Depression and Anxiety Symptoms Among Cisgender Gay and Bisexual Men During the Onset of the COVID-19 Pandemic: Time Series Analysis of a US National Cohort Study
Chloe Mirzayi, Drew Westmoreland, Matthew Stief, Christian Grov

TL;DR
This study found that cisgender gay and bisexual men in the Northeast and Midwest of the US experienced rising depression and anxiety symptoms during the early months of the COVID-19 pandemic, but not in other regions.
Contribution
The study reveals regional differences in mental health impacts of the pandemic among LGBTQ individuals, highlighting the need to consider geographic variation in future research.
Findings
Depression and anxiety symptoms increased in the Northeast and Midwest during the pandemic onset.
No such increase was observed in the South and West regions during the same period.
These trends were not present in data from 2018-2019, indicating pandemic-specific effects.
Abstract
The onset of the COVID-19 pandemic in the United States in March 2020 caused a dramatic change in the way many people lived. Few aspects of daily life were left undisrupted by the pandemic’s onset as well as the accompanying policies to control the spread of the disease. Previous research has found that the pandemic may have significantly impacted the mental health of lesbian, gay, bisexual, transgender, and queer (LGBTQ) individuals—potentially more so than other individuals. However, the pandemic did not affect all areas of the United States at the same time, and there may be regional variation in the impact of the onset of the pandemic on depressive symptoms among LGBTQ individuals. To assess regional variation of the impact of the pandemic, we conducted a time series analysis stratified by US geographic region to examine symptoms of depression and anxiety among a sample of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
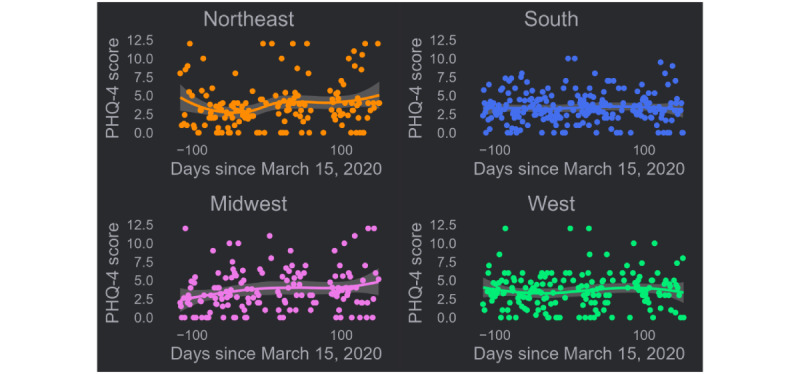 Figure 1
Figure 1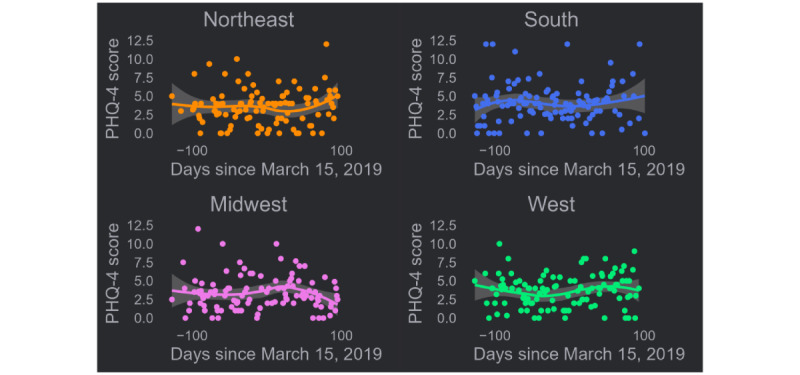 Figure 2
Figure 2| Demographics | Northeast (n=784) | Midwest (n=780) | South (n=2285) | West (n=1158) | Total (N=5007) | PHQ-4 score, mean (SD) | |
|
| |||||||
|
| Black | 77 (9.8) | 55 (7.1) | 330 (14.4) | 45 (3.9) | 507 (10.1) | 2.8 (3.3) |
|
| Hispanic | 158 (20.2) | 99 (12.7) | 580 (25.4) | 376 (32.5) | 1213 (24.2) | 3.1 (3.4) |
|
| White | 419 (53.4) | 544 (69.7) | 1146 (50.2) | 568 (49.1) | 2677 (53.5) | 3.7 (3.5) |
|
| Others or multiracial | 130 (16.6) | 82 (10.5) | 229 (10) | 169 (14.6) | 610 (12.2) | 3.5 (3.6) |
|
| |||||||
|
| Cisgender men | 758 (96.7) | 762 (97.7) | 2234 (97.8) | 1131 (97.7) | 4885 (97.6) | 3.4 (3.5) |
|
| Transgender men | 9 (1.1) | 5 (0.6) | 18 (0.8) | 7 (0.6) | 39 (0.8) | 5.7 (4.1) |
|
| Transgender women | 1 (0.1) | 3 (0.4) | 10 (0.4) | 7 (0.6) | 21 (0.4) | 1.8 (2.0) |
|
| Others or nonbinary | 16 (2) | 10 (1.3) | 23 (1) | 13 (1.1) | 62 (1.2) | 5.4 (4.1) |
|
| |||||||
|
| Gay, queer, or homosexual | 697 (88.9) | 678 (86.9) | 1926 (84.3) | 990 (85.5) | 4291 (85.7) | 3.5 (3.5) |
|
| Bisexual | 81 (10.3) | 96 (12.3) | 328 (14.4) | 155 (13.4) | 660 (13.2) | 3.3 (3.5) |
|
| Straight or heterosexual | 0 (0) | 2 (0.3) | 7 (0.3) | 4 (0.3) | 13 (0.3) | 3.5 (4.1) |
|
| Others | 6 (0.8) | 4 (0.5) | 24 (1.1) | 9 (0.8) | 43 (0.9) | 4.2 (3.9) |
| Age (years), mean (SD) | 32.6 (7.5) | 33.5 (8.0) | 32.5 (8.1) | 33.5 (7.1) | 32.9 (7.9) | N/Ab | |
| Region | 2019 | 2020 | ||
|
| τ | τ | ||
| Northeast | 0.05 | .44 | 0.12 | .03 |
| Midwest | 0.00 | .96 | 0.14 | .01 |
| South | 0.01 | .83 | 0.00 | .96 |
| West | 0.07 | .26 | 0.03 | .50 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLGBTQ Health, Identity, and Policy · COVID-19 and Mental Health
Introduction
The onset of the COVID-19 pandemic in the United States in early 2020 represented a nearly unprecedented disruption in daily life for many Americans. Widespread disruptions were present in nearly every facet of daily life, including in workplaces, schools, and social settings. Mandatory business closures and recommended social distancing were implemented with some heterogeneity in the United States. Many states in the Northeast, Midwest, and West implemented stay-at-home orders in March 2020 prior to Southern states, where the pandemic later took hold in the summer [1].
Several large studies have linked the onset of the pandemic to a significant increase in the symptoms of depression and anxiety in US adults [2-5]. Other studies have found that lesbian, gay, bisexual, transgender, and queer (LGBTQ) people may be particularly vulnerable to developing symptoms of depression and anxiety relative to non-LGBTQ populations [6]. For instance, a study of cannabis users conducted during the pandemic found that the LGBTQ cannabis users were more likely to report symptoms of depression and anxiety [7]. Similarly, a national longitudinal cohort study of LGTBQ adults found increased anxiety and depression symptoms among participants after the beginning of the pandemic [8]. Additionally, a study of LGBTQ college students found that nearly half had unmet mental health needs during the first few months of the pandemic [6]. These findings may be due to being confined in uncomfortable home situations or isolation from friends, which may have disparate impacts on LGBTQ individuals compared to others [9]. However, other studies have found decreased anxiety symptoms and no differences in depressive symptoms before and after the start of the pandemic [10].
Recently, researchers have proposed potential mechanisms by which the onset of the COVID-19 pandemic may have disproportionately affected LGBTQ people. A web-based study in Germany during the pandemic found that depressive symptoms were mediated by loneliness [11], while a study of Mexican LGBTQ people found that perceived social support also acted as a mediator [12]. Taken together, it appears that a lack of access to supportive friends and other members of the LGBTQ community, and the accompanying loneliness, may be one mechanism through which the COVID-19 pandemic, and associated lockdowns, had a greater impact on LGBTQ individuals compared to others.
Despite several studies finding that LGBTQ people were more likely to experience symptoms of depression and anxiety with the onset of the COVID-19 pandemic, we have been unable to identify any studies that examined trends in symptoms and anxiety over time for the period. Time series studies have been used to examine trends in mental health leading up to and immediately following the 2016 US presidential election [13], in mental health referrals during the pandemic [14,15], and in suicide mortality also during the COVID-19 pandemic [16]. However, to our knowledge, no study has examined symptoms of depression and anxiety in an LGBTQ population during the onset of the COVID-19 pandemic in the United States using a time series approach.
The aim of this study was to examine the effects of the onset of the first wave of the COVID-19 pandemic on a population of primarily gay and bisexual men, but also transgender men and transgender women as well as nonbinary people, using time series analysis. Given the heterogeneity of the burden of cases and in COVID-19 policies, analyses were stratified by US census region. We hypothesized that regions that were more impacted by the early onset of the COVID-19 pandemic or had more stringent pandemic control policies or recommendations (eg, the Northeast) would show an increase in symptoms of depression and anxiety as the pandemic progressed.
Methods
Study Population
Participants were members of Together 5000, a US national cohort of primarily cisgender gay and bisexual men at risk for HIV recruited from sexual networking applications. Members of the cohort complete yearly web-based surveys as well as at-home HIV testing beginning in 2017 and running through the onset of the pandemic. The yearly web-based surveys assessed a variety of health-related domains such as socioeconomic factors, drug and alcohol use, sexual behaviors, food and housing insecurity, and mental health measures. A detailed profile of the study procedures and participants has been published elsewhere [17].
Measures
Data Collection
Data for this study were primarily taken from participants’ 24-month assessment. These assessments began on November 20, 2019 (–116 days), and ran through August 15, 2020 (+153 days)—with some participants completing their assessment prior to the onset of the COVID-19 pandemic in the United States and others completing it after. We defined the onset as March 15, 2020, which roughly coincides with the beginning of the week in which many local and state governments announced mandatory closure of nonessential businesses and schools [18-20].
To establish whether a similar trend would be observed in prior yearly assessments, we compared 24-month results to participants’ 12-month assessment (all of which were conducted prior to the pandemic). Survey completion dates were calculated relative to March 15, 2019, and ranged from November 7, 2018 (–127 days), to June 24, 2019 (+101 days).
Demographics
On the baseline survey, race and ethnicity information was assessed using a list of common racial and ethnic categories for participants to select all that apply. Participants were also given the ability to specify their own race or ethnicity. These options were recoded to a 4-category variable representing Black, Hispanic, White, and multiracial or others. To assess current gender identity, participants were asked their assigned sex at birth as well as their current gender identity. Participants had the option of writing in their own gender identity. The variable was then recoded into 5 categories: cisgender man, cisgender woman, transgender man, transgender woman, or others or nonbinary. Finally, participants were asked to select the best option for their sexual orientation: gay, queer, or homosexual; bisexual; straight or heterosexual; or others. This variable was not recoded prior to analysis.
Region
Participants self-reported their zip codes at baseline and were able to provide updated zip codes during the 12- and 24-month assessments. These zip codes were coded into state of residence, which in turn were categorized according to US census regions [21].
Patient Health Questionnaire-4
The 4-item Likert-type Patient Health Questionnaire-4 (PHQ-4) was used to assess symptoms of anxiety and depression. The Patient Health Questionnaire-2, a measure of depression, and Generalized Anxiety Disorder-2, a measure of anxiety, constitute the PHQ-4. The reliability and validity of the PHQ-4 in the general population have been previously established [22]. The PHQ-4 is scored from 0 to 12, with an increasing score indicating increasingly severe anxiety and depressive symptomology. The continuous measure was used for analyses.
Statistical Analysis
PHQ-4 scores were stratified by US census region of residence and then plotted as a function of the survey completion date for participants completing the 24-month assessment, which ran from November 20, 2019, to August 15, 2020. A locally estimated scatterplot smoothing trend line with 95% CI was applied. A sieve-bootstrap Mann-Kendall test for monotonic trends was conducted to assess the presence and direction of trends in the scores. All steps of this analysis were then repeated for the 12-month assessment for comparison.
Analyses were conducted in R (version 4.1.0; R Foundation for Statistical Computing). Plots and trend lines were created using the ggplot2 package [23], while the test for trend was conducted using the funtimes package [24].
Ethical Considerations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review board (Institutional Review Board of the City University of New York Graduate School of Public Health and Health Policy, IRB file #2017-0893) and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All participants provided informed consent for data collection at each assessment. Participant data were deidentified and stored in an encrypted closed network. Participants received US $25 Amazon gift cards for completing study assessments.
Results
In total, 5007 participants completed the 24-month assessment survey and resided in 1 of the 4 US census regions. An additional 22 participants completed the survey but resided in a US territory and were not included in these analyses. Of these 5007 participants, 784 (15.6%) resided in the Northeast, 780 (15.6%) resided in the Midwest, 2285 (45.6%) resided in the South, and 1158 (23.1%) resided in the West.
Demographically, 507 (10.1%) participants were Black, 1213 (24.2%) were Hispanic, 2677 (53.5%) were White, and 610 (12.2%) were another race or multiracial. The mean age of the sample at the 24-month assessment was 32.9 (SD 7.5) years. The sample was primarily cisgender men with 4885 (97.6%) identifying as such, with the remaining 122 (2.4%) participants identifying as transgender men, transgender women, or nonbinary. A substantial proportion of the sample identified as gay, queer, or homosexual (n=4291, 85.7%) or bisexual (n=660, 13.2%), with the remainder identifying as others. Full demographics as well as PHQ-4 scores stratified by demographic variables are presented in Table 1.
The mean PHQ-4 score at the 24-month assessment was 4.0 (SD 3.0), while the mean PHQ-4 score at the 12-month assessment was 3.7 (SD 2.4). A paired 2-tailed t test revealed this difference to be statistically significant (t4653=2.99; P=.019), indicating an overall increase in PHQ-4 scores between the 12-month assessment and the 24-month assessment.
Survey completion dates for the 24-month assessment were calculated relative to the onset of the COVID-19 pandemic, with a 0 representing March 15, 2020. These dates ranged from November 20, 2019, to August 15, 2020. Individual participant Generalized Anxiety Disorder–Patient Health Questionnaire scores were then plotted as a function of survey completion dates stratified by US census region.
The locally estimated scatterplot smoothing trend line in PHQ-4 scores for the Northeast revealed a trend downward in the days immediately prior to the onset of the pandemic with an upturn in scores following the onset (Figure 1). This trend was significant (τ=0.12; P=.03). A small, steady increase in scores was also observed among participants in the Midwest, beginning prior to the pandemic onset and continuing through to the summer (τ=0.14; P=.01). No trends are immediately apparent in the trend lines for the South and West, and tests for trends were not statistically significant (Table 2).
To establish whether a similar trend would be observed in other yearly assessments, the same analysis was conducted for the 12-month assessment (Figure 2). Inspection of the figure reveals a decrease in scores for participants in the Northeast after March 15, 2019, followed by a sharp upturn at the end. Midwest participant scores decreased markedly shortly after March 15, 2019. A small, nonsignificant oscillation in scores was observed among Western participants. No clear trend was observed in scores among Southern participants. All tests for monotonic trends were nonsignificant for 2019 (all P>.05; Table 2), indicating, compared to 2020, there was no observed trend in PHQ-4 scores over time.
US census region–stratified trends in PHQ-4 scores over time before and after the onset of the COVID-19 pandemic of a prospective US national cohort study of primarily cisgender gay and bisexual men in 2020. PHQ-4: Patient Health Questionnaire-4.
US census region–stratified trends in PHQ-4 scores over time before and 1 year prior to the onset of the COVID-19 pandemic of a prospective US national cohort study of primarily cisgender gay and bisexual men in 2019. PHQ-4: Patient Health Questionnaire-4.
Discussion
Principal Findings
The region-stratified time series analysis of symptoms of depression and anxiety in the days leading up to and following the onset of the COVID-19 pandemic in the United States revealed significant positive trends among participants in the Northeast and Midwest. These trends were not observed in the South or West, nor were they present the previous year.
The disparate impact of the COVID-19 pandemic on the Northeast [25] as well as heterogeneous COVID-19 policies across the United States may explain the observed trends. Other studies have found that lockdown policies, along with adherence to them, may have resulted in increased depressive symptoms [26].
Comparison to Prior Work
The findings of significant positive trends in symptoms of depression and anxiety during the onset of the COVID-19 pandemic were consistent with similar studies that found an increased prevalence of depression and anxiety among the general population as well as LGBTQ people during the COVID-19 pandemic [2,6]. However, to our knowledge, this is the first time-series analysis of symptoms of anxiety and depression conducted in an LGBTQ population with data before and after the onset of the COVID-19 pandemic in the United States as well as the first study to identify a regional trend in this population.
Other time series studies have shown the impact of the COVID-19 pandemic on related mental health constructs. A UK study found a significant decrease in referrals to mental health services during the start of the pandemic, although this study was not focused specifically on sexual minorities [14]. Another study of the general population found a decrease in emergency department visits for psychiatric issues [27]. The decrease in mental health service use combined with increased symptoms could indicate a clear, unmet need for mental health care during the beginning of the COVID-19 pandemic. It is important to consider that the pandemic may have had differential effects on sexual minority individuals based on stigma and vulnerabilities. For instance, young adults who had to return to their parents’ homes as a result of the pandemic were found to have faced greater psychological distress [28]. Future studies could explore whether the observed regional effects were modified by changes in living arrangement. Another potential effect modifier could be social support that other studies have found as an important protective effect for sexual minority populations against depressive symptoms [29].
Limitations
There are some limitations to this study. Survey completion dates were used in calculating days relative to March 15, 2020, and March 15, 2019. It is possible for participants to have started the survey, completed the PHQ-4, and then not completed the survey in its entirety until several days later; however, we do not believe this would have tremendously impacted responses in a meaningful way nor were there enough participants who started before March 15, 2020, and completed it after March 15, 2020, to have had a discernible impact on aggregate results. There also may be other important factors that affect the mental health of sexual minority populations that were not included in this study such as internalized homonegativity [30], social connectedness [31], and minority stress [32]. Finally, the study population was primarily cisgender gay and bisexual men and therefore does not represent the full spectrum of LGBTQ individuals.
Conclusions
We found evidence of increased depression and anxiety symptoms among a sample of primary cisgender gay and bisexual men during the initial onset of the COVID-19 pandemic in 2020 in the Midwest and Northeast regions of the United States. This trend was not similar among the same study population the previous year nor among participants in the South or West regions of the United States.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mervosh S Lu D Swales V See which states and cities have told residents to stay at home The New York Times 20202022-02-01 https://www.nytimes.com/interactive/2020/us/coronavirus-stay-at-home-order.html
- 2Ettman CK Abdalla SM Cohen GH Sampson L Vivier PM Galea S Prevalence of depression symptoms in US adults before and during the COVID-19 pandemic JAMA Netw Open 202039 e 2019686 10.1001/jamanetworkopen.2020.1968632876685277014632876685 PMC 7489837 · doi ↗ · pubmed ↗
- 3Twenge JM Joiner TE Mental distress among U.S. adults during the COVID-19 pandemic J Clin Psychol 2020761221702182 10.1002/jclp.230643303760833037608 PMC 7675251 · doi ↗ · pubmed ↗
- 4Riehm KE Holingue C Smail EJ Kapteyn A Bennett D Thrul J Kreuter F Mc Ginty EE Kalb LG Veldhuis CB Johnson RM Fallin MD Stuart EA Trajectories of mental distress among U.S. adults during the COVID-19 pandemic Ann Behav Med 202155293102 10.1093/abm/kaaa 12633555336613080733555336 PMC 7929474 · doi ↗ · pubmed ↗
- 5Daly M Robinson E Anxiety reported by US adults in 2019 and during the 2020 COVID-19 pandemic: population-based evidence from two nationally representative samples J Affect Disord 2021286296300 10.1016/j.jad.2021.02.05433756307 S 0165-0327(21)00188-933756307 PMC 9754788 · doi ↗ · pubmed ↗
- 6Gonzales Gde Mola EL Gavulic KA Mc Kay T Purcell C Mental health needs among lesbian, gay, bisexual, and transgender college students during the COVID-19 pandemic J Adolesc Health 2020675645648 10.1016/j.jadohealth.2020.08.00632933837 S 1054-139X(20)30488-232933837 PMC 10251764 · doi ↗ · pubmed ↗
- 7Gattamorta KA Salerno JP Islam JY Vidot DC Mental health among LGBTQ cannabis users during the COVID-19 pandemic: analysis of the COVID-19 cannabis health study Psychol Sex Orientat Gend Divers 202182172179 10.1037/sgd 00004913671419836714198 PMC 9880987 · doi ↗ · pubmed ↗
- 8Flentje A Obedin-Maliver J Lubensky ME Dastur Z Neilands T Lunn MR Depression and anxiety changes among sexual and gender minority people coinciding with onset of COVID-19 pandemic J Gen Intern Med 202035927882790 10.1007/s 11606-020-05970-43255687710.1007/s 11606-020-05970-432556877 PMC 7299558 · doi ↗ · pubmed ↗