Pregnancy-Related Eccrine Angiomatous Hamartoma: Case Report
Jonathan David Serrano Arias, Juan Jacobo Del Valle Saavedra, Luz Ellis Arrieta Blanquicet, Ana C Ruiz Suarez

TL;DR
This paper reports a rare case of a benign skin tumor that grew rapidly during pregnancy and was challenging to diagnose.
Contribution
The paper presents a unique case of eccrine angiomatous hamartoma with rapid growth during pregnancy.
Findings
The tumor showed rapid growth during pregnancy, which is unusual for this typically slow-growing condition.
A superficial biopsy complicated the differential diagnosis due to the tumor's atypical presentation.
The case highlights the challenges in diagnosing eccrine angiomatous hamartoma during pregnancy.
Abstract
Eccrine angiomatous hamartoma is rare, slow-growing, and benign neoplasm that is diagnosed based on clinical characteristics and histological findings. It usually presents as a solitary nodule on the extremities and may arise at birth or in childhood. Although it is usually asymptomatic, in some cases it can cause pain and hyperhidrosis. From a histological perspective, it is characterized by an increase in the number of eccrine glands and a proliferation of vascular channels. We present the case of a 26-year-old woman who developed an eccrine angiomatous hamartoma in her right leg. The rapid growth of the lesion during pregnancy coupled with the challenges posed by a superficial biopsy, complicated the differential diagnosis.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
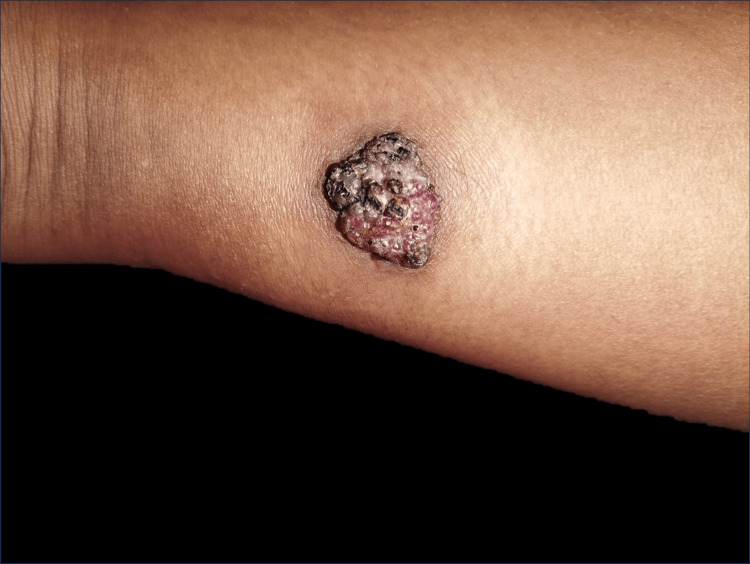 Figure 1
Figure 1 Figure 2
Figure 2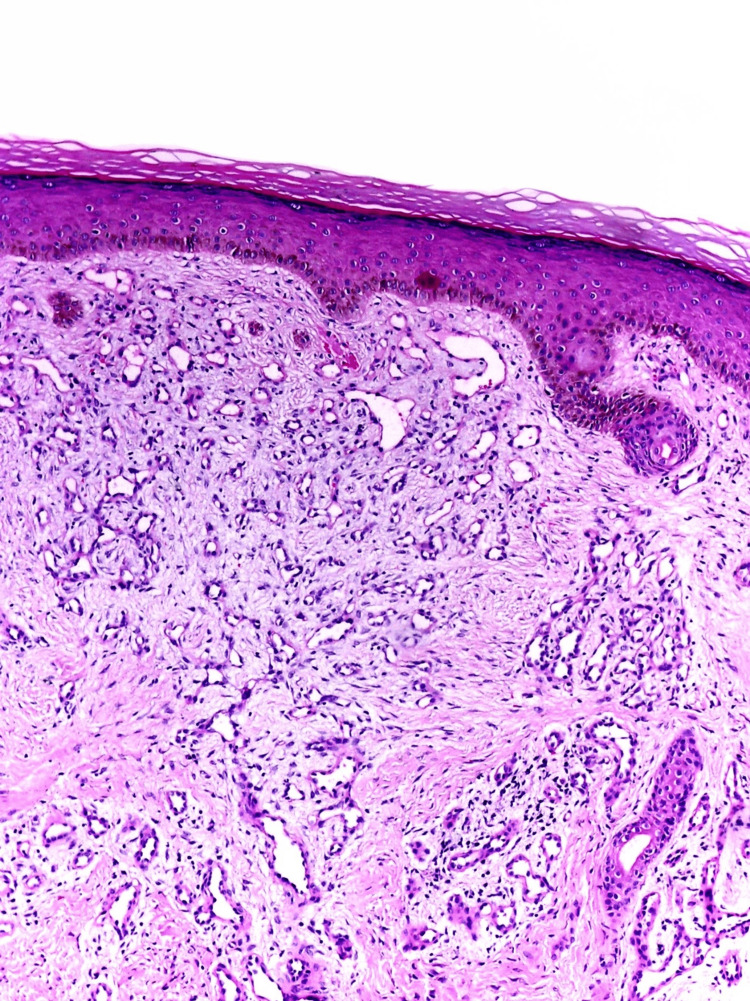 Figure 3
Figure 3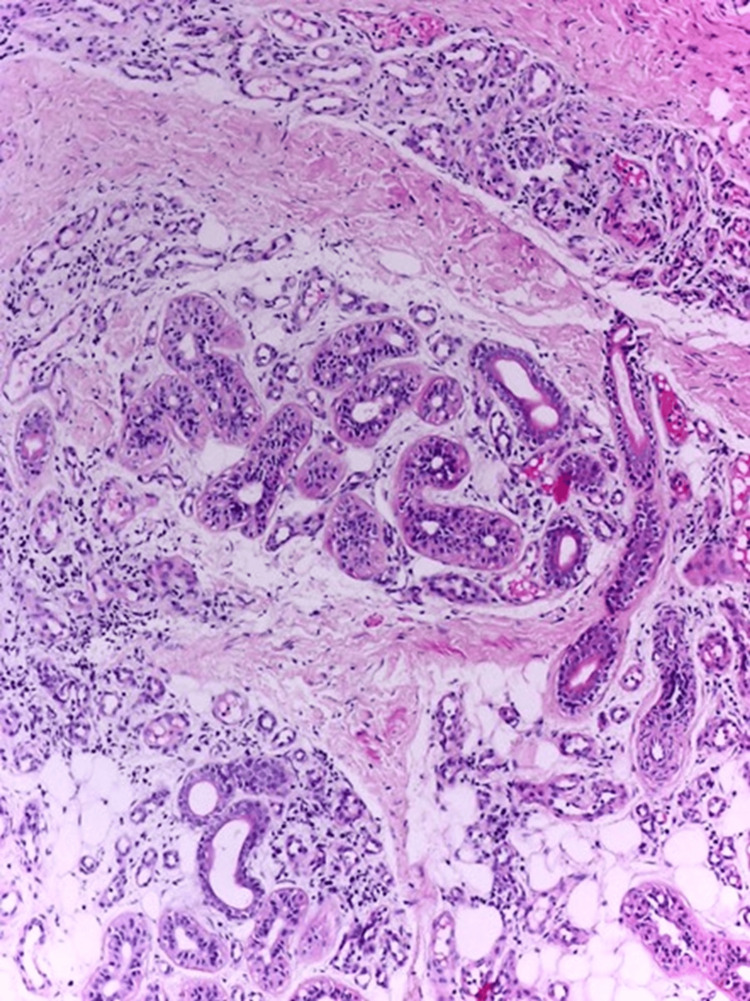 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSympathectomy and Hyperhidrosis Treatments · Chemotherapy-related skin toxicity · Cancer and Skin Lesions
Introduction
Eccrine angiomatous hamartoma (EAH), also known as eccrine angiomatous nevus, is a rare, benign skin malformation that typically manifests at birth or during childhood, although cases have been documented in adults, with a mean age of 16.4 and 21.1 years [1,2]. Due to its low frequency, there isn't extensive epidemiological information available. It often appears as a solitary pink nodule or plaque on the extremities and is generally asymptomatic, but it may cause pain and hyperhidrosis [3]. The increase in size of EAH is proportional to the patient. Histologically, it is characterized by an increase in the number of eccrine sweat glands and the presence of a significant amount of capillaries in the deep and mid dermis [1,2]. There is an association with other vascular anomalies such as arteriovenous malformations, verrucous hemangioma, and spindle cell hemangioma [2,4]. As it is a benign condition, it generally does not require intervention unless it causes discomfort to the patient in terms of pain, hyperhidrosis, or aesthetic concerns [3,5].
Case presentation
A 26-year-old woman with no significant medical history sought medical attention for an erythematous lesion on the distal and posterior region of her right leg, which had been present since birth. During her first pregnancy, the lesion experienced rapid growth and was accompanied by localized pain and hyperhidrosis. Evaluation revealed a single exophytic tumor, black and pink in color, measuring 30x25 mm in size, well-defined, with keratotic areas, and a multilobulated granulomatous appearance (Figures 1, 2).
Exophytic tumor, well-circumscribed, black and pink in color, infiltrating the distal and posterior region of the right leg.
Lateral view of the lesion showing its wart-like appearance with a multilobulated and keratotic surface.
No other abnormalities were identified in the patient's general and systemic examination. Initially, infiltrative lesions were considered as differential diagnoses as sarcoma or squamous cell carcinoma
A first shave biopsy was performed, resulting in a significant reduction in the size of the lesion, and the hyperhidrosis was limited to the central part of it. The report from this initial biopsy suggested the presence of a pyogenic granuloma. Given the differential diagnoses, a decision was made to conduct another biopsy, this time at a greater depth. The histopathological study of the second biopsy (validated by two pathologists) revealed a lesion that was relatively circumscribed but not encapsulated, composed of a hamartomatous proliferation of secretory eccrine glands and ducts intimately intermixed with a proliferation of small, ectatic blood vessels, the size of a capillary. Additionally, a component of mature adipose tissue was found. The epidermis showed no significant changes, and there was no evidence of atypia or an increase in mitotic activity. With these histological findings, the final diagnosis of EAH was confirmed (Figures 3, 4).
Proliferation of small caliber ectatic vascular structures in the superficial dermis (hematoxylin-eosin stain, original magnification x10).
Eccrine angiomatous hamartoma showing small caliber ectatic blood vessels intermixed with multiple eccrine glands and mature adipocytes (hematoxylin-eosin stain, original magnification x10).
After the second biopsy, the lesion completely regressed and after one year there have been no recurrences.
Discussion
Eccrine angiomatous hamartoma is characterized by the presence of solitary nodules or plaques, with macular forms in the minority of cases, sometimes with a velvety appearance or verrucous surface, ranging from an average diameter of 3 to 11 cm. Its coloration resembles the patient's skin, although it may present yellowish, pink, blue, or even violet discoloration. There is a predilection for the distal areas of the limbs and palmoplantar regions, although it can be found in other anatomical areas such as the face, neck, buttocks, and sacral region [2,4-6].
In the two most comprehensive retrospective case series in recent years by Sanusi et al. and Patterson et al., which included 26 and 18 cases, respectively, it was observed that EAH occurred from congenital cases up to 84 years, showing a slight male predominance and primarily located on the limbs [7,8]. While several of these characteristics were present in our patient, including the described solitary lesion, the fact that she had a biphasic growth behavior after her pregnancy, and considering that her initial biopsy showed characteristics of a pyogenic granuloma, posed a diagnostic challenge. Additionally, the mentioned case series did not comment on the existence of any biphasic form congenitally, with sudden growth in adulthood related to pregnancy, as was the case with our patient.
Considering that this tumor involves the proliferation of vascular channels, the angiogenic and hormonal factors observed in pregnancy could be a contributing factor to the development of these lesions. Just as in the case reported by Gabrielsen et al., where a 34-year-old woman in her second trimester of pregnancy was diagnosed, following a histopathological study, with EAH on the distal phalanx of the fifth finger of her left hand [9]. As studied in other vascular proliferations, there is an increase in the levels of vascular endothelial growth factor (VEGF) and basic fibroblast growth factor (bFGF), and less circulating tumor necrosis factor-alpha (TNF-α) compared to the control population, which is associated with their formation [10].
The clinical suspicion of a vascular lesion can be confirmed through imaging studies such as nuclear magnetic resonance, ultrasound or color Doppler, but the precise diagnosis requires histology [3,11]. The distinctive microscopic characteristics of EAH include an increase in the number of eccrine glands in the mid and lower dermis, with ectatic or collapsed vessels in relation to hyperplastic eccrine units. This is associated with varying proportions of mature adipose tissue, lymphatics, smooth muscle, pilosebaceous structures, neural elements, and, rarely, bone tissue. The overlying epidermis may be normal or show acanthosis or papillomatosis. Immunohistochemical studies have shown positivity of the eccrine component for S100 and of the vascular component for markers CD31, CD34, and factor VIII [1,2,4,7,12].
In the differential diagnosis, various entities should be considered, such as vascular tumors and vascular malformations, and the approach to painful tumors should not be overlooked [3,13]. In our case, a superficial biopsy was interpreted as a vascular lesion of capillary lobular hemangioma type (pyogenic granuloma), possibly due to the difficulty in appreciating the eccrine glandular component present in the mid and lower dermis. Additionally, eccrine angiomatous hamartoma is a rare lesion and therefore not widely recognized by pathologists and dermatologists. We emphasize the importance of performing a punch biopsy rather than shave biopsies when EAH is suspected. The clinical course of this condition is always benign, with no reports of malignant potential. Regarding treatment, it has been observed that simple excision is often curative, and aggressive resections are not justified [14]. Recently, successful treatment has been achieved using intralesional botulinum toxin and sclerosants [3].
Conclusions
EAH is a rare condition that should be considered in the management of painful and rapidly growing tumors temporally related to pregnancy. It still has a vascular component that is sensitive to hormones and growth factors related to pregnancy. Despite its benign etiology, due to its rapid growth, it is essential to rule out any of the multiple malignant tumors of the skin adnexa, even in tissues found at greater depths. Deep biopsies are necessary to distinguish between glandular and vascular components since a superficial biopsy may not characterize all the components described in its histopathology. This approach ensures a more precise diagnosis for pregnant patients who require it.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mc Kee’s Pathology of the Skin, 5th ed Calonje E Brenn T Lazar AJ Billings SD Edinburg Elsevier 2018
- 2Eccrine angiomatous hamartoma with arteriovenous malformation: a rare entity re-explored Cureus Al-Zaidi RS Alotaibi G Aljuaid M 014202210.7759/cureus.23669 PMC 905528835505764 · doi ↗ · pubmed ↗
- 3Facial eccrine angiomatous hamartoma in a 52-year-old woman: a case report SAGE Open Med Case Rep Ahmad SM Mohammad T Elsebaey AM 205031311202310.1177/2050313 X 231161440 PMC 1003426936968990 · doi ↗ · pubmed ↗
- 4Eccrine angiomatous hamartoma with verrucous hemangioma-like features - an unusual combination Indian J Dermatol Venereol Leprol Liu L Zhou L Zhao Q Wei D Jiang X 8428448720213437994810.25259/IJDVL_195_2021 · doi ↗ · pubmed ↗
- 5Eccrine angiomatous hamartoma in an adult BMJ Case Rep Mendes SR Gameiro AR Cardoso JC TellecheaÓ 14202110.1136/bcr-2020-240422 PMC 790306733619145 · doi ↗ · pubmed ↗
- 6Congenital eccrine angiomatous hamartoma: expanding the morphologic presentation and a review of the literature Pediatr Dermatol Smith SD Di Caudo DJ Price HN Andrews ID 9099123620193141090510.1111/pde.13974 · doi ↗ · pubmed ↗
- 7Eccrine angiomatous hamartoma: a clinicopathologic review of 18 cases Am J Dermatopathol Patterson AT Kumar MG Bayliss SJ Witman PM Dehner LP Gru AA 4134173820162676068410.1097/DAD.0000000000000430 · doi ↗ · pubmed ↗
- 8Adult-onset eccrine angiomatous hamartoma: report of a rare case Indian J Dermatol Yaghoobi R Pazyar N Mostufi E Hemmati E 4314346620213475941310.4103/ijd.IJD_702_19PMC 8530048 · doi ↗ · pubmed ↗