An Atypical Presentation of Pancreatitis Secondary to a Ventriculoperitoneal Shunt
Tasciana T Gordon, Katherine Goodall, Joanne Dale

TL;DR
A young woman developed acute pancreatitis due to a mispositioned ventriculoperitoneal shunt, highlighting an unusual complication requiring surgical intervention.
Contribution
This case report highlights an atypical and rare complication of VP shunt malposition causing acute pancreatitis.
Findings
A 23-year-old female presented with acute pancreatitis due to a malpositioned VP shunt in the lesser sac.
The condition was managed via laparoscopy, washout, and shunt externalisation.
This case underscores the need for high clinical suspicion in diagnosing VP shunt-related pancreatitis.
Abstract
Ventriculoperitoneal (VP) shunts are catheters inserted to drain excess cerebrospinal fluid (CSF) when there is an obstruction in the normal outflow or a decreased absorption of the fluid leading to hydrocephalus. Recognised complications of placement of the distal catheter are malposition, obstruction, pseudocysts and infection. Here, we present a case of a 23-year-old female with acute pancreatitis following the placement of a VP shunt in the lesser sac. The patient originally had a VP shunt placed in infancy for congenital hydrocephalus with one revision at four years old. She presented with a three-day history of worsening epigastric pain with an associated lipase of 3030 (10-60IU), CRP 157 (<5mg/L) and normal liver function tests. A CT scan showed acute pancreatitis with an associated collection within the lesser sac extending to the greater omentum. This was due to the malposition…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1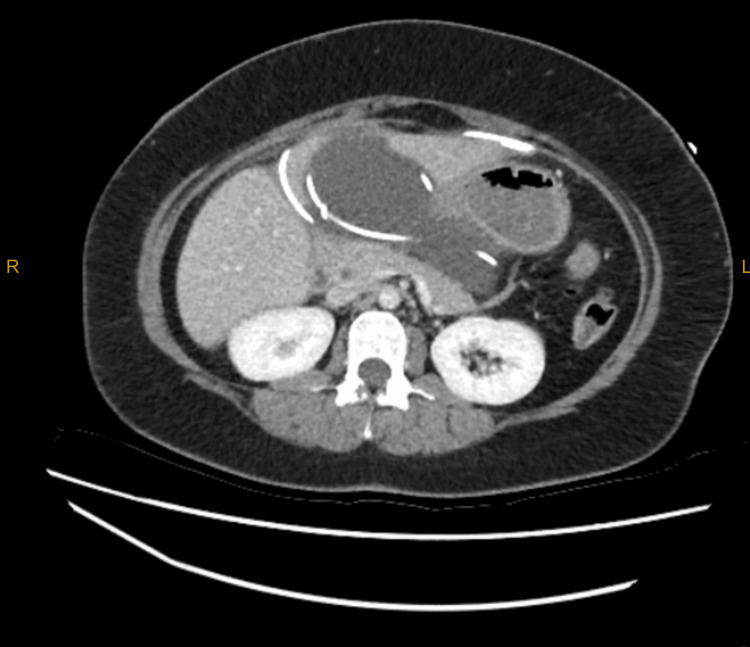 Figure 2
Figure 2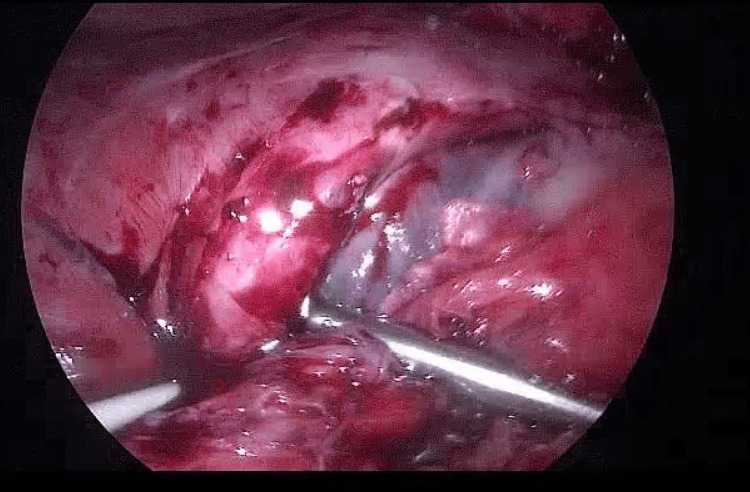 Figure 3
Figure 3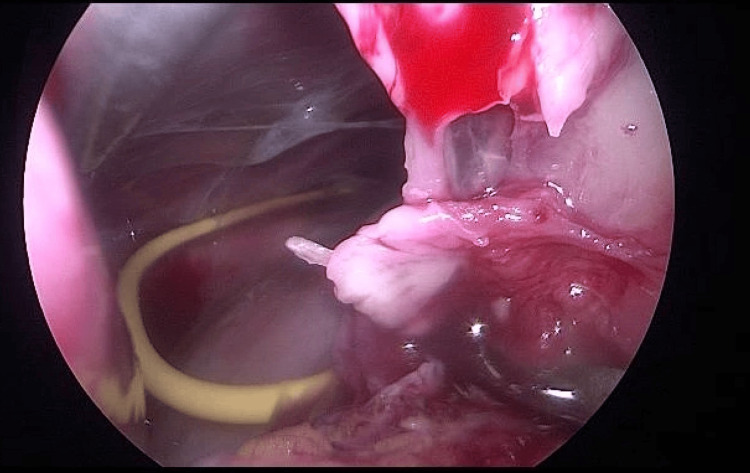 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Spinal Dysraphism and Malformations · Congenital Diaphragmatic Hernia Studies
Introduction
Pancreatitis is an inflammatory disorder of the pancreas. Common causes include gallstones, alcohol, hyperlipidaemia and autoimmune pancreatitis [1,2]. The diagnosis of pancreatitis is typically stipulated by the presence of two of the three following criteria: upper abdominal pain, elevated lipase (three or more times the upper limit of normal) and radiological findings consistent with pancreatitis [1,2]. Classification scores such as Ranson criteria are utilised to determine the severity of pancreatitis. Management may consist of fluid support in mild cases to surgical intervention with intensive care therapy in the more severe cases [2]. We present a 23-year-old female patient with an atypical presentation of mild pancreatitis secondary to a ventriculoperitoneal (VP) shunt.
Case presentation
A 23-year-old female patient presented to the emergency department with a three-day history of epigastric abdominal pain that was associated with nausea. She has a history of congenital hydrocephalus having a VP shunt placed in infancy and revised at age four for obstruction. She is currently breastfeeding, is a non-drinker, non-smoker and has a recent abdominal ultrasound (two months prior) showing no biliary calculi.
The patient has had multiple recent abdominal surgeries and has subsequently had VP shunt-related complications. She had a recent emergent caesarean section for foetal distress six months prior. She subsequently presented to the emergency department with a painful Richter’s hernia with an abdominal ultrasound showing the tip of the VP shunt tubing present within the hernia with extraperitoneal fluid tracking from this region into the lower anterior abdominal wall. This was managed with a laparoscopic reduction, washout and repair of the Richter’s hernia. A week later she re-presented with severe headaches, photophobia, nausea and vomiting with evidence of VP shunt obstruction. A stereotactic revision of the VP shunt was performed by neurosurgery. She had a right parietal skin incision adjacent to the valve catheter which confirmed the VP shunt obstruction. As the distal catheter was being removed it snapped and a decision was made to leave the remaining portion in situ with the tip draining into the lesser sac. A left subcostal incision was then made in a mini-laparotomy fashion to insert a new distal catheter which was tunnelled and secured to the existing valve before being placed in the general peritoneal cavity. She was subsequently discharged two days later and followed up in the outpatient clinic.
She presented acutely two months later. She was normotensive, tachycardic with a pulse rate of 106 beats per minute, respiratory rate of 20 breaths per minute and temperature of 37.9 degrees Celsius. She was orientated with a Glasgow Coma Scale 15 with no signs of VP obstruction. She had a soft abdomen but was guarding and tender in the epigastric and right upper quadrant. Her previous incisions had healed and there was no evidence of cellulitis.
Investigations showed a lipase 3030 (10-60U/L), CRP 157 (<5mg/L) and normal white cell count and liver function tests. CT abdomen showed a walled-off collection measuring approximately 136 mm x 108 mm x 56 mm containing the tips of both VP shunts. There was also some fat stranding neighbouring the pancreas parenchyma and a small volume of free fluid in the right iliac fossa, as seen in Figures 1, 2.
CT sagittal view showing collection within the lesser sac
CT abdomen showing catheter tips within the collection
She was managed by general surgery and neurosurgery with emergent laparoscopy. Findings included significant abdominal wall adhesions, and a bulging clear collection in the lesser sac where the new tip (yellow) and old tip (white) were found, as seen in Figures 3, 4.
Laparoscopic image of lesser sac collection
Laparoscopic image showing yellow catheter (new catheter) within the collection following aspiration
The old tip was surrounded by fibrin and obstructing the foramen of Winslow. The new tip appeared to have migrated into the lesser sac via the omentum and was sitting curled up in the lesser sac. It was externalised due to concerns of infection and the old tip was removed. The fluid was sent for lipase, CSF biochemistry as well as microscopy, culture and sensitivity. The infectious disease team was consulted and she was commenced on cephazolin whilst awaiting further biochemistry. The fluid culture showed no organisms and the CSF shows protein <0.1 (15-40mg/dL), glucose 3.8 (50-80mg/dL), leucocytes 5 (0-5), erythrocytes 5000 (0) and lipase of 75. It was concluded the fluid was CSF, and Corynebacterium sensitive to vancomycin was cultured from the old tip.
The VP shunt was internalised on day 8. This was a combined procedure as laparoscopic-assisted placement of the distal catheter. There were upper abdominal omental adhesions and fat saponification secondary to pancreatitis not seen at the initial laparoscopy. This was thought to be the sequelae of the underlying pancreatitis. The VP shunt tip was placed in the right lower quadrant. She was discharged with outpatient follow up which was unremarkable.
Discussion
VP shunts have become the standard in the management of hydrocephalus [3,4]. A shunt consists of a ventricular catheter that is connected to a valve and then connected to a distal catheter. The use of the peritoneal cavity as the location for CSF absorption was introduced by Kaush in 1908 [4,5]. Peritoneal placement is thought to be associated with reduced complications compared with ventriculoatrial and ventriculopleural shunts. The peritoneal approach has been described both as a mini-laparotomy or laparoscopic-assisted [6,7]. Pancreatitis is a rare complication of VP shunts and may be associated with the location of the distal catheter [3-5].
Methods of surgical technique described include using the falciform ligament to suspend the catheter directing it to the suprahepatic space or placing it in the general peritoneal cavity [6-8]. The most common complications described include malposition, infection, visceral perforation, shunt erosion of the skin, VP obstruction and pseudocyst formation [3-8]. Utilising the falciform technique has been shown to reduce the risk of malposition compared with general peritoneal placement [8].
In this case, there were two distal catheters in situ, both located in the lesser sac increasing the risk of complication. We hypothesise that the new catheter migrating into the lesser sac resulted in pseudocyst formation abutting the body of the pancreas causing trauma and pressure. Leading to inflammation of the pancreas and presentation of acute pancreatitis. The old distal catheter tip may have contributed to this process by trauma to the pancreas after being snapped in the removal process and obstructing the foramen of Winslow with the catheter.
At the time of the presentation, the radiological findings raised concern about an infectious collection. There was concern this was from the VP shunt rather than the pancreas. The literature supports the externalisation of the shunt in shunt-related intra-abdominal infections. However, there is much debate with regard to the externalisation of non-shunt-related abdominal or pelvic infections [9]. Some publications have stated that there was no statistical evidence of a reduction in chronic peritonitis if the shunt remained in situ. Given the fluid culture had shown no organisms it is important to assess this at the time of laparoscopy to potentially avoid a further operation.
Conclusions
The location of the distal VP catheter needs to be considered when placing a VP shunt for hydrocephalus. Pancreatitis is a complication if the VP shunt catheter migrates as demonstrated by this case. Management is dependent on the symptoms, presence of infection and severity of the pancreatitis. The anatomical consideration of the course of the intra abdominal portion of the VP shunt should be considered. This case also demonstrates the collegial nature of collaborative care between two surgical specialities to improve patient outcomes successfully. Adoption of laparoscopic assisted placement of the distal catheter may be beneficial and this should be considered when assessing the patient prior to the initial VP shunt placement or revision surgery.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Acute pancreatitis: diagnosis and treatment Drugs Szatmary P Grammatikopoulos T Cai W 12511276822022 https://link.springer.com/article/10.1007/s 40265-022-01766-43607432210.1007/s 40265-022-01766-4PMC 9454414 · doi ↗ · pubmed ↗
- 2Significant elevations of serum lipase not caused by pancreatitis: a systematic review HPB (Oxford) Hameed AM Lam VW Pleass HC 99112172014 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 4299384/2488839310.1111/hpb.12277 PMC 4299384 · doi ↗ · pubmed ↗
- 3Ventriculoperitoneal shunt In: Stat Pearls [Internet] Fowler JB De Jesus O Mesfin FB Treasure Island, FL Stat Pearls Publishinghttps://www.ncbi.nlm.nih.gov/books/NBK 459351/2024 https://www.ncbi.nlm.nih.gov/books/NBK 459351/29083724 · pubmed ↗
- 4Risk factors associated with distal catheter migration following ventriculoperitoneal shunt placement J Clin Neurosci Abode-Iyamah KO Khanna R Rasmussen ZD Flouty O Dahdaleh NS Greenlee J Howard MA 3rd 46492520162654967410.1016/j.jocn.2015.07.022PMC 6262820 · doi ↗ · pubmed ↗
- 5Abdominal complications related to ventriculoperitoneal shunt placement: a comprehensive review of literature Cureus Ferreira Furtado LM Da Costa Val Filho JA Moreira Faleiro R Lima Vieira JA Dantas Dos Santos AK 013202110.7759/cureus.13230 PMC 787725733585146 · doi ↗ · pubmed ↗
- 6Laparoscopic-assisted distal ventriculoperitoneal shunt placement Surg Neurol Khosrovi H Kaufamn HH Hrabovsky E 127135491998 https://www.sciencedirect.com/sdfe/pdf/download/eid/1-s 2.0-S 0090301997003571/first-page-pdf 945726110.1016/s 0090-3019(97)00357-1 · doi ↗ · pubmed ↗
- 7Laparoscopically assisted ventriculoperitoneal shunt placement: a prospective randomized controlled trial J Neurosurg Schucht P Banz V Trochsler M 1058106712220152553423110.3171/2014.9.JNS 132791 · doi ↗ · pubmed ↗
- 8Suprahepatic space as an alternative site for distal catheter insertion in pseudocyst-associated ventriculoperitoneal shunt malfunction J Neurosurg Habibi Z Golpayegani M Ashjaei B 247254262020 https://thejns.org/pediatrics/view/journals/j-neurosurg-pediatr/26/3/article-p 247.xml 10.3171/2020.3.PEDS 1977232413860 · doi ↗ · pubmed ↗