Hybrid Stent Implantation Into Right Ventricular Outflow Tract in a Newborn With Tetralogy of Fallot
Grzegorz Zalewski, Michał Buczyński, Michał Zawadzki, Paulina Kopacz, Jacek Kuźma

TL;DR
A newborn with heart defects received a hybrid stent to improve blood flow and delay major surgery.
Contribution
The use of hybrid stent implantation in a newborn with complex heart defects is described.
Findings
Hybrid stent implantation effectively improved pulmonary flow in the newborn.
The procedure allowed postponing corrective surgery due to anatomical constraints.
Abstract
A case is presented of a newborn with tetralogy of Fallot and aortic coarctation. Progressive right ventricular outflow tract (RVOT) obstruction required urgent surgical therapy. Coronary artery crossing the outflow tract made ventriculotomy impossible. Hybrid RVOT stent implantation was performed, providing effective pulmonary flow and enabling postponing of corrective jumping graft implantation.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
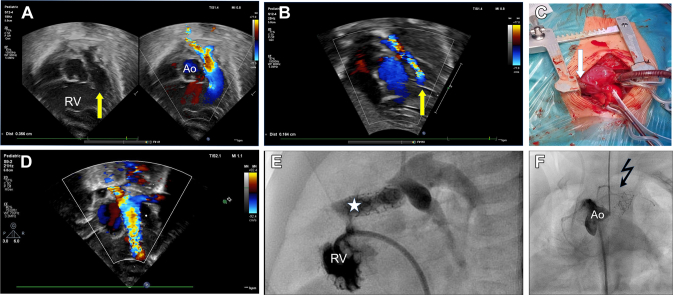 Figure 1
Figure 1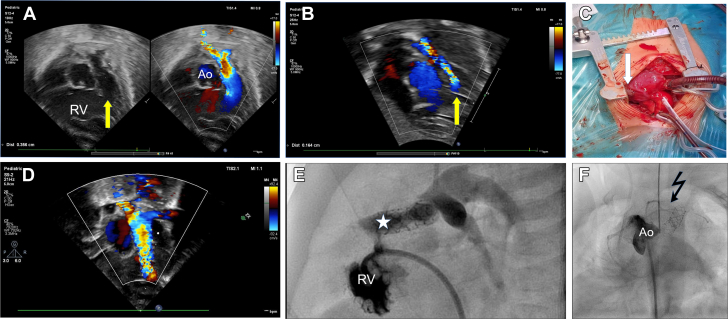 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCongenital Heart Disease Studies · Vascular anomalies and interventions · Coronary Artery Anomalies
Tetralogy of Fallot (TOF) is a challenging cyanotic heart defect requiring early palliative cardiac surgery or invasive therapy (eg, right ventriculotomy with patch dilation, systemic-pulmonary anastomosis, or interventional RVOT stent implantation) in symptomatic neonates with other risk factors (eg, low body weight, hypoplastic pulmonary arteries, abnormal coronary arteries crossing the RVOT, coexisting genetic syndromes, and organ defects).1, 2, 3
A case is presented of a premature newborn of 35 weeks of gestation and birth weight of 1,850 g. Multiorgan congenital defects were diagnosed, including unilateral lip and palate cleft, additional 13th pair of ribs, butterfly vertebra, left preauricular processes, and a heart defect.
Transthoracic echocardiography (TTE) revealed complex TOF with aortic valve dextroposition of 50%, a large ventricular septal defect of anterior malalignment type, mild subpulmonary stenosis (Figure 1A), hypoplastic pulmonary valve annulus (5 mm, Z score −2.0), normal pulmonary and coronary arteries, and right aortic arch with isthmus stenosis, which extremely rarely coexists with TOF (Video 1, Video 2, Video 3, Video 4). Within 14 days, hypoxemic spells appeared, with oxygen saturation of 70% without improvement after propranolol therapy. Both TTE and CT showed severe progression of the subpulmonary stenosis (Figure 1B, Video 5), requiring urgent palliative surgery in cross-clamp circulation. Intraoperative evaluation of the coronary arteries revealed wide coronary arteries crossing the RVOT (Figure 1C), which made ventriculotomy impossible. Systemic-pulmonary anastomosis was an alternative procedure, but because of the infant’s low body weight of 2.3 kg, hybrid RVOT stent implantation was performed via a small ventriculotomy just below the additional left anterior descending artery. A Palmaz Genesis 6-mm × 18-mm stent was deployed into the RVOT under epicardial echocardiography guidance. TTE confirmed a stable stent position and effective pulmonary flow (Figure 1D, Video 6). The Postoperative course was uneventful, with a high SaO_2_ of 90%, and the child was discharged home. At the 2-month follow-up visit, the child’s condition was stable, with sufficient SaO_2_ (80%); however, owing to progressive stent stenosis (Video 7) and aortic coarctation as shown by TTE, with a pressure gradient of 50 mm Hg, heart catheterization was performed with effective balloon aortoplasty (Tyshak 8-mm balloon catheter), and the pressure gradient dropped to 5 mm Hg. RV angiography revealed severe stent obstruction by hypertrophied muscular bands (Figure 1E, Videos 8 and 9) leading to pulmonary flow impairment and progressive hypoxia. Aortography confirmed 2 wide coronary arteries crossing the RVOT (Figure 1F, Videos 10 and 11) and normal left coronary artery (Video 12). After dilation of the isthmus, the SaO_2_ dropped to 70%, and the child required a palliative systemic-pulmonary 3.5-mm anastomosis between the left subclavian artery and the pulmonary trunk (Video 13), which improved the SaO_2_ ≤85%. The patient is awaiting corrective therapy with jumping graft implantation and ventricular septal defect closure.Figure 1. Progressive Right Outflow Tract Obstruction Despite Stent Implantation(A) Transthoracic echocardiogram (TTE). Subcostal view with color Doppler flow showing mildly stenotic right ventricular outflow tract (yellow arrow) on the first day of life with effective pulmonary flow. (B) TTE. Subcostal view with color Doppler flow showing severely stenotic right ventricular outflow tract (yellow arrow) impairing pulmonary flow. (C) Intraoperative view of coronary arteries with wide additional left anterior descending artery crossing outflow tract and a right ventriculotomy patch (white arrow) for hybrid procedure. (D) TTE. Subcostal view with color Doppler flow showing effective RV outflow tract flow through the implanted stent. (E) Right ventriculography in lateral view showing severe intraventricular stenosis by hypertrophied muscular bands obstructing the flow through the implanted stent (white star). (F) Aortography (CAU 40, CRA 30) showing right coronary artery, additional left anterior descending artery, and conal branch crossing outflow tract (dark jagged arrow). Ao = aorta; CAU = caudal; CRA = cranial; RV = right ventricle.
The authors conclude that careful follow-up observation of an infant with TOF is necessary because of the high risk of progressive RVOT obstruction with anoxemic spells. The staged palliative therapy is necessary in neonates with symptomatic TOF, low body weight, coexisting anomaly of the coronary arteries, and aortic coarctation. A hybrid approach with RVOT stent implantation is a safe and effective alternative solution in children with TOF anatomy unfavorable to other types of palliation (Supplemental Figure 1).
Funding Support and Author Disclosures
The authors have reported that they have no relationships relevant to the contents of this paper to disclose.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Luxford J.C.Adams P.E.Roberts P.A.Mervis J.Right ventricular outflow tract stenting is a safe and effective bridge to definitive repair in symptomatic infants with tetralogy of Fallot Heart Lung Circ 32520236386443696400510.1016/j.hlc.2023.02.010 · doi ↗ · pubmed ↗
- 2Qureshi A.M.Caldarone C.A.Romano J.C.Congenital Cardiac Research Collaborative Investigators. Comparison of management strategies for neonates with symptomatic tetralogy of Fallot and weight <2.5 kg J Thorac Cardiovasc Surg 1631202219220710.1016/j.jtcvs.2021.01.10033726912 · doi ↗ · pubmed ↗
- 3Kuźma J.Skorek P.Pitak M.Decompression of suprasystemic right ventricular pressure as palliative treatment for a child with tetralogy of Fallot Kardiol Pol 775201957857910.33963/KP.1484931125030 · doi ↗ · pubmed ↗