Bronchiectasis in renal transplant patients: a cross-sectional study
Pauline Mulette, Jeanne-Marie Perotin, Anaëlle Muggeo, Thomas Guillard, Audrey Brisebarre, Hélène Meyer, Jean Hagenburg, Julien Ancel, Valérian Dormoy, Vincent Vuiblet, Claire Launois, François Lebargy, Gaëtan Deslee, Sandra Dury

TL;DR
This study compares bronchiectasis in kidney transplant patients and those with idiopathic bronchiectasis, finding similar clinical and microbiological features.
Contribution
The study is the first prospective comparison of bronchiectasis in renal transplant patients and idiopathic cases.
Findings
RT-B and IB groups showed similar dyspnea, exacerbations, and pulmonary function.
Chronic cough was less frequent in RT-B patients compared to IB patients.
Airway microbiota prevalence and diversity were similar between the two groups.
Abstract
Bronchiectasis is a chronic airway disease characterized by permanent and irreversible abnormal dilatation of bronchi. Several studies have reported the development of bronchiectasis after renal transplantation (RT), but no prospective study specifically assessed bronchiectasis in this population. This study aimed to compare features of patients with bronchiectasis associated with RT to those with idiopathic bronchiectasis. Nineteen patients with bronchiectasis associated with RT (RT-B group) and 23 patients with idiopathic bronchiectasis (IB group) were prospectively included in this monocentric cross-sectional study. All patients underwent clinical, functional, laboratory, and CT scan assessments. Sputum was collected from 25 patients (n = 11 with RT-B and n = 14 with IB) and airway microbiota was analyzed using an extended microbiological culture. Dyspnea (≥ 2 on mMRC scale),…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
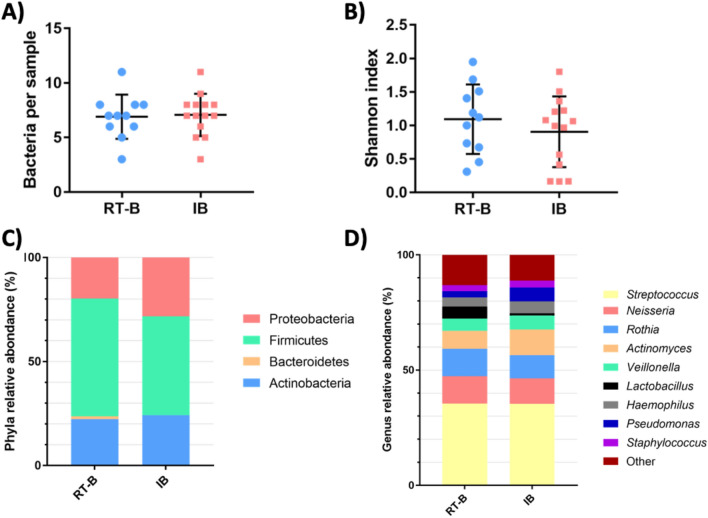 Figure 1
Figure 1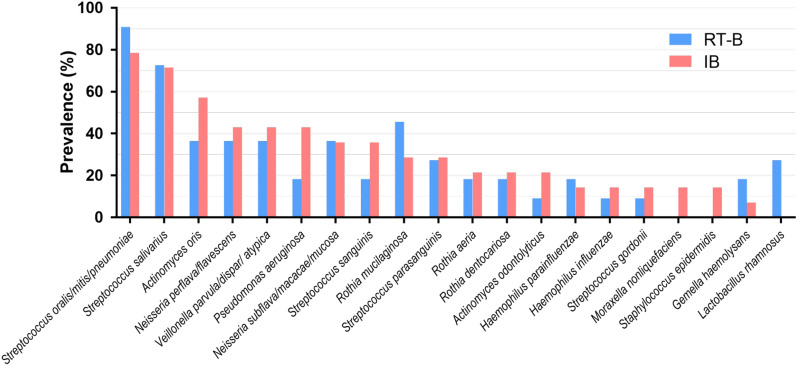 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCystic Fibrosis Research Advances · Tracheal and airway disorders · Dysphagia Assessment and Management
Background
Non-cystic fibrosis (non-CF) bronchiectasis is a chronic airway disease characterized by permanent and irreversible abnormal dilatation of bronchi [1]. The main causes of bronchiectasis are post-infectious, immunodeficiency, chronic obstructive pulmonary disease, connective tissue disease, ciliary dysfunction, and allergic bronchopulmonary aspergillosis. However, despite extensive etiologic investigations, bronchiectasis remains considered idiopathic in 45% of the cases [2, 3]. The most common symptoms of bronchiectasis are cough, sputum, dyspnea, and fatigue [4] which are associated with impaired quality of life [5–7] and frequent exacerbation [8]. The airways of non-CF bronchiectasis are predisposed to microbial colonization and increased risk of chronic infection [9]. At a stable state, the most common bacteria are Haemophilus influenzae and Pseudomonas aeruginosa [10–12].
Several studies have previously reported the development of bronchiectasis after renal transplantation (RT) in children and adults [13–16]. Recently, we conducted a multicenter retrospective study describing the clinical, functional, radiological and microbiological characteristics of 46 patients with bronchiectasis revealed after RT [17]. This study identified frequent symptoms of chronic cough and sputum, frequent airway infections with H. influenzae, and a mean time of 11 years between RT and the diagnosis of bronchiectasis. The pathophysiology of bronchiectasis associated with RT is not yet elucidated. It may involve hypogammaglobulinemia induced by immunosuppressive drugs, a potential direct effect of mycophenolic acid, and/or predisposing factors associated with the underlying renal disease especially autosomal dominant polycystic kidney disease (ADPKD) [17]. Although RT is the most common form of solid organ transplantation, no prospective study specifically assessed bronchiectasis in this population. Moreover, no study compared the clinical features of bronchiectasis associated with RT (RT-B) to idiopathic bronchiectasis (IB) in terms of respiratory symptoms, pulmonary function, quality of life, and airway microbiota.
This study aimed to compare the clinical features of RT-B patients to those with IB. In addition, we compared the viable airway microbiota at a stable state between RT-B and IB patients.
Methods
Study population
This prospective cross-sectional monocenter study was conducted in the Department of Respiratory Diseases at Reims University Hospital (France) from November 2016 to December 2019. Patients were included in the cohort for research and innovation in inflammatory respiratory diseases (Recherche et INNOvation en PAthologie Respiratoire Inflammatoire: RINNOPARI). This study was approved by the ethics committee (Comité de Protection des Personnes—Dijon EST I, No. 2016-A00242-49) and registered in clinicaltrials.gov (NCT02924818). The authorization to access patient data was obtained from the French Advisory Committee for Data Processing in Health Research (CCTIRS, Comité Consultatif sur le Traitement de l’Information en matière de Recherche dans le domaine de la Santé) (no. 13.018) and approved by the national commission for the personal data protection (CNIL, Comité National de l’Informatique et des Libertés) (no. 913412). Data were fully anonymized. Each patient signed written informed consent.
Patients were consecutively included if they were at least 18 years old and matched to one of the two groups: (1) patients with RT and bronchiectasis (RT-B group) or (2) patients without RT and with bronchiectasis considered as idiopathic (IB group). Causative diseases of bronchiectasis including cystic fibrosis, common variable immunodeficiency, allergic bronchopulmonary aspergillosis, asthma, alpha-1-antitrypsin deficiency, chronic obstructive pulmonary disease, rheumatoid arthritis, inflammatory bowel disease, or mycobacterial lung infection sequelae were considered as exclusion criteria [1, 18]. Patients were also excluded if the respiratory disease was not at a stable state defined by the absence of airway infection requiring antibiotics in the last month.
Data collection
Demographic, clinical, functional (pulmonary function tests, 6-min walking test, arterial blood gas), laboratory, and microbiological data and thoracic computed tomography (CT)-scan results were recorded in a standardized format. Symptoms and quality of life scores were evaluated using four scales: the Cough And Sputum Assessment Questionnaire (CASA-Q) [19], the Hospital Anxiety and Depression Scale (HAD) [20, 21], the St George’s Respiratory Questionnaire (SGRQ) [22, 23], and the Medical Outcome Study Short Form 36 health survey (MOS SF-36) [24, 25].
Measurement of full blood count, serum creatinine, level of total immunoglobulins (Ig), and dosage of immunosuppressive drugs for RT-B group were performed.
According to the international consensus, an exacerbation was defined by an impairment of at least 3 or more baseline symptoms (cough, sputum volume or purulence, breathlessness, fatigue, malaise, hemoptysis) for at least 48 h and requiring a change in treatment [26].
The severity and prognosis of bronchiectasis were evaluated according to two multidimensional grading systems: the FACED [27] and the E-FACED score [28].
CT scans
Each CT scan was reviewed by two pulmonologists (SD, GD) with a final consensus interpretation. All CT scans were performed with the patient in the supine position at end-inspiratory volume using multidetector CT scanners. One- to 5-mm-thick slices at 5- to 10-mm intervals were analyzed from the lung apices to the lung bases. The diagnosis of bronchiectasis was defined according to the Fleischner Society as dilated bronchial lumen relative to the adjacent pulmonary artery, absence of bronchial tapering, and visualization of bronchi within 1 cm of the pleural surface [29]. The extent of bronchiectasis, the thickness of the bronchial wall, and small airways abnormalities were quantified for each lobe (lingula was considered as a separated lobe) according to the Ooi score [30].
Microbiology
Sputum samples were collected after patients rinsed their mouths out with sterile water. If spontaneous sputum was not possible, induced sputum was systematically performed according to international recommendations [31, 32].
Extended culture analysis was performed on the sputum. After liquefaction by N-acetylcysteine, serial dilutions (1/1000, 1/10,000, and 1/100,000) were made and cultured in Columbia blood agar, chocolate agar, Schaedler agar, and Pseudomonas selective cetrimide agar (Thermo Fisher Scientific, USA), at 37 °C for 48 h for aerobic and 5% CO_2_ cultures and 5 days for anaerobic cultures. All colonies that appeared to be morphologically distinct were quantified as colony-forming unit (CFU) per milliliter and identified by matrix-associated laser desorption ionization-time of flight (MALDI-TOF) mass spectrometry (MALDI Biotyper®, Bruker Daltonics, Bremen, Germany). The α-diversity of the airway microbiota was evaluated with the Shannon index (a marker of intra-individual diversity).
Chronic P. aeruginosa infection was defined by the isolation of P. aeruginosa in two or more cultures, at least 3 months apart in a consecutive period of 12 months at a stable state [33].
Statistical analysis
Statistical analysis was performed using SPSS software (version 26). Data are expressed as mean (standard deviation) or median (25th or 75th percentiles) depending on data distribution for quantitative variables and as numbers (%) for qualitative variables. Comparisons were performed using Chi^2^ or fisher’s exact test for qualitative variables and Student’s t-test for quantitative variables. A p value < 0.05 was considered significant.
Results
Patients characteristics
Clinical characteristics of the 42 patients anlayzed are shown in Table 1. Among 44 patients included, two patients were excluded from the IB group because of underlying causes (rheumatoid arthritis n = 1, alpha-1 antitrypsin deficiency n = 1). Data were analyzed for 19 patients in the RT-B group and 23 patients in the IB group. RT-B and IB groups were similar in terms of age, sex ratio, body mass index (BMI), and smoking history. Dyspnea (≥ 2 on modified Medical Research Council scale (mMRC)), hemoptysis, and number of exacerbations were similar in the RT-B and IB groups. By contrast, the chronic cough was more frequent in the IB group when compared with the RT-B group. The median interval between first RT and first respiratory symptoms and between first RT and diagnosis of bronchiectasis was 11 (1–20) and 12 (2–18) years, respectively. Most RT-B patients (79%) had undergone only one renal transplantation.Table 1. Clinical characteristicsRT-Bn = 19IBn = 23P valueMale12 (63)11 (48)0.320Age, years66 (57–69)62 (48–70)0.147Smoker (current or former)12 (63)9 (39)0.121 Pack-years26 (14–30)10 (7–25)0.652Clinical features BMI, kg/m^2^25 (23–30)23 (21–26)0.144 Chronic cough13 (68)22 (96)0.034 Dyspnea mMRC ≥ 2^a^8 (53)9 (39)0.768 Hemoptysis0 (0)2 (9)0.215Respiratory tract infections Exacerbation in the past year12 (63)19 (83)0.637 Number of episodes per patient1 (0–2)1 (1–3)0.551 Hospitalization for exacerbation in the past year6 (32)1 (4)0.189Cause of end-stage renal disease Chronic glomerulonephritis4 (21)NA Diabetic nephropathy2 (11)NA Autosomal dominant polycystic kidney disease6 (32)NA Chronic tubulointerstitial nephritis2 (11)NA Unknown cause of end-stage renal disease3 (16)NA Other renal^b^2 (11)NAImmunosuppressive drugs Mycophenolate mofetil14 (74)NA Cyclosporine8 (42)NA Tacrolimus7 (37)NA Azathioprine2 (11)NA Oral corticosteroids5 (26)NAAntibiotic therapy in the last 6 months12 (63)15 (65)1.000Interval between first RT and first symptoms, years^c^11 (1–20)NAInterval between first RT and diagnosis of bronchiectasis, years^c^12 (2–18)NAData are expressed as median (25th or 75th percentiles) and as number (percentage). p-value < 0.05 are considered as significant and highlighted in bold BMI body mass index, IB patients with idiopathic bronchiectasis, mMRC modified Medical Research Council, NA not applicable, RT-B patients with renal transplantation and bronchiectasis^a^Missing data for 4 patients in RT-B group^b^Dysplastic kidney disease (malformation of the kidney)^c^One patient exhibited bronchiectasis before transplantation
Functional characteristics and radiological data are shown in Table 2. There was no difference between the RT-B and IB groups regarding pulmonary function tests, 6-min walking test and arterial blood gas. The total bronchiectasis score was similar in the RT-B and IB groups except for the middle lobe exhibiting a higher bronchiectasis score in the IB group than in the RT-B group [4 (1–4) vs. 2 (1–3); p = 0.038].Table 2. Functional characteristics and CT scan dataRT-Bn = 19IBn = 23P valuePulmonary function tests FEV_1_, %85 ± 2580 ± 270.593 FVC, %90 ± 2188 ± 220.758 FEV_1_/FVC < 0.706 (32)6 (26)0.694 RV, %135 ± 27138 ± 540.794 TLC, %103 ± 14103 ± 140.949 DLCO, %59 ± 1664 ± 190.3936-min walking test (room air)^a^ SpO_2_ min, %94 ± 493 ± 50.900 Distance, m390 ± 99459 ± 1040.067Arterial blood gas (room air)^b^ PaO_2_, mmHg82 ± 1581 ± 160.883Bronchiectasis score^c,d^ Total score16 (6–22)17 (10–28)0.169Data are expressed as mean (± standard deviation), median (25th or 75th percentiles) and number (percentage).DLCO diffusing capacity of the lungs for carbon monoxide, FEV1 forced expiratory volume in 1 s, FVC forced vital capacity, IB patients with idiopathic bronchiectasis, PaO2 partial pressure of oxygen, RT-B patients with renal transplantation and bronchiectasis, RV residual volume, SpO2 pulse oxygen saturation, TLC total lung volume^a^Missing data for 7 patients in IB group^b^Missing data for 7 patients in RT-B group and 5 patients in IB group^c^Missing data for 2 patients in IB group^d^According to the Ooi score [30]
Symptoms or prognostic scores and quality of life scales are shown in Table 3. The severity scores (FACED and E-FACED) were similar in the RT-B and IB groups. Regarding the quality of life, the SGRQ total score was similar between the RT-B group and the IB group. There was no significant difference between the RT-B and IB groups in domains of the MOS SF-36 questionnaire. By contrast, cough on the CASA-Q score was more impaired in the IB group compared with the RT-B group.Table 3. Symptoms scores and quality of life scalesRT-Bn = 19IBn = 23P valueSeverity score FACED^a^2 (1–3)2 (1–3)1.000 E-FACED^b^2 (0–3)3 (1–4)0.200Symptoms score CASA-Q Cough symptom75 (50–100)42 (17–58)0.0004 Cough impact82 (56–100)50 (25–81)0.019 Sputum symptom75 (50–100)50 (33–67)0.008 Sputum impact88 (71–100)75 (38–83)0.012 HAD Anxiety (mean)7 (3–10)7 (3–10)0.902 Depression (mean)6 (2–7)6 (2–8)0.805Quality of life scales SGRQ Total score38 (1–58)38 (22–61)0.219 MOS SF-36 Global physical score36 (24–43)36 (24–50)0.745 Global mental score27 (5–47)28 (16–44)0.244Data are expressed as median (25th or 75th percentiles). p-value < 0.05 are considered as significant and highlighted in boldIB patients with idiopathic bronchiectasis, RT-B patients with renal transplantation and bronchiectasisCASA-Q: Cough And Sputum Assessment Questionnaire score assessing impact of cough and sputum production on daily activities, ranging from 0 to 100, with the highest score corresponding to a better quality of life; HAD: Hospital Anxiety and Depression Scale (HAD: a score between 0 and 7 for anxiety or depression domain meant no trouble, 8–10 suspected troubles, 11–21 confirmed trouble; SGQR: St George’s respiratory questionnaire (SGRQ) assessing symptoms and impact on daily activities with a score ranging from 0 to 100, that indicates the maximum impairment of quality of life; MOS SF-36: Medical Outcome Study Short Form 36 health survey, a multidimensional generic scale evaluating health status regardless of causal disease, sex, age, and treatment. A Physical Composite Score and a Mental Composite Score was calculated. A score of 100 indicates no impairment of quality of life [24]^a^FACED score incorporates five variables: forced expiratory volume in 1 s (FEV_1_) % predicted, age, chronic colonization by P. aeruginosa, extension of bronchiectasis by radiological assessment, and dyspnea^b^E-FACED score also includes the occurrence of exacerbations in the previous year
Laboratory data
The frequency of lymphopenia and hypogammaglobulinemia was not different in the RT-B group compared to the IB group. Dosage of immunosuppressive drugs was within the therapeutic targets in all patients in the RT-B group. As expected, estimated glomerular filtration rate was more impaired in the RT-B group than in the IB group. IgG4 level was lower in the RT-B group compared to the IB group [0.2 (0.0–0.4) vs. 0.7 (0.2–1.1), p = 0.032] (Additional file 1: Table S1).
Microbiological data
We determined the viable airway microbiota of 25 sputa (11 for RT-B patients and 14 for IB patients). In the RT-B group, we obtained 34 different species with a mean of 6.9 species per sample. In the IB group, we obtained 33 different species with a mean of 7.1 species per sample (Fig. 1A). Assessment of α-diversity revealed no significant differences between the 2 groups (Fig. 1B). A small and non-significant increase of firmicutes and depletion of proteobacteria were observed in the RT-B group (respectively, p = 0.23 and p = 0.15) (Fig. 1C). The different genera found showed a similar repartition in the two groups, with a predominance of the Streptococcus, Neisseria, and Rothia (Fig. 1D).Fig. 1. Bacterial diversity of airway microbiota in RT-B and IB patients. A Number of bacteria per sample. B Alpha diversity (Shannon index). Relative abundance on the phyla level (C) and genus level (D)
We next compared the prevalence of the different species of the microbiota in both RT-B and IB groups (Fig. 2). Two Streptococci, S. oralis/mitis/pneumoniae and S. salivarius, were the most common bacteria, being found in more than 60% of the patients. Although not statistically significant, Lactobacillus rhamnosus was more common in RT-B patients than in IB patients (27% in the RT group vs. 0% in the IB group, p = 0.072). We also found some pathogenic bacteria at a stable state in this cohort including P. aeruginosa, H. influenzae, and S. aureus (Additional file 1: Table S2).We observed a trend with less P. aeruginosa in the RT-B group than in the IB group (18.2 vs 42.9%, p = 0.19), and all patients exhibiting L. rhamnosus in the RT-B group did not co-carry *P. aeruginosa.*Fig. 2. Prevalence of the main bacteria in airway microbiota in RT-B and IB patient sputa. Isolates with less than 10% frequency are not listed. IB patients with idiopathic bronchiectasis, RT-B patients with renal transplantation and bronchiectasis
Bacterial quantifications ranged from 1 × 10^2^ to 1 × 10^9^, with a median at 1 × 10^5^ and no difference between the two groups of patients. The quantification of the three pathogens P. aeruginosa, H. influenzae, and S. aureus were all higher than this global median, from 1 × 10^6^ to 1 × 10^8^.
Discussion
This prospective cross-sectional study allowed us to characterize the features of patients with bronchiectasis associated with RT and to compare these features to patients with IB. This study demonstrates that RT-B patients share many clinical features with IB patients including chronic respiratory symptoms, exacerbations, and impaired quality of life. At a stable state, the microbiota of IB and RT-B groups are nearly similar in terms of richness, diversity, and prevalence of different phyla and genera, except for a higher prevalence of L. rhamnosus in RT-B patients.
Chronic cough was frequent in RT-B patients (68%) but lower than in IB patients. By contrast, patients with RT-B had similar symptoms of dyspnea and rate of exacerbation per year. Interestingly, the incidence and number of exacerbations in the past year were similar in the RT-B group (63% of patients, median of 1.0 exacerbation per patient) and the IB group (83% of patients, median of 1.0 exacerbation per patient). In a prospective cohort including 608 patients with non-CF bronchiectasis, only 21% of patients had at least one exacerbation in the past year [34], suggesting that our IB group might be more severe due to a selection bias of IB patients followed up in a tertiary university hospital. In both groups, the pulmonary functional impact was limited with mild impairment of forced expiratory volume in 1 s (FEV_1_), consistent with another prospective study including patients with IB showing a mean FEV_1_ of 78% [35]. In our study, the diffusion capacity of carbon monoxide (DLCO) was impaired in 68% (RT-B) and 61% (IB) of the patients, with a mean DLCO between 59 and 64%, respectively. Comparison with literature is limited by few data available regarding DLCO in bronchiectasis. In a study assessing DLCO in non-CF bronchiectasis, 56% of patients had a reduction in DLCO [36]. King et al. reported a mean DLCO value of 88 ± 21%, with a rate of 23% of current or former smokers [37]. The lower DLCO value in our study may be related to a higher rate of current or former smokers in both groups (63% in the RT-B group, 39% in the IB group). Interestingly, the mean DLCO value in RT patients without bronchiectasis was normal in previous studies ranging from 83% [38] to 84% [39]. Regarding CT scan, the bronchiectasis score was similar between the IB and RT-B groups (15 and 20, respectively) assessed by the Ooi et al. score [40].
In our study, FACED and E-FACED scores were similar in RT-B and IB groups, suggesting a similar severity and prognosis despite immunosuppression in the RT group. Of note, there was a trend of lymphopenia in the RT-B group compared to the IB group. The most common causes of mortality in RT patients are cardiovascular disease, followed by cancer and infections (mainly urinary tract and lung infections) [41, 42]. In RT patients, the incidence of pulmonary infection was 8.8% [43]. However, no information regarding thoracic CT scan characteristics including the presence of bronchiectasis was available in these studies. The quality of life in RT patients is associated with general health assessment, physical functioning, pain, sleep quality, occupational status, vitality, social activity, staff support, and quality of care [44]. Mean values of MOS SF-36 global physical and mental scores in RT-B patients seemed more impaired than previously reported in RT patients [45]. However, quality of life was overall similar between RT-B and IB in our study.
Few microbiological data on RT-B patients are available and are limited to case reports [14, 15] and one retrospective study [17]. In this study, we described for the first time the airway viable microbiota of patients with RT-B at a clinically stable state using an extended-quantitative bacterial culture of sputum samples with detection and identification of isolated bacteria. We found that the microbiota was globally similar between RT-B and IB groups. We described the same richness, diversity, and prevalence of the different phyla and genera, with a predominance of the Streptococci, Neisseria, Rothia, and Veillonella, as usually described in the airway microbiota in bronchiectasis [9, 45, 46]. Some pathogenic bacteria were detected as part of the microbiota such as P. aeruginosa, H. influenzae, and S. aureus, as reported in other studies from non-CF bronchiectasis patients in Europe [34, 46–48].
The prevalence of all the different bacteria was similar in the 2 groups. Although not statistically significant, probably due to the low number of samples, we found that L. rhamnosus was more common in RT-B patients compared to IB patients (27% vs. 0%) and that P. aeruginosa was less common in the RT-B group than in the IB group (18% vs. 43%). We also noticed that the patients with L. rhamnosus did not co-carry P. aeruginosa. This inverse correlation may suggest a protective effect of L. rhamnosus, a known probiotic agent, on the carriage of P. aeruginosa in airway microbiota. Indeed, there is a growing interest in the potential use of Lactobacilli probiotics, notably L. rhamnosus, as clinical studies showed the prevention of pneumonia after oral or respiratory administration [49–52]. Many studies also described the abilities of Lactobacilli to specifically protect against P. aeruginosa infections in murine models of pneumonia [53–55]. Further studies, with an increased number of patients, are needed to confirm this potential protective effect of Lactobacilli in bronchiectasis.
There are several limitations to our study. First, it was a monocenter study with a small sample size with a potential selection of more severe IB patients. Second, the small number of patients did not allow us to investigate the potential role of ADPKD as a risk factor of bronchiectasis as previously suggested [56, 57]. However, in our study, the main underlying renal disease in RT-B patients was also ADPKD (n = 6, 32%). Third, this study was conducted at a stable state. Some patients were therefore not able to produce sputum and were not included in the microbiological analyzes. Fourth, we did not use the Bronchiectasis Health Questionnaire, which has been developed and validated specifically for patients with bronchiectasis, but was not available when our study started [58]. Finally, the cross-sectional design does not provide information regarding the evolution of the clinical, functional, CT scan, and microbiological features of RT-B over time which would require longitudinal studies with long-term follow-up.
Conclusion
This cross-sectional study showed that RT-B patients share many clinical features with IB patients including chronic respiratory symptoms, exacerbations, pulmonary function, and quality of life impairment. At a stable state, the microbiota of IB and RT-B groups are nearly similar in terms of richness, diversity, and prevalence of different phyla and genera. These results highlight that bronchiectasis should be considered in RT patients exhibiting chronic respiratory symptoms and/or exacerbation. We hope these results will stimulate to conduct further larger longitudinal studies to better characterize the mechanisms of RT-B including monitoring of airway microbiota in RT, its incidence, and potential impact on therapeutic management.
Supplementary Information
Additional file 1: Table S1. Laboratory data.Additional file 2: Table S2. Prevalence and quantification of the bacteria in airway microbiota in RT-B and IB patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Polverino E Pieter C Mc Donell MJ Aliberti S Marshall SE Loebinger MR Murris M Canton R Torres A Dimakou K De Soriza A Hill AT Hawortj CS Vendrell M Ringshausen FC Subotic D Wilson R European Respiratory Society guidelines for the management of adult bronchiectasis Eur Respir J 2017503170062910.1183/13993003.00629-201728889110 · doi ↗ · pubmed ↗
- 2Gao YH Guan WJ Liu SX Wang L Cui JJ Chen RC Zhang GJ Aetiology of bronchiectasis in adults: a systematic literature review Respirology 20162181376138310.1111/resp.1283227321896 · doi ↗ · pubmed ↗
- 3Flume PA Chalmers JD Olivier KN Advances in bronchiectasis: endotyping, genetics, microbiome and disease heterogeneity Lancet 20183921015088089010.1016/S 0140-6736(18)31767-730215383 PMC 6173801 · doi ↗ · pubmed ↗
- 4Saadi Imam J Duarte AG Non-CF bronchiectasis: orphan disease no longer Respir Med 202016610594010.1016/j.rmed.2020.10594032250872 · doi ↗ · pubmed ↗
- 5Martinez-Garcia MA Perpina-Tordera M Roman-Sanchez P Soler-Cataluna JJ Quality-of-life determinants in patients with clinically stable bronchiectasis Chest 2005128273974510.1378/chest.128.2.73916100162 · doi ↗ · pubmed ↗
- 6Terpstra LC Biesenbeek S Altenburg J Boersma WG Aetiology and disease severity are among the determinants of quality of life in bronchiectasis Clin Respir J 201913852152910.1111/crj.1305431295770 · doi ↗ · pubmed ↗
- 7Wilson CB Jones PWO'Leary CJ Hansell DM Cole PJ Wilson R Effect of sputum bacteriology on the quality of life of patients with bronchiectasis Eur Respir J 1997101754176010.1183/09031936.97.100817549272915 · doi ↗ · pubmed ↗
- 8Chalmers JD Aliberti S Filonenko A Shteinberg M Goemine PC Hill AT Fardon TC Obradovic D Mc Donell MJ Characterization of the “frequent exacerbator phenotype” in bronchiectasis Am J Respir Crit Care Med 2018197111410142010.1164/rccm.201711-2202 OC 29357265 · doi ↗ · pubmed ↗