Retrograde Migration of a Percutaneous Endoscopic Gastro-Jejunal Tube Into the Esophagus
Binyamin R Abramowitz, Jude Noel, Sushil Ahlawat

TL;DR
A rare case of a gastro-jejunal tube moving into the esophagus is reported, highlighting a rare complication of a common medical procedure.
Contribution
The paper documents an extremely rare case of PEG-J tube migration into the esophagus.
Findings
A patient's PEG-J tube migrated retrogradely into the esophagus.
This case highlights the potential for tube migration as a rare complication of PEG-J procedures.
Abstract
Percutaneous endoscopic gastrostomy (PEG) and percutaneous endoscopic gastro-jejunal (PEG-J) tube placement are both common procedures regularly performed on patients requiring nutritional support. These procedures may be complicated by infection, hemorrhage, fistulization, or tube migration. We present an extremely rare case of a patient with a PEG-J tube that migrated into the esophagus.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1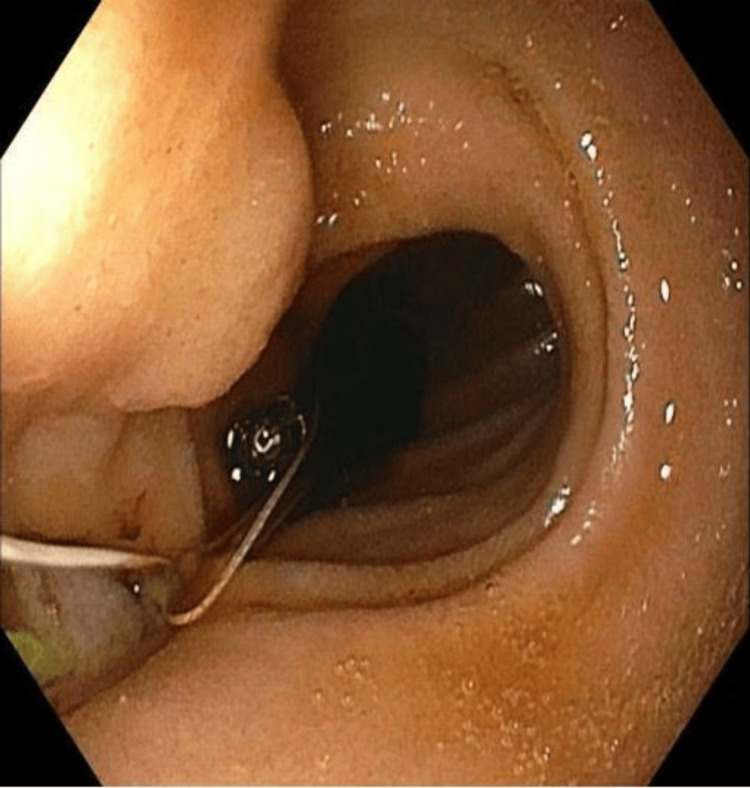 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsClinical Nutrition and Gastroenterology · Child Nutrition and Feeding Issues · Dysphagia Assessment and Management
Introduction
Percutaneous endoscopic gastrostomy (PEG) and percutaneous endoscopic gastro-jejunal (PEG-J) tube placement are commonly performed on patients requiring long-term enteral nutritional support. Due to underlying pathology, these patients have a mismatch between their oral caloric intake and their overall metabolic demands [1]. Pathological disease processes causing this mismatch include stroke, dementia, motor neuron disease, gastrointestinal malignancies, and prolonged coma [2,3]. However, the progressively worsening clinical courses of these pathologies are not the sole determining factor as to whether PEG or PEG-J tube placement is indicated. Rather, detailed discussions about the goals of care are required. These discussions aim to elucidate the prognosis, priorities, and realistic expectations of the patient before finalizing the decision on whether tube feeding is indicated [4].
While PEG tubes are inserted through the abdominal wall to deliver feeds directly into the stomach, PEG-J tubes are inserted similarly but with an extension leading into the jejunum so that feeds bypass the stomach itself and are directed into the small bowel. Although PEG tubes are more common, patients may still be at high risk for aspirating gastric feeds, especially in conditions such as gastric outlet obstruction, gastroparesis, and gastric resection [5,6]. In many of these patients, PEG-J tubes may be a better option, as feeds are delivered more distally into the jejunum, thereby reducing the risk of aspiration [7]. The placement of a PEG-J tube is uncommonly complicated by tube migration, which can lead to infection, hemorrhage, fistulization, buried bumper syndrome, or aspiration pneumonia [8,9]. We present a unique case of a PEG-J tube that was found to have migrated into a patient’s mid-esophagus.
Case presentation
A 29-year-old female with a past medical history of sickle cell disease, cerebral palsy, and cerebral vascular accident status post-PEG-J tube placement presented with her PEG-J tube clogged since the previous day. The PEG-J tube had last been replaced only four months earlier. Although the patient was non-verbal at baseline, she appeared comfortable and not in any acute distress. Her mother reported no vomiting, fever, or chills, and no aberrant behavior from the patient’s baseline. She was hemodynamically stable: blood pressure of 112/78, heart rate of 92 beats per minute, respiratory rate of 18 breaths per minute, temperature of 98.0˚F, and oxygen saturation at 98% on room air. Of note, she had recently been discharged from a three-month-long hospitalization for sepsis secondary to pneumonia complicated by pulmonary embolism treated with both antibiotics and full-dose anticoagulation.
On physical examination, the patient’s lungs were clear to auscultation bilaterally with no wheezes or crackles, and her abdomen was soft and non-tender. The PEG-J tube site appeared clean, non-erythematous, and with the tube properly in place. Laboratory data showed a white blood cell count of 9.74 K/uL, hemoglobin of 9.9 g/dL, platelets of 186 K/uL, and all electrolytes as well as renal function within normal limits. The chest X-ray was largely unremarkable, though it was noted to be a limited study due to the non-ideal positioning of the patient. Although the PEG-J tube site appeared clean, the balloon lumen appeared to be hyperinflated, and both the jejunal as well as the gastric ports could not be flushed properly, as every flush attempt resulted in saline pouring right back out of the tube. Attempts to unclog the tube with ginger ale were unsuccessful.
The gastroenterology service was consulted, and after further unsuccessful attempts to unclog the tube, esophagogastroduodenoscopy (EGD) was subsequently performed for tube replacement. During the procedure, the distal tip of the PEG-J tube was visualized to be within the mid-esophagus (Figure 1). Following balloon deflation, the tube was removed. Using the prior tube tract, a new 24-French gastrostomy (G) tube was placed, utilizing the endoscope as well as a guidewire. A jejunostomy (J) tube was then placed via the G tube under endoscopic guidance. The J tube was subsequently anchored in the second portion of the duodenum using endoscopic clips and surgical sutures (Figure 2). After feeds were initially restarted, the patient was unable to tolerate continuous feeding as she was having episodes of minimal emesis once the feeding rate exceeded 40 cc/hr. The patient was switched to bolus feeds, which she tolerated well with no episodes of emesis or leakage from the tube. After several days of tolerating bolus feeding, the patient was safely discharged.
Jejunal limb of PEG-J tube within the mid-esophagusPEG-J: Percutaneous endoscopic gastro-jejunal
Jejunal limb of new PEG-J tube anchored with endoscopic clipsPEG-J: Percutaneous endoscopic gastro-jejunal
Discussion
Tube migration is a known complication of PEG-J tube placement and is associated with negative outcomes such as aspiration, sepsis, hemorrhage, and fistulization. A retrospective study of PEG-J tubes placed using endoscopic clips and surgical sutures found that 7% of all tube placement was complicated by migration [10]. Anterograde migration rarely occurs when sutures anchoring the tube in place erode through the skin, leading to tube dislodgement [11]. Physiologic peristalsis subsequently pushes the tube more distally into the small bowel and, in some cases, can even get into the colon [12]. In contrast, the retrograde migration of PEG-J tubes into the stomach itself is well documented in the literature [13]. A recent retrospective review found that tube insertion into the gastric body rather than the antrum and tube entry tracts directed away from the pylorus rather than toward it were both associated with a greater likelihood of retrograde migration of the jejunal limb into the stomach [14].
Retrograde migration of the jejunal limb of PEG-J tubes into the esophagus is extremely rare in the adult population, with only two reported cases in the literature [15,16]. In both cases, proximal tube migration was associated with vomiting and aspiration. As feeds are exiting the tube more proximally into the esophagus instead of the small bowel, the feeds being in closer proximity to the respiratory tract puts the patient at a much higher risk of aspiration. Although our patient only presented with a malfunctioning PEG-J tube rather than the acute vomiting or aspiration pneumonia presentation that has previously been reported, it is definitely worth noting that the patient had recently been discharged from a three-month-long hospitalization for sepsis secondary to pneumonia. In retrospect, it is likely that retrograde migration of the PEG-J tube occurred months before the patient’s current presentation and may have been a triggering event for aspiration that resulted in hospitalization for pneumonia and sepsis.
Conclusions
This case report describes the retrograde migration of a PEG-J tube into the esophagus, highlighting an extremely rare complication of PEG-J tubes. This complication can have various presentations; it may involve persistent gagging or vomiting, the development of aspiration pneumonia, or it can simply present as an inability for the tube to flush properly. While the distal placement of PEG-J tubes is designed to prevent feed aspiration, it does not completely eliminate the risk. Retrograde migration is one potential complication that significantly increases the risk of aspiration. Tube migration into the esophagus should be within the differential diagnosis for patients with PEG-J tubes presenting with aspiration pneumonia.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Percutaneous Gastrostomy and Jejunostomy Hitawala AA Mousa OY Treasure Island Stat Pearls 2023 https://www.ncbi.nlm.nih.gov/books/NBK 559215/32644641 · pubmed ↗
- 2Percutaneous endoscopic gastrostomy and jejunostomy: indications and techniques World J Gastrointest Endosc Fugazza A Capogreco A Cappello A 2502661420223571990210.4253/wjge.v 14.i 5.250PMC 9157691 · doi ↗ · pubmed ↗
- 3Percutaneous endoscopic gastrostomy: indications, technique, complications and management World J Gastroenterol Rahnemai-Azar AA Rahnemaiazar AA Naghshizadian R Kurtz A Farkas DT 773977512020142497671110.3748/wjg.v 20.i 24.7739 PMC 4069302 · doi ↗ · pubmed ↗
- 4Enteral nutrition by nasogastric tube in adult patients under palliative care: a systematic review Nutrients Sánchez-Sánchez E Ruano-Álvarez MA Díaz-Jiménez J Díaz AJ Ordonez FJ 15621320213406638610.3390/nu 13051562 PMC 8148195 · doi ↗ · pubmed ↗
- 5Percutaneous endoscopic transgastric jejunostomy (PEG-J): a retrospective analysis on its utility in maintaining enteral nutrition after unsuccessful gastric feeding BMJ Open Gastroenterol Yoon EWT Yoneda K Nakamura S Nishihara K 03201610.1136/bmjgast-2016-000098 PMC 494770827486522 · doi ↗ · pubmed ↗
- 6Fluoroscopy-guided jejunal extension tube placement through existing gastrostomy tubes: analysis of 391 procedures Diagn Interv Radiol Uflacker A Qiao Y Easley G Patrie J Lambert D de Lange EE 4884932120152638089510.5152/dir.2015.14524 PMC 4622397 · doi ↗ · pubmed ↗
- 7Short- and long-term outcomes from percutaneous endoscopic gastrostomy with jejunal extension Surg Endosc Ridtitid W Lehman GA Watkins JL Mc Henry L Fogel EL Sherman S CotéGA 290129093120172779660110.1007/s 00464-016-5301-3PMC 5409872 · doi ↗ · pubmed ↗
- 8Buried bumper syndrome: a complication of percutaneous endoscopic gastrostomy World J Gastroenterol Cyrany J Rejchrt S Kopacova M Bures J 6186272220162681161110.3748/wjg.v 22.i 2.618PMC 4716063 · doi ↗ · pubmed ↗