Wave-Based Outcomes Comparison of Hospitalized COVID-19 Patients: A Retrospective Multicenter Cohort Study From Rural Appalachia
Sandhya Kolagatla, Joshua K Jenkins, Joseph Elsoueidi, Lauren Wisnieski, Nagabhishek Moka

TL;DR
This study compares outcomes of hospitalized COVID-19 patients in rural Appalachia across pandemic waves, highlighting disparities and the impact of vaccination.
Contribution
The first study to analyze wave-based outcomes of hospitalized COVID-19 patients in rural Appalachia.
Findings
The second wave had the highest mortality, particularly affecting younger patients.
Elderly and patients with chronic conditions had the highest mortality and need for ventilation.
Vaccination reduced the odds of ICU stay and mechanical ventilation.
Abstract
Background: There has been little to no characterization of the pandemic’s effects on rural Central Appalachia, in which health disparities in the pre-COVID-19 era have historically plagued. This is the first study to compare wave-based differences in outcomes of hospitalized patients with COVID-19 in the rural Appalachian region. This study aims to provide a more comprehensive understanding of the effects of the COVID-19 pandemic on large rural communities and Appalachia. Methods: This is a retrospective cohort study of hospitalized patients with COVID-19 between April 2020 and June 2022, which includes 13 Appalachian Regional Healthcare (ARH) hospitals. The primary outcome of the study was in-hospital mortality. Secondary outcomes included intensive care unit (ICU) stay, need for mechanical ventilation, length of hospital stay, 1-30-day re-admittance, 30-60-day re-admittance, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
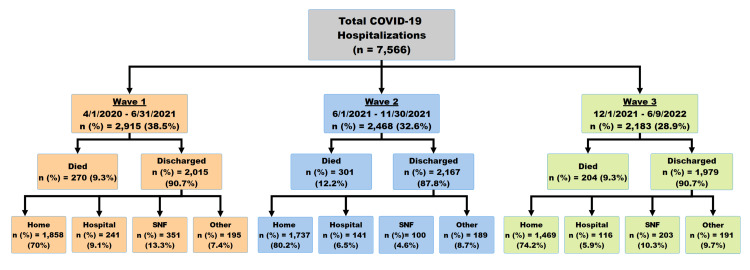 Figure 1
Figure 1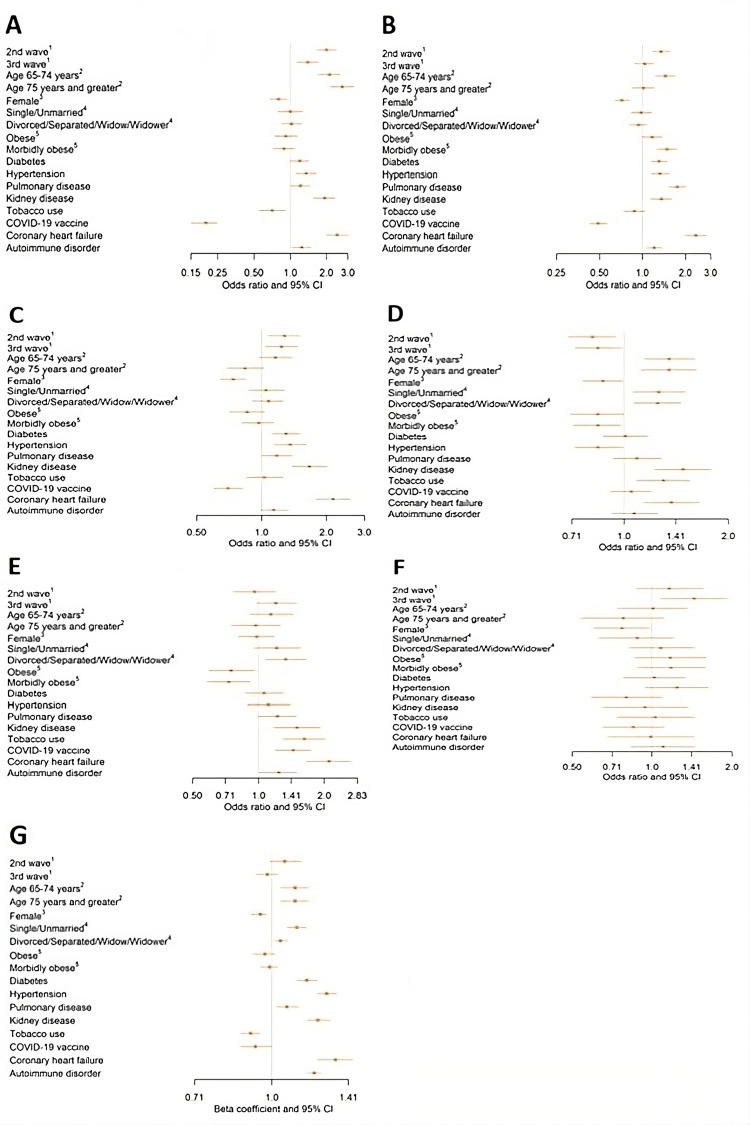 Figure 2
Figure 2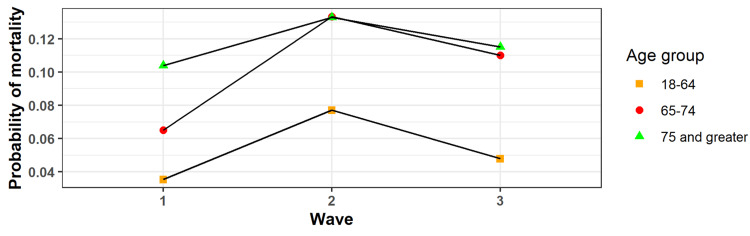 Figure 3
Figure 3| Wave 1 (n=2,915) | Wave 2 (n=2,468) | Wave 3 (n=2,183) | Total (n=7,566) | |||||||
| Characteristic | n | % (within row) | n | % (within row) | n | % (within row) | n | % (of total) | p-Value | |
| Demographics | ||||||||||
| Age (years) | 18 to 39 | 238 | 29.13 | 340 | 41.62 | 239 | 29.25 | 817 | 10.8 | <0.001 |
| 40 to 49 | 310 | 35.35 | 349 | 39.79 | 218 | 24.86 | 877 | 11.59 | - | |
| 50 to 64 | 766 | 35.04 | 794 | 36.32 | 626 | 28.64 | 2,186 | 28.89 | - | |
| 65 to 74 | 762 | 40.55 | 558 | 29.7 | 559 | 29.75 | 1,879 | 24.83 | - | |
| 74 and older | 839 | 46.43 | 427 | 23.63 | 541 | 29.94 | 1,807 | 23.88 | - | |
| Marital status | Married | 1,443 | 40.31 | 1,204 | 33.63 | 933 | 26.06 | 3,580 | 47.77 | <0.001 |
| Single | 546 | 35.09 | 534 | 34.32 | 476 | 30.59 | 1,556 | 20.76 | - | |
| Divorced/separated/widowed | 897 | 38.02 | 708 | 30.01 | 754 | 31.96 | 2,359 | 31.47 | <0.001 | |
| Gender | Male | 1,480 | 40.36 | 1,202 | 32.78 | 985 | 26.86 | 3,667 | 48.47 | - |
| Female | 1,435 | 36.8 | 1,266 | 32.47 | 1,198 | 30.73 | 3,899 | 51.53 | - | |
| Insurance | Medicaid/Medicare | 2,313 | 37.73 | 1,967 | 32.09 | 1,850 | 30.18 | 6,130 | 81.02 | <0.001 |
| Other | 602 | 41.92 | 501 | 34.89 | 333 | 23.19 | 1,436 | 18.98 | - | |
| Comorbidities | ||||||||||
| Weight status | Underweight | 85 | 33.46 | 66 | 25.98 | 103 | 40.55 | 254 | 3.5 | <0.001 |
| Normal weight | 500 | 35.46 | 443 | 31.42 | 467 | 33.12 | 1,410 | 19.41 | - | |
| Overweight | 747 | 38.91 | 606 | 31.56 | 567 | 29.53 | 1,920 | 26.42 | - | |
| Obese | 570 | 38.2 | 517 | 34.65 | 405 | 27.14 | 1,492 | 20.53 | - | |
| Morbidly obese | 882 | 40.27 | 753 | 34.38 | 555 | 25.34 | 2,190 | 30.14 | - | |
| Diabetes | No | 1,807 | 36.68 | 1,651 | 33.51 | 1,469 | 29.82 | 4,927 | 65.12 | <0.001 |
| Yes | 1,108 | 41.99 | 817 | 30.96 | 714 | 27.06 | 2,639 | 34.88 | - | |
| Hypertension | No | 1,829 | 37.69 | 1,533 | 31.59 | 1,491 | 30.72 | 4,853 | 64.14 | <0.001 |
| Yes | 1,086 | 40.03 | 935 | 34.46 | 692 | 25.51 | 2,713 | 35.86 | - | |
| Hepatitis | No | 410 | 38.68 | 342 | 32.26 | 308 | 29.06 | 1060 | 91.7 | 0.03 |
| Yes | 26 | 27.08 | 43 | 44.79 | 27 | 28.13 | 96 | 8.3 | - | |
| Pulmonary disease | No | 2,842 | 38.79 | 2,380 | 32.49 | 2,104 | 28.72 | 7,326 | 96.83 | 0.03 |
| Yes | 73 | 30.42 | 88 | 36.67 | 79 | 32.92 | 240 | 3.17 | - | |
| Kidney disease | No | 2,354 | 37.67 | 2,130 | 34.09 | 1,765 | 28.24 | 6,249 | 82.59 | <0.001 |
| Yes | 561 | 42.6 | 338 | 25.66 | 418 | 31.74 | 1,317 | 17.41 | - | |
| Kidney failure | No | 2,211 | 39.3 | 1,830 | 32.53 | 1,585 | 28.17 | 5,626 | 74.36 | 0.03 |
| Yes | 704 | 36.29 | 638 | 32.89 | 598 | 30.82 | 1,940 | 25.64 | - | |
| Malignancy | No | 2,799 | 38.41 | 2,391 | 32.81 | 2,097 | 28.78 | 7,287 | 96.31 | 0.19 |
| Yes | 116 | 41.58 | 77 | 27.6 | 86 | 30.82 | 279 | 279 | - | |
| Acute respiratory failure | No | 1,744 | 40.13 | 1,281 | 29.48 | 1,321 | 30.4 | 4,346 | 57.44 | <0.001 |
| Yes | 1,171 | 36.37 | 1,187 | 36.86 | 862 | 26.77 | 3,220 | 42.56 | - | |
| CHF | No | 2,404 | 38.37 | 2,107 | 33.63 | 1,754 | 28 | 6,265 | 82.8 | <0.001 |
| Yes | 511 | 39.28 | 361 | 27.75 | 429 | 32.97 | 1,301 | 17.2 | - | |
| Dementia | No | 2,691 | 37.72 | 2,387 | 33.45 | 2,057 | 28.83 | 7,135 | 94.3 | <0.001 |
| Yes | 224 | 51.97 | 81 | 18.79 | 126 | 29.23 | 431 | 5.7 | - | |
| Osteoarthritis | No | 2,617 | 38.03 | 2,272 | 33.01 | 1,993 | 28.96 | 6,882 | 90.96 | 0.01 |
| Yes | 298 | 43.57 | 196 | 28.65 | 190 | 27.78 | 684 | 9.04 | - | |
| Obstructive pulmonary disease | No | 2,178 | 38.03 | 1,918 | 33.49 | 1,631 | 28.48 | 5,727 | 75.69 | 0.02 |
| Yes | 737 | 40.08 | 550 | 29.91 | 552 | 30.02 | 1,839 | 24.31 | - | |
| Pulmonary embolism | No | 2,888 | 38.56 | 2,453 | 32.75 | 2,148 | 28.68 | 7,489 | 98.98 | 0.003 |
| Yes | 27 | 35.06 | 15 | 19.48 | 35 | 45.45 | 77 | 1.02 | - | |
| Lipidemia | No | 1,937 | 36.73 | 1,780 | 33.75 | 1,557 | 29.52 | 5,274 | 69.71 | <0.001 |
| Yes | 978 | 42.67 | 688 | 30.02 | 626 | 27.31 | 2,292 | 30.29 | - | |
| History of TIA and cerebral infarction | No | 2,756 | 38.53 | 2,345 | 32.79 | 2,051 | 28.68 | 7,152 | 94.53 | 0.28 |
| Yes | 159 | 38.41 | 123 | 29.71 | 132 | 31.88 | 414 | 5.47 | - | |
| Severe sepsis with shock | No | 2,784 | 38.58 | 2,371 | 32.86 | 2,061 | 28.56 | 7,216 | 95.37 | 0.03 |
| Yes | 131 | 37.43 | 97 | 27.71 | 122 | 34.86 | 350 | 4.63 | - | |
| Autoimmune disorder | No | 2,122 | 37.59 | 1,891 | 33.5 | 1,632 | 28.91 | 5,645 | 74.61 | 0.01 |
| Yes | 793 | 41.28 | 577 | 30.04 | 551 | 28.68 | 1,921 | 25.39 | - | |
| Tobacco use | No | 2,551 | 40.63 | 2,020 | 32.18 | 1,707 | 27.19 | 6,278 | 82.98 | <0.001 |
| Yes | 364 | 28.26 | 448 | 34.78 | 476 | 36.96 | 1,288 | 17.02 | - | |
| Long-term opiate use | No | 2,801 | 38.65 | 2,359 | 32.55 | 2,087 | 28.8 | 7,247 | 95.78 | 0.58 |
| Yes | 114 | 35.74 | 109 | 34.17 | 96 | 30.09 | 319 | 4.22 | - | |
| COVID-19 vaccination | No | 1,903 | 37.45 | 1,839 | 36.19 | 1,339 | 26.35 | 5,081 | 67.16 | <0.001 |
| Yes | 1,012 | 40.72 | 629 | 25.31 | 844 | 33.96 | 2,485 | 32.84 | - | |
| Outcomes | ||||||||||
| ICU | No | 2,537 | 38.99 | 2,105 | 32.35 | 1,864 | 28.65 | 6,506 | 85.99 | 0.12 |
| Yes | 378 | 35.66 | 363 | 34.25 | 319 | 30.09 | 1,060 | 14.01 | - | |
| Mortality | No | 2,645 | 38.95 | 2,167 | 31.91 | 1,979 | 29.14 | 6,791 | 89.76 | <0.001 |
| Yes | 270 | 34.84 | 301 | 38.84 | 204 | 26.32 | 775 | 10.24 | - | |
| 1-30-day re-admit | No | 2,132 | 38.21 | 1,822 | 32.66 | 1,625 | 29.13 | 5,579 | 82.15 | 0.01 |
| Yes | 513 | 42.33 | 345 | 28.47 | 354 | 29.21 | 1,212 | 17.85 | - | |
| 31-60-day re-admit | No | 2,434 | 39.13 | 2,008 | 32.28 | 1,778 | 28.59 | 6,220 | 91.59 | 0.003 |
| Yes | 211 | 36.95 | 159 | 27.85 | 201 | 35.2 | 571 | 8.41 | - | |
| Mechanical ventilation | No | 2,367 | 38.82 | 1,926 | 31.59 | 1,804 | 29.59 | 6,097 | 80.58 | <0.001 |
| Yes | 548 | 37.3 | 542 | 36.9 | 379 | 25.8 | 1,469 | 19.42 | - | |
| Clot risk | No | 2,819 | 38.79 | 2,369 | 32.6 | 2,079 | 28.61 | 7,267 | 96.05 | 0.03 |
| Yes | 96 | 32.11 | 99 | 33.11 | 104 | 34.78 | 299 | 3.95 | - | |
| Unadjusted OR (95% CI) | Adjusted OR (95% CI)1 | |
| Mortality | ||
| Wave 1 (reference) | 1 | 1 |
| Wave 2 | 1.40 (1.18-1.67)* | 2.00 (1.64-2.44)* |
| Wave 3 | 1.05 (0.87-1.27)* | 1.40 (1.13-1.73)* |
| Mechanical ventilation | ||
| Wave 1 (reference) | 1 | 1 |
| Wave 2 | 1.24 (1.08-1.42)* | 1.35 (1.17-1.56)* |
| Wave 3 | 0.92 (0.80-1.07) | 1.04 (0.88-1.21) |
| ICU stay | ||
| Wave 1 (reference) | 1 | 1 |
| Wave 2 | 1.20 (1.03-1.41)* | 1.28 (1.08-1.51)* |
| Wave 3 | 1.19 (1.01-1.40)* | 1.24 (1.04-1.48)* |
| 1-30 d readmittance | ||
| Wave 1 (reference) | 1 | 1 |
| Wave 2 | 0.77 (0.66-0.89)* | 0.81 (0.69-0.95)* |
| Wave 3 | 0.90 (0.77-1.05) | 0.84 (0.72-0.98)* |
| 31-60 d readmittance | ||
| Wave 1 (reference) | 1 | 1 |
| Wave 2 | 0.91 (0.74-1.13) | 0.96 (0.77-1.20) |
| Wave 3 | 1.32 (1.08-1.62)* | 1.20 (0.97-1.49) |
| Clot risk | ||
| Wave 1 (reference) | 1 | 1 |
| Wave 2 | 1.25 (0.94-1.67) | 1.16 (0.87-1.56) |
| Wave 3 | 1.43 (1.08-1.90)* | 1.44 (1.07-1.92)* |
| Length of stay in days2 | ||
| Wave 1 (reference) | 1 | 1 |
| Wave 2 | 1.00 (0.92-1.09) | 1.06 (0.99-1.03) |
| Wave 3 | 0.93 (0.89-0.98) | 0.98 (0.93-1.03) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · Infection Control and Ventilation · Climate Change and Health Impacts
Introduction
SARS-CoV-2, the virus that caused the coronavirus disease 2019 (COVID-19) pandemic, has resulted in 6.8 million deaths across the globe and 2.9 million deaths in the Americas as of March 21, 2023 [1]. At this point in the pandemic, more than 13 billion COVID-19 vaccine doses have been administered worldwide [1]. Throughout the pandemic, cases and hospitalizations related to COVID-19 surged in waves worldwide. The first wave, which began in March-April 2020, severely disturbed social and economic activities due to high mortality and transmissibility worldwide. The second wave began around July 2020 and led to higher mortality rates than the previous wave, and the third wave around January 2021 brought a new strain (B.1.1.7; Delta) with higher transmission rates and increased the number of re-infections [2].
Throughout these waves of the pandemic, rural communities were disproportionately affected compared to their urban dweller counterparts. The origin of their high-risk status is multifactorial, primarily involving a combination of aging populations, multiple comorbidities, and health-related behaviors. For instance, individuals living in rural America are older, with a median age of 51 years compared to 45 years in urban America [3]. Rural communities also have a larger density of residents aged 65 years or older than urban areas (18.4% compared to 14.5%) [4]. Declining birth rates and migration patterns in younger adults have also increased the density of the rural older population more quickly than in urban settings [5]. Rural Americans are more likely to have comorbid health conditions [6,7], limited access to emergency and intensive care healthcare facilities, and live further from healthcare facilities compared to individuals in urban settings [8]. There is also a shortage of healthcare providers in rural America [9]. Health behaviors also put rural populations at risk with higher rates of cigarette smoking, obesity, and physical inactivity compared to more urban populations [10].
Central Appalachia is a unique rural community that endured a significant impact during each wave of the pandemic, regardless of dominant strain, resulting in significant morbidity and mortality. We performed a multicenter retrospective cohort study to evaluate the differences in mortality and morbidity of hospitalized COVID-19 patients in a wave-based distribution. This is the first study in the literature that evaluates wave-based outcomes of hospitalized patients in Central Appalachia.
Materials and methods
This is a multicenter, retrospective, three-arm cohort study of hospitalized patients with COVID-19 between April 2020 and June 2022, which aims to compare the differences in wave-based outcomes in hospitalized COVID patients. The Appalachian Regional Healthcare (ARH) Institutional Review Board (IRB) approved this study. As per IRB, written consent was waived for this study.
As this is a retrospective study, the data was extracted from electronic medical records (EMRs). Data was extracted from 13 ARH hospitals located in eastern Kentucky and West Virginia. We queried the EMR database for comorbid conditions using the International Classification of Diseases, 10th Revision (ICD-10) master codes. Stata version 17.0 (StataCorp, College Station, TX) was used for all statistical analyses. Bar charts and forest plots were created using the "ggplot2" and "forestplot" packages from R version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria), respectively [11,12].
Three waves of COVID-19 were defined based on visually assessing a histogram of cases in the hospital system during the study period. The first wave was defined from April 2020 to May 2021, the second wave was defined from June 2021 to November 2021, and the third wave was defined from December 2021 to June 2022. The primary outcome of the study was in-hospital mortality, whereas the secondary outcomes included intensive care unit (ICU) stay, need for mechanical ventilation, length of hospital stay (LOS), 1-30-day re-admittance, 30-60-day re-admittance, and thromboembolism incidence risk.
Data analysis
Descriptive and chi-square analyses were used to compare demographic characteristics, comorbidities, and discharge status between waves. Analysis of variance (ANOVA) was used to compare the age and body mass index (BMI) of patients between waves.
Outcomes among COVID-19 patients between the three waves were compared using adjusted and unadjusted regression models. Mixed-effects logistic regression using the "melogit" command in Stata was used to model mortality, ICU stay, mechanical ventilation, 1-30-day re-admittance, 31-60 day re-admittance, and thromboembolism risk. Mixed linear regression using the "xtmixed" command in Stata was used to model LOS. A random intercept for hospital (N=13) was included in all models. Adjusted analyses were adjusted for age, gender, marital status, obesity status, diabetes, hypertension, pulmonary disease, chronic kidney disease, autoimmune disease, coronary heart disease, and tobacco use. An interaction term between age category and wave was assessed in each model to determine if trends in the likelihood of different outcomes changed across each age category between the three waves.
Normality and homoskedasticity of residuals were assessed using residual plots (i.e., histograms and quantile-quantile [Q-Q] plots) for mixed linear regression models and ANOVA tests. LOS and BMI were transformed by the logarithm function to meet normality requirements. All model results for the transformed variables were back-transformed to improve interpretability.
Results
In total, data from 7,572 patients was downloaded from the EMR database. Six records were missing discharge data and were removed, leaving a total of 7,566 records (Figure 1). There was missing data at the patient level for BMI (n=300) and marital status (n=71).
Summary of patients hospitalized with COVID-19 during the COVID-19 pandemic.
Patients in wave 2 had a higher mortality rate (12.2%) compared with those in wave 1 (9.3%) and wave 3 (9.3%). During wave 1, patients were older on average (64.2 years) compared to wave 2 (58.8 years) and wave 3 (62.5 years). A larger percentage of patients were married in wave 1 (50.0%) and wave 2 (49.2%) compared to wave 3 (43.1%) (Table 1). In addition, the percentage of female patients was higher in wave 1 (50.8%) and wave 2 (48.7%) compared to wave 3 (45.1%). The average BMI was lower among those in wave 3 (30.7) versus wave 1 (32.0) and wave 2 (32.1). Other differences in the prevalence of comorbidities between waves are presented in Table 1.
Outcomes by wave
In adjusted and unadjusted analyses, the odds of death and requiring mechanical ventilation were lowest during wave 1, followed by wave 3, and were highest in wave 2 (Table 2). Patients in wave 2 had greater than two times the odds of mortality compared to patients in wave 1 in adjusted analyses (OR [95% CI]: 2.44 [1.71-3.49]; Table 2; Figure 2A). In adjusted analyses, odds of ICU stay were also higher in wave 2 (OR [95% CI]: 1.28 [1.08-1.51]) and wave 3 (OR [95% CI]: 1.24 [1.04-1.48]) in comparison to wave 1 (Table 2; Figure 2C). In both unadjusted and adjusted analyses, the odds of re-admittance between 1 and 30 days were approximately 20% lower in wave 2 (OR [95% CI]: 0.81 [0.69-0.95]) and wave 3 (OR [95% CI]: 0.84 [0.72-0.98]) compared to wave 1. However, the odds of re-admittance between 31 and 60 days during wave 3 were higher than wave 1 and wave 2, although this was only significant in unadjusted analyses. The odds of thromboembolism risk were highest in wave 3, although this was also not statistically significant in adjusted analyses. Finally, in unadjusted analyses, LOS was shorter in wave 3 compared to wave 1 and wave 2, although this was not statistically significant in adjusted analyses.
Comorbidities
The odds of mortality increased by age group (Figure 2A). Patients who were 75 years or older had greater than two times the odds of mortality compared with those patients aged 18-64 years (OR [95% CI]: 2.70 [2.14-3.40]). Females had lower odds of mortality compared with males (OR [95% CI]: 0.80 [0.68-0.95]). Comorbidities associated with greater odds of mortality included diabetes (OR [95% CI]: 1.20 [1.00-1.43]), hypertension (OR [95% CI]: 1.36 [1.11-1.67]), pulmonary disease (OR [95% CI]: 1.22 [1.01-1.46]), chronic kidney disease (OR [95% CI]: 1.93 [1.56-2.39]), coronary heart disease (OR [95% CI]: 2.45 [1.99-3.03]), and autoimmune disease (OR [95% CI]: 1.25 [1.04-1.49]). Having a COVID-19 vaccine was associated with 80% lower odds of mortality (OR [95% CI]: 0.20 [0.15-0.25]). Interestingly, tobacco use was also associated with lower odds of mortality (OR [95% CI]: 0.71 [0.55-0.92]).
The odds of mechanical ventilation were highest among those aged 64-74 years (Figure 2B). Patients aged less than 65 and 75 years and older had similar odds of mechanical ventilation. Risk factors for mechanical ventilation included morbid obesity (OR [95% CI]: 1.49 [1.28-1.74], compared to not being obese), diabetes (OR [95% CI]: 1.31 [1.15-1.50]), hypertension (OR [95% CI]: 1.33 [1.15-1.55]), chronic kidney disease (OR [95% CI]: 1.36 [1.14-1.62]), coronary heart disease (OR [95% CI]: 2.37 [2.00-2.81]), and having an autoimmune disorder (OR [95% CI]: 1.21 [1.06-1.39]). Females had lower odds of requiring mechanical ventilation (OR [95% CI]: 0.72 [0.64-0.82]). Those who received the COVID-19 vaccination had 51% lower odds of requiring mechanical ventilation compared with those who did not (OR [95% CI]: 0.49 [0.43-0.57]).
Risk factors for ICU stay included diabetes (OR [95% CI]: 1.30 [1.12-1.51]), hypertension (OR [95% CI]: 1.36 [1.14-1.61]), pulmonary disease (OR [95% CI]: 1.18 [1.01-1.39]), kidney disease (OR [95% CI]: 1.67 [1.38-2.02]), and coronary artery disease (OR [95% CI]: 2.15 [1.78-2.59]) (Figure 2C). Being female was associated with lower odds of ICU stay (OR [95% CI]: 0.74 [0.64-0.85]). Having the COVID-19 vaccination was also associated with lower odds of ICU stay (OR [95% CI]: 0.70 [0.60-0.82]).
Older age (>64 years old) and not being married were associated with about 30% greater odds of being re-admitted within 1-30 days (Figure 3A). Other risk factors for re-admittance between 1 and 30 days included chronic kidney disease (OR [95% CI]: 1.48 [1.23-1.78]), tobacco use (OR [95% CI]: 1.30 [1.09-1.55]), and coronary artery disease (OR [95% CI]: 1.37 [1.14-1.65]). Females had lower odds of being re-admitted within 1-30 days (OR [95% CI]: 0.87 [0.76-0.99]). Interestingly, obese patients and those with the COVID-19 vaccine had higher odds of re-admission. In addition, patients with hypertension had lower odds of being re-admitted (OR [95% CI]: 0.84 [0.72-0.99]).
Risk factors for being re-admitted within 31-60 days included being divorced, separated, or widowed (OR [95% CI]: 1.33 [1.08-1.65], compared to being married) (Figure 2E), chronic kidney disease (OR [95% CI]: 1.50 [1.17-1.91]), tobacco use (OR [95% CI]: 1.62 [1.29-2.03]), coronary artery disease (OR [95% CI]: 2.10 [1.65-2.67]), having the COVID-19 vaccine (OR [95% CI]: 1.44 [1.19-1.73]), and autoimmune disease (OR [95% CI]: 1.24 [1.01-1.51]). Obesity lowered the odds of being re-admitted.
The only factor associated with high thromboembolism risk was gender (Figure 2F). Females had lower odds of being at high risk for thromboembolism compared to males (OR [95% CI]: 0.77 [0.60-0.98]).
Demographics associated with a longer LOS included being older (>64 years old) and unmarried. Both of these factors increased the average LOS by approximately one day (Figure 2G). Other factors associated with a longer LOS include diabetes, hypertension, obstructive pulmonary disease, chronic kidney disease, coronary artery disease, and autoimmune disease. Being female, using tobacco, and having the COVID-19 vaccine were associated with a shorter LOS.
Demonstrates odds ratios for (A) mortality, (B) mechanical ventilation requirement, (C) ICU stay requirement, (D) 1-30-day re-admittance, (E) 31-60-day re-admittance, and (F) being at high risk for development of venous thromboembolism in a sample of patients with primary or secondary diagnoses of COVID-19 by demographic group and comorbidity (N = 7,197).In reference to these figures, 1 is in reference to the first wave of infections, 2 is in reference to ages <65 years, 3 is in reference to the male sex, 4 is in reference to a married marital status, and 5 is in reference to a Not Obese classification by BMI. Figure 2G represents the factors associated with LOS in the same sample of patients. In this figure, coefficients are back-transformed from the logarithm scale. Coefficients <1 are associated with a shorter LOS.
Age and wave interaction effects
The only outcome with a significant interaction effect between the age group and the wave was mortality (Figure 3). Across all age groups, mortality was highest in wave 2. However, those in the 65-74-year age group experienced a larger increase in mortality from wave 1 to wave 2.
Displays the probability of mortality in each wave stratified by age categorization.
Discussion
To our knowledge, this is the first study to compare the wave-based differences in outcomes of hospitalized patients with COVID-19 in the rural Appalachian region. This study offers a more comprehensive characterization of the effects of the COVID-19 pandemic on patients in the rural regions of Appalachian Kentucky and West Virginia.
Though exact strains were not isolated and reported for this study, the data gives indirect insight into the virulence patterns of the different COVID-19 strains most predominant in the country during these waves and how they may have affected rural Appalachian communities. For instance, the SARS-CoV-2 B.1.617.2 (Delta) variant emerged in the United States in June 2021 and remained the predominant sequenced lineage between July 2021 and November 2021 [13]. This correlates with the timeline of our second wave of infections in Appalachian Kentucky and West Virginia. The national Delta period was characterized by the highest crude mortality risk (15.1) and adjusted mortality risk for patients older than or equal to 18 years [14]. This is consistent with our data characterizing the second wave of infections, which also demonstrated the highest odds of mortality across all age groups, mechanical ventilation requirement, and ICU stay requirement in the region. The SARS-CoV-2 B.1.1.529 (Omicron) variant emerged in the United States in December 2021 and accounted for 72% of sequenced lineages by December 25, 2021 [15]. This emergence correlates with our third wave of infections in Appalachian Kentucky and West Virginia. The national Omicron period was characterized by a chronological decrease in crude mortality rate (13.1 in the early period; 4.9 in the late period), with 81.9% of in-hospital deaths occurring in elderly adults aged 65 years or older and 73.4% of in-hospital deaths occurring in patients with three or more underlying medical conditions [14]. This is also consistent with our data from the region, which demonstrated a similar mortality rate in the third wave compared to the first wave of infections. 29.8% of patients in wave 3 were aged 65 years or older, whereas 26.7% were in the same age group in wave 2. The first wave of infections in the region was likely a combination of the remaining major viral variants, including B.1.1.7 (Alpha), B.1.351 (Beta), and/or P.1 (Gamma), as these strains were most predominant in the timeline of wave 1 (April 2022 to May 2021) [16].
The increased odds of mortality, odds of ICU admittance, and odds of longer LOS demonstrated in wave 2 are likely primarily related to the presumed predominant viral strain according to the aforementioned timelines, which had been compounded in the Appalachian region through a combination of the poor resource allocation and funding in the rural setting during the pandemic. Regarding the strain of healthcare resources in the rural Appalachian setting, public health funding in this region is vastly inefficient. Allocation of healthcare resources is tiered. At the policy level, which is the highest level of resource allocation, strategies are determined through legislation, health insurance plans, and government funding mandates. At the organizational level, allocation decisions are made through institutional policies, clinical practice guidelines, and protocols [17]. For example, limited resources at the organizational level may attempt to maximize resources through triage protocols. Microallocation of resources, the lowest level of resource allocation, is mostly provider-dependent, anchored by the medical decision-making process and assessing risks versus benefit scenarios for particular interventions related to patient care [17].
During the COVID-19 pandemic, macroallocation in the form of federal mandates and legislation shifted the availability of resources as rural health departments rely heavily on state and federal funds. Local public health funding is often determined by a region’s overall wealth and tax base [18]. With rural communities facing a declining tax base and often having lower overall wealth, local health departments are typically left with insufficient or less stable funding. In Kentucky, local and state health officials worked to transform the public health funding model in 2018 to direct more resources to areas with the greatest needs to ensure equitable access to essential services and supplies [18]. This funding model, however, was hampered by budget constraints associated with the pandemic. The budget constraints also exacerbated financial issues at the institutional level in this region. As the virus spread throughout the United States, providers across the country were forced to cancel elective procedures, close or limit primary care and outpatient clinic hours, and shift resources from higher margin care to focus on acute COVID-19 cases, which inevitably led to an institutional loss of revenue [19]. As the Appalachian region was not exempt from this effect, this exacerbated institutional funding problems. In response, many hospitals throughout the pandemic were forced to furlough staff or reduce working hours, leading to staffing constraints within hospitals, role frustration, and burnout [19].
The odds of overall mortality in this region were increased at baseline, given the comorbidity of the patient population. Comorbid conditions, such as smoking status, chronic obstructive pulmonary disease (COPD), diabetes, and obesity, have been deemed clinical risk factors for fatal outcomes associated with coronavirus [20]. In Central Appalachia, the prevalence of smoking (the leading cause of COPD in the United States) in adults is 25.2% in comparison to the national level of 16.3%. The prevalence of diabetes in Appalachia is 11.9% overall (13.7% in the region’s most distressed counties) in comparison to the national mark of 9.8%. Obesity is 34.7% prevalent in the Central Appalachian region, which is also higher than the national level of 27.4% [21]. Concerning the present study, tobacco use, obstructive pulmonary disease, and diabetes were all less present in hospitalized patients. However, obesity in general was present in slightly more than half of hospitalized patients, with a vast majority of patients at least being overweight. These results were surprising; however, it is possible that more critical patients with these comorbidities were admitted to one of the tertiary care institutions in the region instead of the lower acuity hospitals in the ARH healthcare system.
Limitations
This study has several limitations. Recall bias and database documentation errors are derived from the intrinsic study design. Along with these limitations, the predominant COVID-19 strain for each wave in this area of Central Appalachia was not recorded in the EMR database. Therefore, the dominant viral strain per wave is unknown. Racial characterizations for patients were not captured in the datasets for the study. Thus, racial disparities related to the pandemic in rural Central Appalachia could not be measured. Dates were based on the dates of initial admittance to the ARH healthcare system, not the date of symptom onset or diagnosis. Our team could also not assess the differences in severity or stage of comorbid conditions because only ICD-10 master codes were utilized.
Additionally, the use of remdesivir in hospitalized adult patients with COVID-19 has been shown to result in a moderate reduction in length of stay in previous studies [22]. However, dates of administration of remdesivir or steroid therapy were not captured in this database for inclusion in this study. We cannot translate these results on LOS in Appalachia. However, this study aimed to represent the pandemic in a large, underserved region comprehensively. It was not meant to evaluate the relationship of individual therapies in the region. Future studies comparing the clinical impacts of specific variants in rural Appalachian and urban or suburban communities should be assessed to unveil potential health disparities between the communities. Further, retrospective or prospective studies examining the effects of different therapeutic modalities, such as steroid therapy or remdesivir administration, in this particularly comorbid patient population may provide interesting insight.
Conclusions
This is the first study to compare the wave-based differences in outcomes of hospitalized patients with COVID-19 in the rural Appalachian region. This report characterizes the COVID-19 pandemic’s effect on the Central Appalachian region. The second wave of infections during the pandemic resulted in the highest mortality rate, with elderly patients and patients with comorbidities being the most significant. Future studies comparing the clinical impacts of specific variants in rural Appalachian and urban or suburban communities should be evaluated to unveil potential health disparities between the communities.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization: COVID-19 Dashboard 3 2023 2023 https://covid 19.who.int/
- 2Three waves changes, new variant strains, and vaccination effect against COVID-19 pandemic Int J Biol Macromol El-Shabasy RM Nayel MA Taher MM Abdelmonem R Shoueir KR Kenawy ER 16116820420223507433210.1016/j.ijbiomac.2022.01.118PMC 8782737 · doi ↗ · pubmed ↗
- 3United States Census Bureau: New census data show differences between urban and rural populations 3 2023 2016 https://www.census.gov/newsroom/press-releases/2016/cb 16-210.html#:~:text=Adults%20in%20rural%20areas%20had,19.5%20percent%20compared%20with%2029.0)
- 4Rural Health Research Gateway. Rural Communities: Age, Income, and Health Status Rural Health Research Gateway 3 2023 Schroeder S 12Grand Forks, ND Rural Health Research Gateway 2018 https://www.ruralhealthresearch.org/alerts/262
- 5Rural-Urban Differences Among Older Adults The University of Minnesota Rural Health Research Center Chartbook Tuttle C Tanem J Lahr M Schroeder J Tuttle MS Henning-Smith C 141Minneapolis, MN University of Minnesota Rural Health Research Center 2020 https://rhrc.umn.edu/publication/rural-urban-differences-among-older-adults/
- 6Unequal distribution of COVID-19 risk among rural residents by race and ethnicity J Rural Health Henning-Smith C Tuttle M Kozhimannil KB 2242263720213239622010.1111/jrh.12463 PMC 7273062 · doi ↗ · pubmed ↗
- 7Dynamics of the COVID-19 epidemic in urban and rural areas in the United States Ann Epidemiol Cuadros DF Branscum AJ Mukandavire Z Miller FD Mac Kinnon N 16205920213389438510.1016/j.annepidem.2021.04.007PMC 8061094 · doi ↗ · pubmed ↗
- 8COVID-19 exacerbating inequalities in the US Lancet Dorn AV Cooney RE Sabin ML 1243124439520203230508710.1016/S 0140-6736(20)30893-XPMC 7162639 · doi ↗ · pubmed ↗