Early Recovery of Physical Function After Total Hip Arthroplasty in a Patient With Osteopetrosis: A Case Report
Shusuke Nojiri, Azusa Kayamoto, Chiaki Terai, Yusuke Osawa, Yasuhiko Takegami

TL;DR
A patient with osteopetrosis successfully recovered physical function after hip replacement surgery using standard rehabilitation methods.
Contribution
This case demonstrates that standard rehabilitation protocols can be effective for osteopetrosis patients after hip arthroplasty.
Findings
The patient walked independently with a cane 17 days post-surgery.
Maximal walking speed and hip abductor strength improved post-operation.
No adverse events occurred during the rehabilitation process.
Abstract
Osteopetrosis is an uncommon and inherited disorder. Some disease-specific characteristics, such as diffuse osteosclerosis and a high incidence of fractures, may potentially affect postoperative rehabilitation. This report presents a case of successful rehabilitation early after total hip arthroplasty for osteopetrosis. A 56-year-old Japanese man, who was diagnosed with osteopetrosis at the age of 11, underwent total hip arthroplasty in the right hip. Full weight-bearing was allowed on the day after the operation; the postoperative rehabilitation program was proceeded based on a standard program as done after total hip arthroplasty for osteoarthritis. A shoe lift in the left leg was used in supervised walking training to correct the imbalanced alignment due to leg length discrepancy. The patient could walk independently with a cane 17 days after the operation. Three weeks after the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
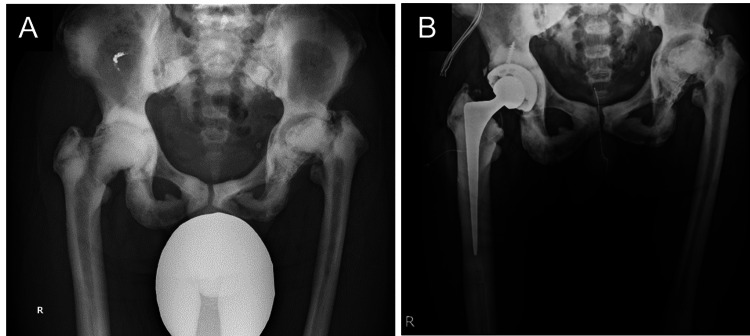 Figure 1
Figure 1 Figure 2
Figure 2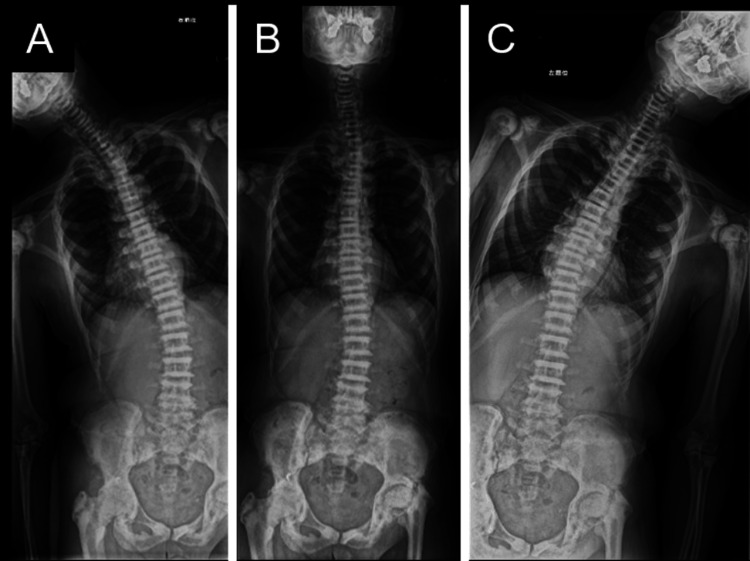 Figure 3
Figure 3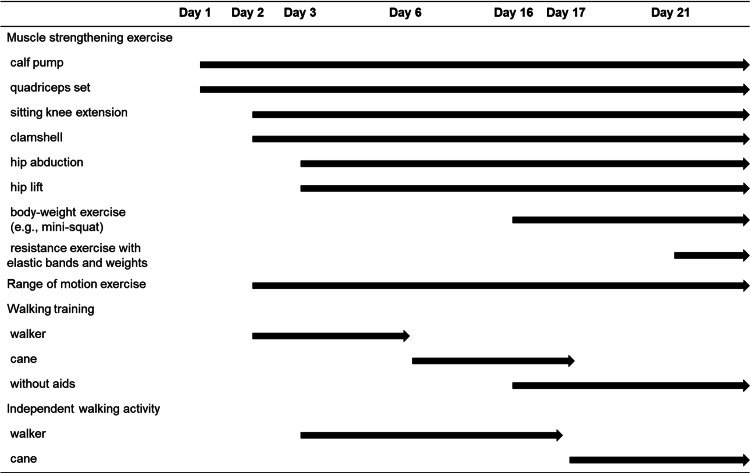 Figure 4
Figure 4| Preoperation | |
| Range of motion (degree; right/left) | |
| Hip flexion | 90/80 |
| Hip extension | 0/0 |
| Hip abduction | -5/10 |
| Hip adduction | 15/10 |
| Muscle strength | |
| Handgrip (kgf; right/left) | 42.2/40.4 |
| Hip abduction (kgf・m; right/left) | 2.67/2.88 |
| Knee extension (kgf・m; right/left) | 12.15/15.26 |
| Walking ability | |
| Comfortable speed (m/s) | 0.76 |
| Maximal speed (m/s) | 0.90 |
| Walking aid | none |
| PLLD (cm) | 1.5 (right longer than left) |
| Preoperation | POD 20 | POD 27 | ||
| Muscle strength in the right lower limb (kgf・m) | ||||
| Hip abduction | 2.67 | 3.96 | 4.50 | |
| Knee extension | 12.15 | 7.38 | 11.50 | |
| Walking ability | ||||
| Comfortable speed (m/s) | 0.76 | 1.11 | 0.99 | |
| Maximal speed (m/s) | 0.90 | 1.34 | 1.39 | |
| Walking aid | None | |||
| Hip pain (NRS) | 4 | 0 | 0 | |
| PLLD (cm; right longer than left) | 1.5 | - | 4.0 | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Metabolism and Diseases · Pharmacological Effects of Medicinal Plants · Bone health and osteoporosis research
Introduction
Osteopetrosis, also referred to as "marble bone disease," is an uncommon and inherited disorder, characterized by impaired osteoclast function resulting in hard and brittle bone. Osteopetrosis is associated with a high risk of fracture, osteoarthritis (OA), and poor fracture healing with non-union [1].
For individuals with hip OA, total hip arthroplasty (THA) is an effective treatment for reducing pain and improving joint function. Recovery of physical function, such as lower-limb muscle strength and walking speed, after THA in patients with OA is well documented [2-4]. However, in patients with osteopetrosis, THA is associated with technical difficulties and a higher risk of complications [5,6]. In addition to surgical techniques, some potential risk factors related to postoperative rehabilitation may exist in patients with osteopetrosis after THA. Patients with osteopetrosis commonly exhibit skeletal deformities, including scoliosis, spondylolisthesis, and degenerative arthritis [7]. Diffuse osteosclerosis and a high incidence of fractures are typical examples [8]. Considering the higher risk of intra- and postoperative complications, the rehabilitation course after THA in patients with osteopetrosis may differ from that in patients with OA; however, there is a lack of knowledge regarding the safety and efficacy of rehabilitation after THA in patients with osteopetrosis. This report presents a case of successful rehabilitation early after THA for osteopetrosis.
Case presentation
Patient information
A 56-year-old Japanese man (height, 173 cm; body weight, 73.8 kg), who was diagnosed with osteopetrosis at the age of 11, has suffered from bilateral hip pain (left greater than right) for several decades due to hip OA associated with osteopetrosis (Figure 1A). In the last few years, however, the patient experienced rapidly worsening pain in the right hip and progressive activity limitation and therefore was scheduled for THA in the right hip. Japanese Orthopedic Association score was 51 and 61 out of 100 points, for the right and left hip, respectively [9]. Preoperative X-rays indicated leg length discrepancy (LLD) (right longer than left) due to more progressive hip OA in the left and poor lateral flexion flexibility in the lumbar spine (Figures 2, 3).
X-ray images of the hipA, preoperative X-ray image; B, postoperative X-ray imageHip osteoarthritis associated with osteopetrosis was observed in both sides.
Preoperative full-leg X-ray image
Preoperative X-ray images of the spineA, right lateral flexion; B, neutral; C, left lateral flexionPoor lateral flexion flexibility in the lumbar spine was indicated.
The patient had a fracture history in the rib and was treated conservatively. The patient’s father and sister also have a known history of osteopetrosis. As scheduled, THA in the right hip was performed via posterior approach without any intraoperative complications (Figure 1B). The operation time and blood loss were 142 minutes and 597 mL, respectively. There were no adverse events during the hospitalization. On postoperative day (POD) 29, the patient was transferred to a different hospital to continue rehabilitation training as the patient expected.
Preoperative physical function
Preoperative physical function was assessed on the day before the operation (Table 1). Lower limb muscle strength (hip abduction and knee extension) was measured during a 5-s isometric contraction using a handheld dynamometer with a restraining belt (μTas; Anima Corp., Tokyo, Japan). The measurement was performed in a supine with the hip and knee in a neutral position and sitting on the edge of a platform with the knee in 60-degree flexion for the hip abduction and knee extension, respectively. Comfortable and maximal walking speeds were measured over the middle 10 m of a 16-m walkway. In summary, the patient had good muscle strength in both the upper and lower limbs but demonstrated decreased walking speed (<1.0 m/s). In addition, the patient felt a perceived LLD of 1.5 cm in the right limb longer than the left.
Postoperative rehabilitation course
The postoperative rehabilitation course is presented in Figure 4. Full weight-bearing was allowed from POD 1. On POD 1, the patient was able to stand up and transfer to the wheelchair. The patient started supervised walking training on POD 2 using walking aids and a shoe lift in the left leg for correcting LLD. Shoe lift, started from 4.0 cm on POD 2, remained in use at the supervised training and was decreased gradually. On POD 3, the patient achieved unsupervised walking with a walker; however, the patient was instructed not to increase physical activity because of the imbalanced alignment due to the LLD. On POD 9, the appropriate shoe lift was decided as 2.5 cm based on the structural LLD and prescribed. On POD 17, the patient received the lifted shoe; at the time, the patient was allowed to walk independently with a cane and instructed to increase physical activity. Enhanced muscle strengthening exercise using elastic bands and weights was added on POD 21.
Postoperative rehabilitation course
Postoperative physical function
Postoperative physical function was assessed via lower-limb muscle strength and walking speed on POD 20 and POD 27 (Table 2). Except for the knee extension muscle strength, the patient demonstrated better performance than preoperation at both postoperative time points. Although the knee extension muscle strength decreased at POD 20, it recovered to almost the same extent as preoperative at POD 27. The perceived LLD remained at 4.0 cm on POD 27.
Discussion
In this report, we described a rehabilitation course and functional recovery after THA in a patient with osteopetrosis. Although slight modifications by the shoe list for correcting LLD were added, we basically provided a standard rehabilitation program after THA, as is done in patients with OA (e.g., gradually increasing muscle strength exercise and walking training). Our result suggests the safety of a standard rehabilitation program after THA even in patients with osteopetrosis.
In individuals with osteopetrosis, some disease-specific factors, such as diffuse osteosclerosis and high incidence of fractures, could have a negative impact on postoperative rehabilitation. In the present case, there were no adverse events during the postoperative rehabilitation course, both in affected and non-affected regions. These results imply the safety of a standard rehabilitation and reinforce the suggestion by Gao et al. [10]. They reported a case of a 52-year-old female patient with osteopetrosis who was able to walk with sticks 18 days after THA and stated that postoperative functional exercises for patients with osteopetrosis ought to be carried out “as usual.”
Our interventions of taking into consideration the whole body, such as the contralateral hip and spine, may have contributed to the safe and effective rehabilitation course. In individuals with osteopetrosis, in particular, it may be important for therapists to consider the whole-body condition, since osteopetrosis often presents non-localized problems. Difficulties in surgical techniques may also be related to this perspective; sometimes, LLD could not be able to corrected with the contralateral THA. In this case, the patient had other problems than hip OA in the right hip, such as more progressive hip OA in the left and poor spine lateral flexion flexibility. Hence, to avoid the overloads in the abovementioned regions, we used a shoe lift in the contralateral leg to correct LLD in the early phase after THA, and we instructed the patient not to increase physical activity until the shoe lift was ready.
In terms of functional recovery, such as muscle strength and walking function, the early recovery in the present case is comparable or somewhat superior to that after THA in patients with OA. Previous studies regarding functional recovery after THA in patients with OA have reported that physical function decreased one month after the operation compared to preoperation and recovered later [3,4]. In this case, better hip abduction muscle strength and walking speed than preoperation were observed three weeks after the operation. When the postoperative rehabilitation is carried out safely, good recovery in muscle strength and walking function could be expected even in individuals with osteopetrosis. Another potential reason for the early recovery in this case is good preoperative physical function. It has been well established that preoperative physical function, including nonoperating regions, is an important factor for postoperative rehabilitation courses and clinical outcomes [11-13]. The patient in the present case had a relatively good preoperative physical performance compared to those undergoing THA, and therefore the early recovery was achieved.
Conclusions
In this case report, we describe a rehabilitation course and functional recovery after THA in a patient with osteopetrosis. Our intervention with the consideration for the whole-body condition may have contributed to the safety rehabilitation. The patient showed good recovery of muscle strength and walking speed within one month. Even in individuals with osteopetrosis, good recovery in muscle function may be expected, as a result of safety rehabilitation. In rehabilitation of patients with osteopetrosis, skeletal complications, such as fractures, should be noted. Further studies with larger sample sizes would be needed to confirm our findings.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Osteopetrosis. Current clinical considerations Clin Orthop Relat Res Shapiro F 33441993 https://europepmc.org/article/med/83589408358940 · pubmed ↗
- 2Abductor muscle strength deficit in patients after total hip arthroplasty: a systematic review and meta-analysis J Arthroplasty Ismailidis P Kvarda P Vach W Cadosch D Appenzeller-Herzog C Mündermann A 301530273620213386720810.1016/j.arth.2021.03.042 · doi ↗ · pubmed ↗
- 3Muscle strength and functional recovery during the first year after THA Clin Orthop Relat Res Judd DL Dennis DA Thomas AC Wolfe P Dayton MR Stevens-Lapsley JE 65466447220142381775610.1007/s 11999-013-3136-y PMC 3890211 · doi ↗ · pubmed ↗
- 4Changes in hip and knee muscle strength in patients following total hip arthroplasty J Jpn Phys Ther Assoc Fukumoto Y Ohata K Tsukagoshi R 22271620132579290010.1298/jjpta.Vol 16_002PMC 4316546 · doi ↗ · pubmed ↗
- 5Total hip arthroplasty in patients with osteopetrosis J Arthroplasty Siljander MP Trousdale RT Perry KI Mabry TM Berry DJ Abdel MP 136713723620213316227710.1016/j.arth.2020.10.018 · doi ↗ · pubmed ↗
- 6Osteopetrosis is associated with an increased risk for intraoperative periprosthetic fracture in total hip arthroplasty but not in total knee arthroplasty J Arthroplasty Burke JF Quinlan ND Werner BC Barnes CL Browne JA 24293820233597357410.1016/j.arth.2022.08.016 · doi ↗ · pubmed ↗
- 7Diagnosis and management of osteopetrosis: consensus guidelines from the osteopetrosis working group J Clin Endocrinol Metab Wu CC Econs MJ Di Meglio LA 3111312310220172865517410.1210/jc.2017-01127 · doi ↗ · pubmed ↗
- 8Genetics, pathogenesis and complications of osteopetrosis Bone Del Fattore A Cappariello A Teti A 19294220081793609810.1016/j.bone.2007.08.029 · doi ↗ · pubmed ↗