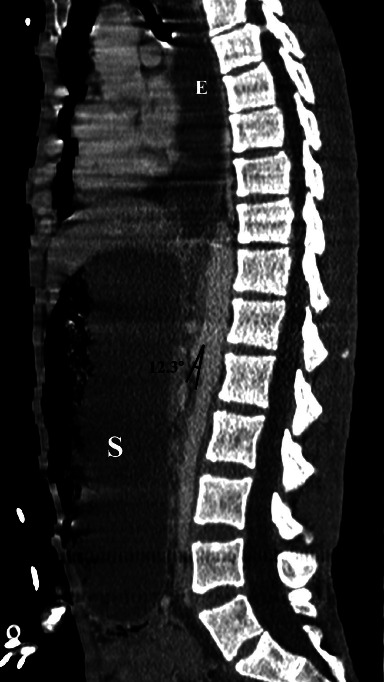 Figure 3
Figure 3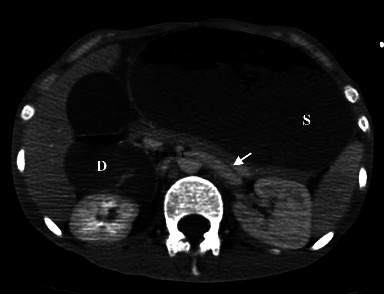 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular anomalies and interventions · Renal and Vascular Pathologies · Coronary Artery Anomalies
1. Introduction
Superior mesenteric artery syndrome (SMAS) is a rare and unusual disease. It is considered to be a form of chronic duodenal ileus [1] and represents a duodenal obstruction secondary to the impingement of the third portion of the duodenum between the abdominal aorta (AA) and the superior mesenteric artery (SMA) due to decreased intraabdominal fat [2]. Clinical symptoms raise suspicion for this diagnosis which can be confirmed by radiological testing [3]; however, the diagnosis remains challenging and the approach for SMAS diagnosis remains controversial [1]. It is known that a delayed or missed diagnosis is linked to high morbidity and mortality rates secondary to complications, making it a crucial differential to be considered when there is a duodenal obstruction, especially in the setting of rapid weight loss [3].
2. Case Presentation
A 33-year-old man presented to the emergency department (ED), complaining of worsening fever, dyspnea, vomiting, and productive cough for 5 days, and an acute onset desaturation. The patient suffers from schizophrenia and has been treated for more than 20 years by using several neuroleptic drugs. From about 6 months ago, his psychiatric condition was not well controlled by medication, and he started weight loss due to low food intake.
His vital signs were as follows: temperature of 39.6°, heart rate of 147 beats per minute, blood pressure of 100/50 mmHg, and oxygen saturation of 80% on room air. His body mass index (BMI) was 14.5 kg/m^2^ (6 months ago, it was about 19.42 kg/m^2^). Physical examination on admission showed a conscious, noncooperant cachectic and dyspneic patient, with tachycardia but no murmurs. Pulmonary auscultation showed bilateral wheezing and bronchial congestion. Abdominal examination revealed epigastric tenderness, and no urinary symptoms were mentioned.
Blood tests showed elevated white blood cell count (13,300/mm^3^) and a protein C level at 26 mg/l. The alkaline reserve was 12.1 mmol/l. Creatinine, liver function tests, sodium, potassium, and chloride levels were within normal limits. A computed tomography (CT) of the chest, abdomen, and pelvis with intravenous contrast material was ordered and revealed bilateral multifocal parenchymal condensations with multiple ground-glass opacities predominant in the lower lobes, suggestive of aspiration pneumonia (Figure 1).
In addition, there was an extremely important distension of the esophagus, stomach, and proximal duodenum (Figure 2), that is, an upstream of an abrupt transition zone involving a decompressed caliber in the third part of the duodenum at the level of its crossing in the mesenteric clamp. The rest of the bowel loops were of normal appearance. No intraabdominal collection, parietal pneumatosis, or pneumoperitoneum were noted. The angle between the proximal SMA and the AA, also known as the aortomesenteric angle, was narrow, at 12.3° (Figure 3) and the aortomesenteric distance was 3.5 mm (Figure 4), suggestive of a SMAS. Also, the left renal vein was distended before its course in the mesenteric clamp.
Initial management included hydration, nasal oxygen, bronchodilators, nasogastric tube insertion, antipyretics, steroids, and hypercaloric total parenteral nutrition (2500 kilocalories per day). Empiric intravenous antibiotics (levofloxacin 500 mg daily and piperacillin/tazobactam 4.5 g QID) were started after blood and urine cultures. Evolution showed severe rapid clinical degradation that resulted in a cardiac arrest and death.
The diagnosis of a severe septic shock due to aspiration pneumonia secondary to SMAS was made.
3. Discussion
SMAS, also known as Wilkie's syndrome, was first described as a case report in 1842 by Carl Von Rokitansky and further detailed by Wilkie in 1927 [3, 4]. Other names for this syndrome include cast syndrome, chronic duodenal ileus, and aortomesenteric duodenal compression. It is a rare entity with an incidence estimated at 0.1%–0.3% [3]. This disease occurs preferentially in young adults and adolescents with an age range between 10 and 39 years, but it can occur at any age, and is more prevalent in females with a ratio of 3 females to 2 males [3]. No ethnic predisposition has been proven; however, familial cases have been reported [5].
The pathophysiology of this syndrome is explained by an important decrease of intraabdominal fat, causing a decrease of the intervening mesenteric fat pad between the AA and the SMA, resulting in a narrow aortomesenteric angle and distance [2]. The duodenal fat pad cushion is responsible for holding the SMA off the vertebral column and protecting it from duodenal compression [3].
In healthy individuals, the aortomesenteric angle ranges from 28° to 65° and the aortomesenteric distance ranges from 10 to 34 mm [6]. In SMAS, when the fat pad cushion becomes thin, the SMA leaves the AA at an abnormally hyperacute angle, typically less than 25°, and runs closer to the aorta, typically at a distance of less than 8 mm, depending on the BMI of the patient [2]. It is important to note that no number is strictly diagnostic, and radiological images must be interpreted in light of the clinical history and physical examination, which makes the diagnosis even more challenging [2].
Other characteristic findings on the CT scanner are distention of the stomach and proximal duodenum with bowel caliber narrowing at the origin of the SMA from the AA [7].
Our patient, in addition to being cachectic due to his psychiatric condition with a very low BMI of 14,5 kg/m^2^, had a hyperacute aortomesenteric angle and short aortomesenteric distance measuring 12.3° and 3.5 mm, respectively, with esophago-gastro-duodenal distension proximal with a transition zone at the takeoff of the SMA from the AA on the CT scanner. He was also treated with several neuroleptic drugs. Some of the known side effects of antipsychotic drugs are bowel hypoperistalsis and constipation [8].
Recent weight loss and symptoms of bowel obstruction should alert physicians to this condition. Late diagnosis has been linked to severe morbidity and mortality [3], emanating from electrolyte abnormalities, dehydration, malnutrition, gastric pneumatosis, portal venous gas, gastric perforation, and hemorrhage [9–11].
Our patient presented to the ED with signs of septic shock, pneumonia, and vomiting. The predominant distribution of the diffuse alveolar infiltrates, ground-glass opacities, and condensations in the lower lobes on the chest CT scan, has allowed us to make the diagnosis of aspiration pneumonia. In aspiration pneumonia, the right lower lobe is most frequently affected, and if aspiration occurs while in the prone position, both lower lobes might be involved [12].
Once the diagnosis is made, in the acute setting, conservative medical management is the initial treatment, including hydration, electrolyte correction, nasogastric tube insertion for gastric decompression, and total parenteral nutrition [3], which were all applied in our case. Nutritional support through hyperalimentation is added during conservative therapy in an attempt to increase the duodenal fat pad cushion, thus increasing the aortomesenteric angle and distance, thereby decreasing the duodenal compression and improving symptoms [3].
Albeit, many patients will fail the conservative measures and will require undergoing invasive procedures such as total parenteral nutrition, lysis of ligament of Treitz (strong procedure), transabdominal or laparoscopic duodenojejunostomy, percutaneous jejunostomy tube placement, and enteral tube placement [3, 7].
Our patient also received large broad-spectrum antibiotics based on a combination of levofloxacin and piperacillin/tazocin to treat the septic shock secondary to aspiration pneumonia.
The most common cause of death in SMAS is gastric perforation and hemorrhage [9–11]. Mortality due to aspiration pneumonia secondary to SMAS has not been described yet. Jung and Koo reported a case of a patient with SMAS, who presented with aspiration pneumonia secondary to induction of general anesthesia, and had a favorable outcome [13].
In our case, the patient received appropriate initial management for septic shock, duodenal obstruction, and SMAS, and the rapid clinical deterioration resulted in cardiac arrest and death.
4. Conclusion
SMAS is an unusual and challenging diagnosis that is made based on clinical suspicion and characteristic findings. Early and accurate diagnosis is a must to avoid serious complications that can lead to high morbidity and mortality rates. Gastric perforation and hemorrhage are considered the most common causes of death in SMAS. However, it is important to note that aspiration pneumonia in the setting of SMAS can be life-threatening when diagnosis is delayed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Salehi A. M. Salehi H. Hasanzarrini M. Khanlarzadeh E. Report of a misleading case of the superior mesenteric artery syndrome Case Reports in Gastrointestinal Medicine 202220223601357910.1155/2022/6013579 PMC 916698035669382 · doi ↗ · pubmed ↗
- 2England J. Li N. Superior mesenteric artery syndrome: a review of the literature Journal of the American College of Emergency Physicians Open 202123 p. e 1245410.1002/emp 2.12454 PMC 821255734179879 · doi ↗ · pubmed ↗
- 3Van Horne N. Jackson J. P. Superior Mesenteric Artery Syndrome 2023 Petersburg, FL, USA Stat Pearls Publishing 29489172 · pubmed ↗
- 4Ehlers T. O. Tsamalaidze L. Pereira L. Stauffer J. Laparoscopic duodenojejunostomy for the SMA syndrome Zentralbl Chir 2018143546146310.1055/a-0668-19912-s 2.0-8505560707830357787 · doi ↗ · pubmed ↗
- 5Hillyard J. Solomon S. Kaspar M. Chow E. Smallfield G. Gastrointestinal: reversal of superior mesenteric artery syndrome following pregnancy Journal of Gastroenterology and Hepatology 2019343 p. 48610.1111/jgh.144752-s 2.0-8505466242030302852 · doi ↗ · pubmed ↗
- 6Inal M. Unal Daphan B. Karadeniz Bilgili M. Y. Superior mesenteric artery syndrome accompanying with nutcracker syndrome: a case report Iranian Red Crescent Medical Journal 20141610 p. e 1475510.5812/ircmj.147552-s 2.0-84930006822 PMC 432974625763192 · doi ↗ · pubmed ↗
- 7Warncke E. S. Gursahaney D. L. Mascolo M. Dee E. Superior mesenteric artery syndrome: a radiographic review Abdom Radiol (NY) 20194493188319410.1007/s 00261-019-02066-42-s 2.0-8506765372731127323 · doi ↗ · pubmed ↗
- 8Stroup T. S. Gray N. Management of common adverse effects of antipsychotic medications World Psychiatry 201817334135610.1002/wps.205672-s 2.0-8505297626030192094 PMC 6127750 · doi ↗ · pubmed ↗