Trend in overall survival from the start of first-line chemotherapy in patients with metastatic urothelial carcinoma
Shoma Yamamoto, Minoru Kato, Taisuke Matsue, Nao Yukimatsu, Yuji Takeyama, Taiyo Otoshi, Takeshi Yamasaki, Katsuyuki Kuratsukuri, Junji Uchida

TL;DR
The study finds that newer treatments for advanced bladder cancer improve patient survival over time.
Contribution
The study identifies a survival trend linked to newer therapies in metastatic urothelial carcinoma.
Findings
Newer agents like pembrolizumab and enfortumab vedotin prolonged overall survival from first-line therapy.
Sequential treatment with these agents in real-world practice is associated with improved survival.
Overall survival has increased over time since the initiation of first-line therapy.
Abstract
New approaches involving immune checkpoint inhibitors and antibody-drug conjugates prolong overall survival in patients with metastatic urothelial carcinoma. However, the access to such systemic therapy in clinical practice is suboptimal, and whether these agents improve overall survival in patients with metastatic urothelial carcinoma over time remains unclear. Hence, we investigated the overall survival trend from the initiation of first-line therapy with these agents to identify changes due to the medication and time of treatment initiation. We retrospectively evaluated 195 patients from a single center. They were treated with chemotherapy, pembrolizumab, or avelumab or enfortumab vedotin. The treatment was categorized into chemotherapy, pembrolizumab or avelumab/enfortumab vedotin period. The new agents prolonged overall survival from the start of first-line therapy. Furthermore,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
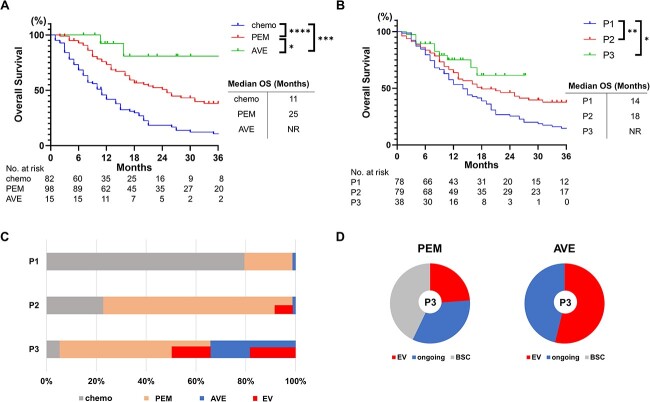 Figure 1
Figure 1| Characteristics ( | Number of patients | ||||
|---|---|---|---|---|---|
| Chemotherapy ( | Pembrolizumab ( | Avelumab ( |
| ||
| Sex (%) | Male | 64 (78) | 67 (68) | 10 (67) | 0.3 |
| Female | 18 (12) | 31 (32) | 5 (33) | ||
| Age, years | Median (range) | 73 (32–95) | 73 (37–86) | 70 (56–84) | 0.51 |
| EOCG PS (%) | 0 | 66 (80) | 70 (71) | 15 (100) | 0.03* |
| ≥1 | 16 (20) | 28 (29) | 0 (0) | ||
| Hb (%) | ≥10 g/dL | 69 (84) | 66 (67) | 11 (73) | 0.03* |
| <10 g/dL | 13 (16) | 32 (33) | 4 (27) | ||
| Primary tumor sites (%) | Bladder | 47 (57) | 49 (50) | 8 (53) | 0.39 |
| Upper urinary tract | 34 (41) | 43 (44) | 7 (47) | ||
| Both | 1 (2) | 6 (6) | 0 (0) | ||
| Metastatic site (%) | Lymph node | 44 (54) | 49 (50) | 11 (73) | 0.97 |
| Lung | 34 (41) | 33 (34) | 6 (40) | ||
| Bone | 21 (26) | 21 (21) | 3 (20) | ||
| Liver | 17 (21) | 17 (17) | 2 (13) | ||
| Surgical treatment (%) | Cystectomy | 22 (27) | 31 (32) | 3 (20) | 0.85 |
| Cystectomy+nephroureterectomy | 0 (0) | 2 (2) | 0 (0) | ||
| Nephroureterectomy | 22 (27) | 25 (26) | 5 (33) | ||
| Transurethral resection | 14 (17) | 17 (17) | 2 (13) | ||
| None | 24 (29) | 23 (23) | 5 (33) | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBladder and Urothelial Cancer Treatments · Urinary and Genital Oncology Studies · Cancer Immunotherapy and Biomarkers
Introduction
Cisplatin-based chemotherapy has been the gold standard as the first-line treatment of metastatic urothelial carcinoma (mUC), and a 2000 clinical trial comparing gemcitabine plus cisplatin and methotrexate, vinblastine, doxorubicin, and cisplatin reported the median overall survival (OS) was 14 months (1). Pembrolizumab was approved in November 2017 as second-line therapy for patients showing disease progression after platinum-based chemotherapy, and the 2017 KEYNOTE-045 trial reported that the OS from the initiation of pembrolizumab was 10.3 months (2). Later, maintenance therapy with avelumab prolonged OS in patients who did not show disease progress after platinum-based chemotherapy, and the median OS from the start of maintenance therapy in avelumab-treated patients was 21.4 months (3). Recently, new agents such as enfortumab vedotin (EV), erdafitinib and sacituzumab govitecan have been approved by the US Food and Drug Administration for patients showing disease progression after treatment with immune checkpoint inhibitors (ICIs) (4–6). Ideally, the estimated median OS from the start of first-line therapy would be ~26.5 and 16–18 months, respectively, among avelumab- and pembrolizumab-treated patients (7). However, real-world studies have reported a lack of optimal receipt of systemic therapies (8). This low rate of receipt of subsequent therapy is attributable to the characteristic of rapid disease progression in patients with mUC as well as the healthcare system. In fact, few studies have investigated the effects of new therapeutic agents on OS after the initiation of first-line chemotherapy in real-world settings. In other words, there is a gap between the findings of clinical trials and real-world clinical practice. Hence, this study was aimed at investigating trends in OS and sequential treatment allocation in patients who received first-line platinum-based chemotherapy for mUC.
Patients and methods
Patients with mUC who received first-line platinum-based chemotherapy at the Osaka Metropolitan University Hospital between April 2009 and August 2022 were enrolled. This retrospective, single-center study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of Osaka Metropolitan University Hospital (no. 2021-090, 4105). Overall, 195 patients were evaluated. OS was defined as the time from the start of the first-line chemotherapy and was calculated per the following two aspects: based on the anticancer agent used and on the time when the first-line treatment was initiated to observe the trend in OS so as to identify changes due to the medication and the time of treatment initiation. For the analysis based on the anticancer agent used, the patients were divided into the following three groups: chemotherapy, pembrolizumab and avelumab groups. The chemotherapy group was defined as the group of patients who received only chemotherapy during treatment. The pembrolizumab and avelumab groups were defined as the groups of patients who received any of these agents during treatment. The time of first-line chemotherapy initiation was classified into the following three periods based on regulatory approval in Japan: chemotherapy period (April 2009–June 2017; P1), pembrolizumab period (July 2017–December 2020; P2) and avelumab and EV period (January 2021–August 2022; P3). The last observation date was set for the end of July 2023. The patients’ data were statistically analyzed using GraphPad Prism version 9 (GraphPad Software, Inc., San Diego, CA, USA). OS was calculated using the Kaplan–Meier method, and the log-rank test was used to determine differences. Fisher's exact test or chi-square test was used to compare categorical variables. A P value of <0.05 was considered statistically significant.
Results
Patients’ backgrounds
The chemotherapy, pembrolizumab and avelumab included 82, 98 and 15 patients, respectively. In the analysis based on the time of initiation of the first-line therapy, the P1, P2 and P3 groups included 78, 79 and 38 patients, respectively. The distribution of clinical parameters was well-balanced in categories such as sex, age, anemia, tumor origin, metastatic sites and radical surgery, except for Eastern Cooperative Oncology Group Performance Status (ECOG PS) (Table 1). The avelumab group had better ECOG PS than the remaining groups.
Patients’ survival
A significant difference in OS was observed between pembrolizumab- and chemotherapy-treated patients [hazard ratio (HR) = 0.44, 95% confidence interval (CI): 0.31–0.63, P < 0.0001], avelumab- and chemotherapy-treated patients (HR = 0.11, 95% CI: 0.062–0.19, P = 0.0001) and avelumab- and pembrolizumab-treated patients (HR = 0.26, 95% CI: 0.12–0.56, P = 0.037) (Fig. 1A).
*Trends in OS by anticancer agent (A) and period (B). EV is used for some patients in the PEM and AVE group. (C) The proportion of therapeutic agents in each period. (D) Treatment breakdown in the patients who received PEM or AVE in P3 at the time of data cutoff. Patients were either treated with EV, best supportive care, or continued ICI treatment (ongoing). OS, overall survival; ICI, immune checkpoint inhibitor; chemo, chemotherapy; PEM, pembrolizumab; AVE, avelumab; EV, enfortumab vedotin; BSC, best supportive care; NR, not reached; chemotherapy period (P1: April 2009–June 2017), PEM period (P2: July 2017–December 2020), AVE and EV period (P3: January 2021–August 2022), *P < 0.05; **P < 0.01; ***P < 0.001; ***P < 0.0001.
Analysis by periods showed that OS was significantly prolonged in P2 compared with that in P1 (HR = 0.62, 95% CI: 0.43–0.89, P = 0.009) and in P3 compared with that in P1 (HR = 0.47, 95% CI: 0.28–0.78, P = 0.015). However, no difference was observed in OS between P2 and P3 (HR = 0.66, 95% CI: 0.36–1.20, P = 0.21) (Fig. 1B). In P1, the majority of patients (80%) belonged to the chemotherapy group (including those who received second-line taxane-based chemotherapy but not ICIs or EV), and the majority of patients received ICIs (pembrolizumab and avelumab) in P2 and P3 (77 and 95%, respectively). Overall, the proportion of patients who received ICIs increased over time, as shown in Fig. 1C (P = 0.005). In P3, when third-line treatment with EV was available, EV was administered to 24% of the pembrolizumab-treated patients and 54% of the avelumab-treated patients (Fig. 1C). Importantly, all the patients in avelumab group with disease progression received EV, while 43% of patients in the pembrolizumab group received best supportive care in P3 (Fig. 1D). We believe this gap in sequential treatment is due to the difference in tumor characteristics between those who received pembrolizumab and avelumab.
Discussion
While a pivotal study has shown that new agents prolonged OS compared with the standard of care in patients with mUC who were eligible for clinical trials, it is important to determine whether this advantage could be obtained in real-world practice in the patients including those ineligible for clinical trials due to a deteriorated PS, rapid disease progression and other reasons. Although the therapeutic benefit of pembrolizumab can be expected irrespective of the objective response and number of cycles of first-line chemotherapy (9), we have previously shown that excessive cycles of first-line chemotherapy may not lead to improved OS, especially in the era of switching maintenance therapies and EV (10). In the present study, the transition rate of ICI treatment increased over time, while the prevalence of the treatment with EV was only 24% in the pembrolizumab group in P3, and 43% of patients received best supportive care. In addition, no significant prolongation in OS was observed between P2 and P3. This unexpected result might be because some patients who received ICIs (especially pembrolizumab) could not receive EV owing to rapid disease progression or other reasons. With the current access to EV as a sequential treatment, it is clinically important not to miss the opportunity for sequential treatment, except for patients who cannot continue the treatment owing to their declining general condition. Many clinical trials to investigate the benefit of combination therapy using ICIs vs platinum-based chemotherapy are ongoing. If the primary endpoints of these trials are achieved, the results of this study, especially the OS in P3, will have important implications as results achieved in a historical cohort in real-world clinical practice when new first-line therapies are approved in the future.
This study was limited by its retrospective nature, the small number of cases in a single institution and immortal time bias. Study limitations also include the lack of a multivariate analysis to minimize variation among the patients owing to the sample size. Prognostic factors such as anemia and poor PS may influence the feasibility of sequential therapy. However, this study showed an improvement in OS in patients with mUC treated with new treatment agents and because of the current prevalence of sequential treatment in real-world practice. This might be because that the ICI contributed to better access to the second-line therapy. The results in the present study may indicate the importance of not missing the appropriate opportunity to receive sequential treatments for mUC.
Abbreviations & Acronyms
mUC: metastatic urothelial carcinoma
OS: overall survival
EV: enfortumab vedotin
ICIs: immune checkpoint inhibitors
ECOG PS: Eastern Cooperative Oncology Group Performance Status
HR: hazard ratio
CI: confidence interval
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1von der Maase H, Hansen SW, Roberts JT, et al. Gemcitabine and cisplatin versus methotrexate, vinblastine, doxorubicin, and cisplatin in advanced or metastatic bladder cancer: results of a large, randomized, multinational, multicenter, phase III study. J Clin Oncol Off J Am Soc Clin Oncol 2000;18:3068–77.10.1200/JCO.2000.18.17.306811001674 · doi ↗ · pubmed ↗
- 2Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med 2017;376:1015–26.28212060 10.1056/NEJ Moa 1613683 PMC 5635424 · doi ↗ · pubmed ↗
- 3Powles T, Park SH, Voog E, et al. Avelumab maintenance therapy for advanced or metastatic urothelial carcinoma. N Engl J Med 2020;383:1218–30.32945632 10.1056/NEJ Moa 2002788 · doi ↗ · pubmed ↗
- 4Powles T, Rosenberg JE, Sonpavde GP, et al. Enfortumab vedotin in previously treated advanced urothelial carcinoma. N Engl J Med 2021;384:1125–35.33577729 10.1056/NEJ Moa 2035807 PMC 8450892 · doi ↗ · pubmed ↗
- 5Loriot Y, Necchi A, Park SH, et al. Erdafitinib in locally advanced or metastatic urothelial carcinoma. N Engl J Med 2019;381:338–48.31340094 10.1056/NEJ Moa 1817323 · doi ↗ · pubmed ↗
- 6Tagawa ST, Balar AV, Petrylak DP, et al. TROPHY-U-01: a phase II open-label study of sacituzumab govitecan in patients with metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors. J Clin Oncol 2021;39:2474–85.33929895 10.1200/JCO.20.03489 PMC 8315301 · doi ↗ · pubmed ↗
- 7Grivas P, Agarwal N, Pal S, et al. Avelumab first-line maintenance in locally advanced or metastatic urothelial carcinoma: applying clinical trial findings to clinical practice. Cancer Treat Rev 2021;97:102187.33839438 10.1016/j.ctrv.2021.102187 · doi ↗ · pubmed ↗
- 8Swami U, Grivas P, Pal SK, Agarwal N. Utilization of systemic therapy for treatment of advanced urothelial carcinoma: lessons from real world experience. Cancer Treat Res Commun 2021;27:100325.33549986 10.1016/j.ctarc.2021.100325 · doi ↗ · pubmed ↗