KIAA1549-BRAF Gene Fusion Spindle Cell Sarcoma With Infantile Fibrosarcoma-Like Pattern in a Pediatric Patient: A Case Report
Rawan A Abualola, Tariq Al-Zaid

TL;DR
A three-year-old girl was diagnosed with a rare childhood sarcoma involving a KIAA1549-BRAF gene fusion, which resembles infantile fibrosarcoma and responded well to treatment.
Contribution
The case highlights the diagnostic importance of molecular testing for KIAA1549-BRAF fusion in tumors resembling infantile fibrosarcoma.
Findings
The tumor showed a favorable outcome three years after surgery.
Molecular testing was essential for accurate diagnosis due to morphological similarity to infantile fibrosarcoma.
The KIAA1549-BRAF fusion suggests potential for targeted therapies in refractory cases.
Abstract
Spindle cell sarcoma with KIAA1549-BRAF fusion is a type of childhood sarcoma that closely resembles infantile fibrosarcoma by morphologic criteria and harbors molecular alteration other than the ETV6-NTRK3 fusion gene. This neoplasm was diagnostically challenging without molecular tests, including next-generation sequencing. The discovery of BRAF translocation in this tumor contributes to the promise of the clinical implication of selecting new therapeutic options for the treatment of progressive diseases that are refractory to conventional chemotherapy. Here we present the case of a three-year-old girl who was diagnosed with spindle cell sarcoma with KIAA1549-BRAF fusion gene and had a favorable outcome three years after surgery.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
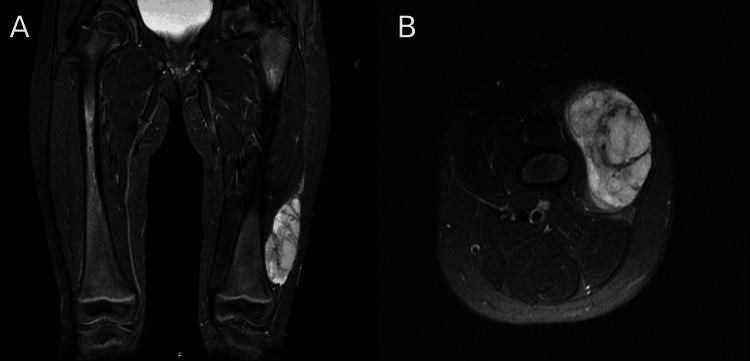 Figure 1
Figure 1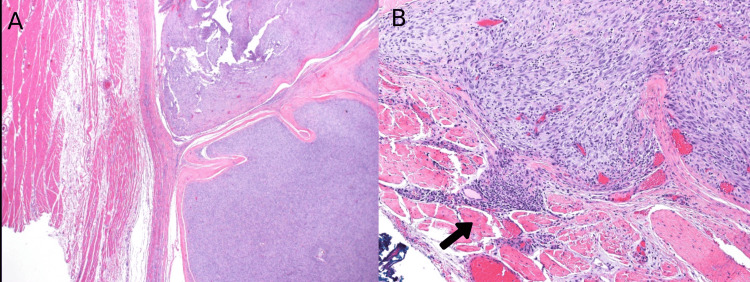 Figure 2
Figure 2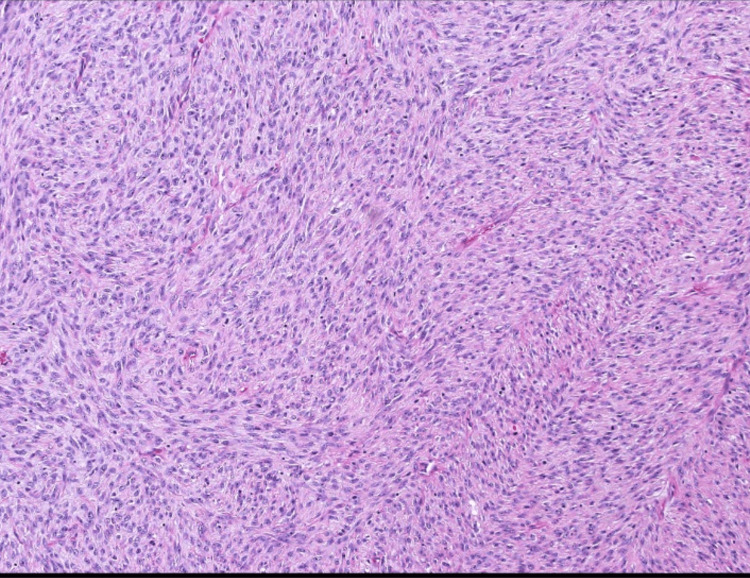 Figure 3
Figure 3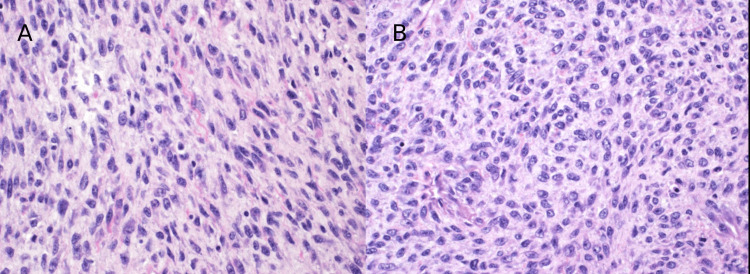 Figure 4
Figure 4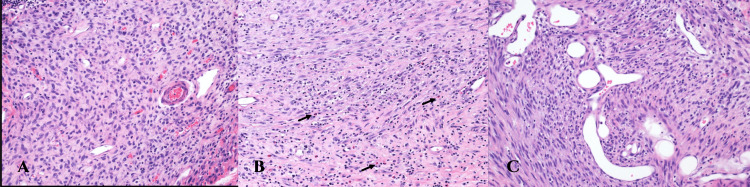 Figure 5
Figure 5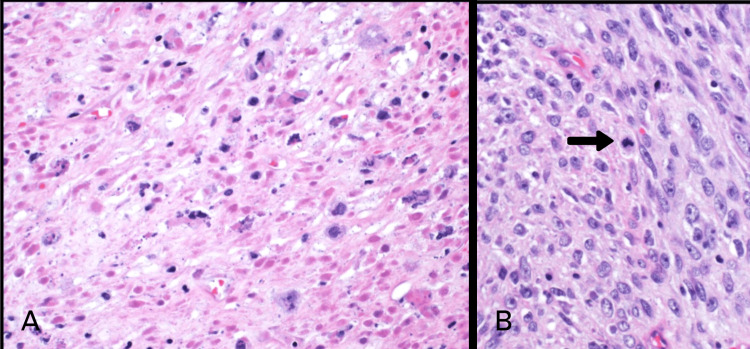 Figure 6
Figure 6Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Neurofibromatosis and Schwannoma Cases · Vascular Tumors and Angiosarcomas
Introduction
Childhood soft-tissue sarcomas are a broad group of cancers that can develop in various anatomic locations, and their cell of origin is typically mesenchymal. Soft tissue tumors are generally uncommon and affect about 7% of the pediatric group [1].
Some pediatric sarcomas exhibit a spindle cell morphology in a fascicular growth pattern, which is a feature of infantile fibrosarcoma (IFS). IFS is a rare primitive fibroblastic neoplasm that most frequently arises in the soft tissues during infancy and early childhood [2]. IFS has a favorable outcome with conservative surgical resection being the preferred therapy and/or cytotoxic chemotherapy [3].
In the last two decades, cytogenetic and molecular analyses have established that the majority of infantile fibrosarcomas harbor a characteristic translocation between chromosomes 12 and 15 which results in the ETV6-NTRK3 gene fusion [4]. Recently, a subset of IFS lacks the* ETV6-NTRK3* fusion and a new spindle cell tumor has been described based on other molecular abnormalities. Next-generation sequencing (NGS) has found a significant number of fusion genes in soft tissue sarcomas [5]. It is now demonstrated that tumors with IFS-like morphology could harbor gene fusions involving additional related kinase genes, such as NTRK1/2, MET, and RET [6]. Novel therapies can target several of these molecular changes, with clinical implications in patients with IFS-like spindle cell sarcomas that have these mutations [7].
BRAF gene fusions are one of these new discoveries with novel fusion partner KIAA1549. In 2018, Kao et al. reported five cases of pediatric spindle cell sarcomas with BRAF gene rearrangement [5]. Penning et al. reported the first case of pediatric spindle cell sarcoma with KIAA1549-BRAF gene fusion in 2021 [8]. Recently, two cases of pediatric spindle cell sarcoma with KIAA1549-BRAF gene rearrangement resembling IFS morphologically were described [9,10]. To our knowledge, this is the fourth case to be reported of spindle cell sarcoma with KIAA1549-BRAF gene fusion in a female child.
Case presentation
A three-year-old girl presented to the orthopedic department with progressive mass swelling in her left thigh for four months as noted by her mother. She had no significant medical or family history. Physical examination revealed a mobile, non-tender, firm mass involving the left lateral distal thigh. MRI imaging showed a 7 cm markedly enhancing, well-defined solid soft tissue mass that abutted the lateral aspect of the lower vastus lateralis muscle (Figure 1A). There was no evidence of local bone invasion or distant metastasis (Figure 1B). She underwent ultrasound-guided biopsy and histopathology showed a spindle cell sarcoma of at least intermediate grade. Later, a wide local resection of the mass was performed and sent for histopathological assessment.
A. Coronal view of MRI shows a well-defined hyper-intense soft tissue mass with marked enhancement at the lateral lower left thigh. B. Axial view of MRI shows no evidence of local bone invasion
On gross examination, the mass appeared well-circumscribed and lobulated with areas of myxoid degeneration. It measured 7.5 x 5 x 4 cm. Scanning power microscopy demonstrated a non-encapsulated densely cellular neoplasm with focal infiltration into adjacent fibroconnective tissue (Figure 2A, 2B). The tumor was composed of monomorphic cells, which were spindle to ovoid in shape and arranged in short intersecting fascicles (Figure 3). On higher magnification, the tumor cells were seen to have uniform nuclei with variable nucleoli embedded in the collagenous stroma (Figure 4A, 4B). In some areas, the tumor cells were arranged haphazardly and contained ectatic/angulated thin-walled blood vessels (Figure 5A, 5C). Focal tumor-infiltrating lymphocytes were noted with occasional eosinophils (Figure 5A, 5B, 5C). Mitotic figures were readily seen (11 per 10 high-power fields) with scattered foci of necrosis (Figure 6A, 6B). By immunohistochemical studies, the tumor cells were focally positive for SMA and negative for S100 protein, CD34, Desmin, EMA, AE1/AE3, Myogenin, and Myod-D1. The fluorescent in situ hybridization (FISH) was negative for the gene rearrangement of ETV6 and SYT. NGS was performed on formalin-fixed, paraffin-embedded tissue and revealed a KIAA1549-BRAF gene fusion.
A. Cellular well-circumscribed neoplasm (H&E x4). B. Focal infiltration into adjacent fibroconnective tissue (arrow) (H&E x10).
Intermediate power view. Areas of high cellularity with spindle cells arranged in short intersecting fascicles (H&E x10).
High power view: The tumor is composed of spindle (A) to more ovoid (B) cells with uniform nuclei and inconspicuous nucleoli in a collagenized stroma (H&E x40).
A. Small thin-walled vascular channels with chronic inflammatory infiltrate composed of lymphocytes. (B) Occasional eosinophils (arrow). (C) Markedly dilated and irregular blood vessels (H&E x40).
A. Foci of necrosis. B. Mitotic figures easily identified (arrow) (H&E x40).
No further treatment or chemotherapy was given after the surgery. Follow-up data showed no evidence of local recurrence or distant metastasis for up to three years after complete surgical resection of the mass.
Discussion
Infantile fibrosarcoma is a locally aggressive, infrequently metastatic tumor that accounts for approximately 5%-10% of all diagnosed sarcomas [11]. Novel pediatric fusion-positive sarcomas have been described in recent literature, including BRAF [8]. Due to the rarity and heterogeneity of pediatric sarcomas, an accurate diagnosis and effective treatments may be provided by the identification of genomic profile. Before RNA sequencing by NGS, the KIAA1549-BRAF fusion-positive tumor was challenging to diagnose. Here, we present a case of pediatric spindle cell sarcoma with KIAA1549-BRAF gene fusions and morphologically overlapping with IFS.
The histopathologic criteria to diagnose IFS usually include infiltrative growth of monomorphic spindle cells composed of mitotically active, fibroblastic spindle cells arranged in cellular sheets and fascicles, with variable lymphocytic infiltrate and hemangiopericytoma-like vascular pattern [3]. Our patient with KIAA1549-BRAF spindle cell sarcoma had heterogenous features found in IFS which made the diagnosis more difficult. Another histologic finding in KIAA1549-BRAF rearranged sarcoma, in contrast to IFS, was evidence of relatively well-circumscribed borders. Therefore, in a child with KIAA1549-BRAF rearranged sarcoma, neither the absence nor the presence of some histologic features found in IFS can be used as a reliable histologic criteria to differentiate these two entities.
Clinically, unlike IFS which commonly involves the extremities, *BRAF-*rearranged sarcomas commonly arise in axial location and have been reported in older children, adolescents, and adults [3,5,7,12]. Our patient with KIAA1549-BRAF spindle cell sarcoma presented with thigh mass which was found in two patients according to previous reports [9,10]. Indeed, only one patient with KIAA1549-BRAF translocation sarcoma in the previous study had evidence of neurofibromatosis type 2, at the time of presentation [10]. In contrast, an adult patient with the same gene fusion has shown a distinct clinical and morphological feature characterized by haphazard spindle cell proliferation with thin-walled vascular channels [7].
Immunohistochemically, the previous cases of spindle cell sarcomas with KIAA1549-BRAF alteration have reported focal expression of Desmin while other markers such as Pan-cytokeratin (AE1/AE3), SMA, Myogenin, CD34, and S100 were all negative [9,10]. Patchy expression of SMA was observed in our case, while other immunostains were negative. The case arising in an adult patient was positive for S100 and CD34 [7]. BRAF V600E immunohistochemistry is sensitive and specific for BRAF V600E mutations in carcinoma and melanoma. However, it is expected to be negative in BRAF-fusion-positive carcinomas and sarcomas. Therefore, immunohistochemical staining for BRAF V600E is not good as a screening marker for fusions involving BRAF [5].
Given the spindle cells appearance of our case and lower limb location, the differential diagnosis includes not only infantile fibrosarcoma but also monophasic synovial sarcoma, spindle cell/ sclerosing rhabdomyosarcoma, malignant peripheral nerve sheath tumor and the emerging entity *NTRK-*rearranged neoplasm with co-expression of S100 and CD34. The combination of our immunohistochemical, genetic, and molecular findings was consistent with a *KIAA1549-BRAF-*rearranged spindle cell sarcoma diagnosis.
BRAF encodes proteins belonging to the RAF family of serine/threonine protein kinases, which have a role in regulating the MAP kinase/ERK signaling pathway and promoting cell survival, proliferation, and transformation [13]. Activating BRAF mutations by fusion and point mutations have been reported in various tumor types, such as thyroid carcinoma and melanoma [14]. A significant number of BRAF-associated gene fusions have emerged more recently as a result of intrachromosomal gene fusion. However, mesenchymal tumors rarely have BRAF gene rearrangements and were recently reported in a subset of spindle cell sarcomas [8]. KIAA1549 is a novel fusion partner for BRAF in soft tissue tumors. *KIAA1549 *is a protein-coding gene belonging to the UPF0606 family. KIAA1549-BRAF translocation commonly occurs in a low-grade pediatric central nervous system tumor [15].
We as well as Fujikawa et al. and Nagy et al. have observed that pediatric KIAA1549-BRAF rearranged sarcoma is usually a localized tumor with indolent biological behavior and generally treated with initial tumor resection and/or chemotherapy [9,10]. There have been no published reports of this tumor metastasizing to other organs or spreading to the lymph nodes, which points to a favorable outcome. However, adult patients with KIAA1549-BRAF fusion tumors show aggressive clinical behavior, such as distant metastases [7].
With the expanding availability of kinase inhibitor therapies, the presence of a BRAF fusion gene has potential therapeutic significance [5]. MEK inhibitors and/or dual MEK/BRAF inhibition are currently used as targeted therapies for tumors with KIAA1549-BRAF fusion and have shown promise in clinical trials [16,17,18]. The use of chemotherapy alone as a therapeutic approach in soft tissue tumors is well-established. In an adult patient, a high-grade spindle cell sarcoma with KIAA1549-BRAF that was resistant to conventional chemotherapies was effectively treated with sorafenib, temsirolimus, and bevacizumab as a combination therapy [7]. In our case, surgical resection showed a good prognosis with no local recurrence. However, more studies are needed to establish the proper management for such cases, including the efficacy of BRAF-targeted therapy, particularly MEK inhibitors for BRAF-altered spindle cell sarcomas that morphologically resemble IFS.
Conclusions
*KIAA1549-BRAF-*rearranged spindle cell sarcoma is a malignant, yet indolent tumor with an IFS-like pattern that is usually composed of spindle cells. The immunohistochemical profile of pediatric *KIAA1549-BRAF-*rearranged spindle cell sarcoma is rather nonspecific, with only a focal expression of SMA or Desmin. For *ETV6-NTRK3-*negative spindle cell sarcomas that morphologically resemble IFS, the confirmation of genomic profile by NGS may help us make an accurate diagnosis and select novel therapeutic options. Future studies are needed to determine the effectiveness of BRAF-targeted therapy in theses sarcomas.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer Incidence and Survival Among Children and Adolescents: United States SEER program National Cancer Bethesda, MD National Cancer Institute 1999
- 2Uncommon and peculiar soft tissue sarcomas: multidisciplinary review and practical recommendations. Spanish Group for Sarcoma research (GEIS -GROUP). Part II Cancer Treat Rev Martínez-Trufero J Cruz Jurado J Hernández-León CN 1022609920213434015910.1016/j.ctrv.2021.102260 · doi ↗ · pubmed ↗
- 3New advances in the molecular classification of pediatric mesenchymal tumors Genes Chromosomes Cancer Suurmeijer AJ Kao YC Antonescu CR 1001105820193018798510.1002/gcc.22681 PMC 6855396 · doi ↗ · pubmed ↗
- 4Molecular detection of the ETV 6-NTRK 3 gene fusion differentiates congenital fibrosarcoma from other childhood spindle cell tumors Am J Surg Pathol Bourgeois JM Knezevich SR Mathers JA Sorensen PH 9379462420001089581610.1097/00000478-200007000-00005 · doi ↗ · pubmed ↗
- 5Recurrent BRAF gene fusions in a subset of pediatric spindle cell sarcomas: expanding the genetic spectrum of tumors with overlapping features with infantile fibrosarcoma Am J Surg Pathol Kao YC Fletcher CD Alaggio R 28384220182887706210.1097/PAS.0000000000000938 PMC 5730460 · doi ↗ · pubmed ↗
- 6Emerging soft tissue tumors with kinase fusions: an overview of the recent literature with an emphasis on diagnostic criteria Genes Chromosomes Cancer Antonescu CR 4374445920203224301910.1002/gcc.22846 PMC 8323076 · doi ↗ · pubmed ↗
- 7Targeted therapy by combined inhibition of the RAF and m TOR kinases in malignant spindle cell neoplasm harboring the KIAA 1549-BRAF fusion protein J Hematol Oncol Subbiah V Westin SN Wang K 8720142442267210.1186/1756-8722-7-8PMC 3896681 · doi ↗ · pubmed ↗
- 8Novel BRAF gene fusions and activating point mutations in spindle cell sarcomas with histologic overlap with infantile fibrosarcoma Mod Pathol Penning AJ Al-Ibraheemi A Michal M 153015403420213385030210.1038/s 41379-021-00806-w · doi ↗ · pubmed ↗