A cystic shaped metastatic osteosarcoma in heart: an unusual view
Mustafa Ucar, Ali Yasar Kilinc

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
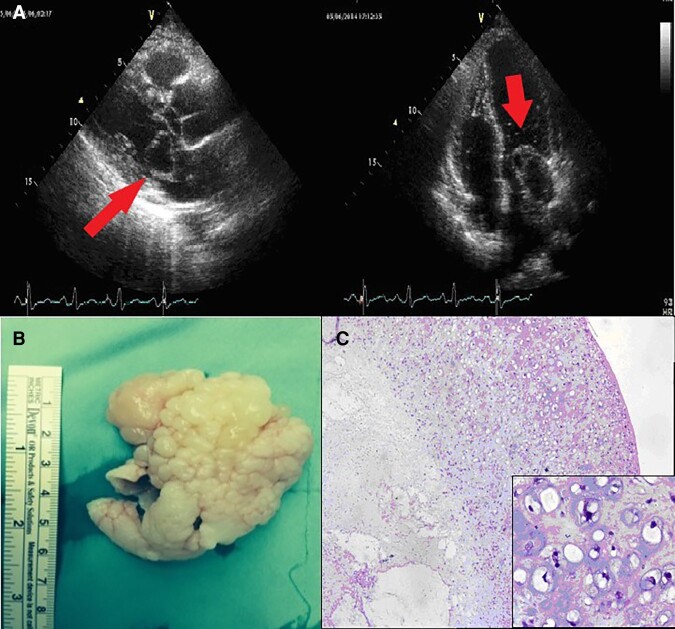 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac tumors and thrombi · Sarcoma Diagnosis and Treatment · Vascular Tumors and Angiosarcomas
Case description
A 32-year-old man was admitted to the hospital complaining of palpitation and dsypnea for 2 weeks. He had a past history of mandibular tumour 8 years ago which was diagnosed as ‘Osteosarcoma, chondroblastic type’ and received chemotherapy after surgical resection. On admission his vital signs were normal. He had a diastolic murmur at the left sternal border. Transthoracic echocardiography revealed a multilocular cystic mass originating from the left superior pulmonary vein in left atrium that prolapsing left ventricle at diastolic period (Figure 1A). There was a 19 mmHg peak gradient and a 10 mmHg mean gradient across the mitral valve. The patient underwent a minimal invasive operation for the excision of mass. On gross examination, 6 × 4.5 × 3 cm sized cauliflower-shaped creamy mass with myxoid cut surface was defined (Figure 1B). Microscopically, tumour was composed of spindle and round tumour cells that lie in the lacunae and form lobules within an abundant extracellular chondroid matrix. The centre of the tumour had necrosis and towards the periphery tumour became hypercellular. Severe cytological atypia and mitotic figures were observed. By these findings, the patient was diagnosed as ‘Malignant mesenchymal tumour with chondroid differentiation’ and considered as ‘Cardiac metastasis of osteosarcoma, chondroblastic type’ (Figure 1C).
(A) Cystic mass was originating from the left superior pulmonary vein and prolapsing to the left ventricle (red arrow). (B) Grossly, cauliflower-shaped mass with myxoid appearance was seen. (C) Tumour was composed of hyperchromatic cells within the chondroid matrix which formed lobules. The centre of the tumour had necrosis. Tumor cells lie in the lacunae and have severe atypia (inset).
Most frequent malignant cardiac tumours are sarcomas.^1^ Metastatic sarcomas to the heart are more likely to involve the myocardium. In only 5% of cases, endocardium or chamber cavities are involved, as in our patient. All types of sarcomas are known to metastasize and evidently, this occurs via the haematogenous route.^2^ Generally, metastatic tumour is a relative contraindication for surgery. In this case, we preferred to perform surgery, because the mass was mimicking mitral stenosis by prolapsing through the mitral valve during diastole and a mass in the cardiac cavity can embolize. According to our knowledge, this case seems to be the first cystic-shaped osteosarcoma metastasis on transthoracic echocardiography.
Consent: The authors confirm that written consent for submission and publication of this case report including images and associated text has been obtained from the patient in line with COPE guidance.
Funding: None declared.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sutsch G, Jenni R, von Segesser L, Schneider J. Heart tumors: incidence, distribution, diagnosis. Exemplified by 20,305 echocardiographies. Schweiz Med Wochenschr 1991;121:621–629.2047823 · pubmed ↗
- 2Silver MD, Gotlieb AI, Schoen FJ. Cardiovascular Pathology. 3rd ed. New York: Churchill Livingstone Company; 2001. p 600–601.