Internuclear ophthalmoplegia as a presentation of procedural stroke: a case report
Norachai Sirisreetreerux, Krongkamol Ponglikitmongkol

TL;DR
A patient developed internuclear ophthalmoplegia after a cardiac catheterization, revealing a rare case of procedural stroke with full recovery.
Contribution
This case highlights internuclear ophthalmoplegia as an unusual and potentially misdiagnosed presentation of procedural stroke.
Findings
Internuclear ophthalmoplegia can present as an unusual symptom of procedural stroke.
MRI confirmed acute infarcts in the midbrain and cerebellum following the procedure.
The patient fully recovered within six weeks despite multiple brain infarcts.
Abstract
Cardiac catheterization and endovascular procedures are extensively used in modern medicine, and procedural stroke is one of the major complications that the catheterization laboratory team may face in their everyday work. Recognizing the signs and symptoms of procedural stroke is crucial to ensuring appropriate management. We herein report a case of internuclear ophthalmoplegia that caused blurred vision, diplopia, and dizziness on lateral gaze as an unusual presentation of procedural stroke. A 60-year-old Thai woman underwent right partial colectomy and was diagnosed with stage IV diffuse large B-cell lymphoma. Pre-chemotherapy echocardiography revealed mild left ventricular systolic dysfunction, and she therefore underwent diagnostic catheterization. Coronary angiography revealed normal coronary arteries, leading to a diagnosis of non-ischemic cardiomyopathy. After the procedure,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1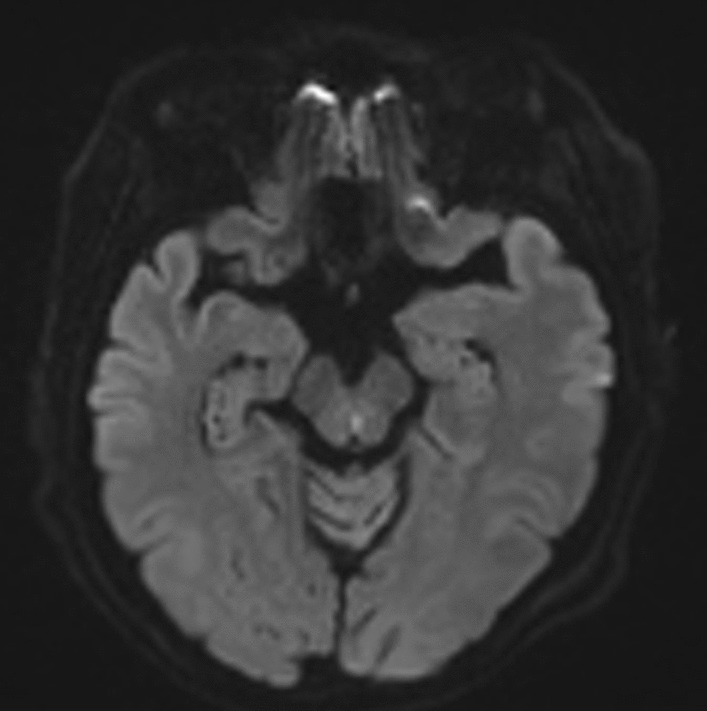 Figure 2
Figure 2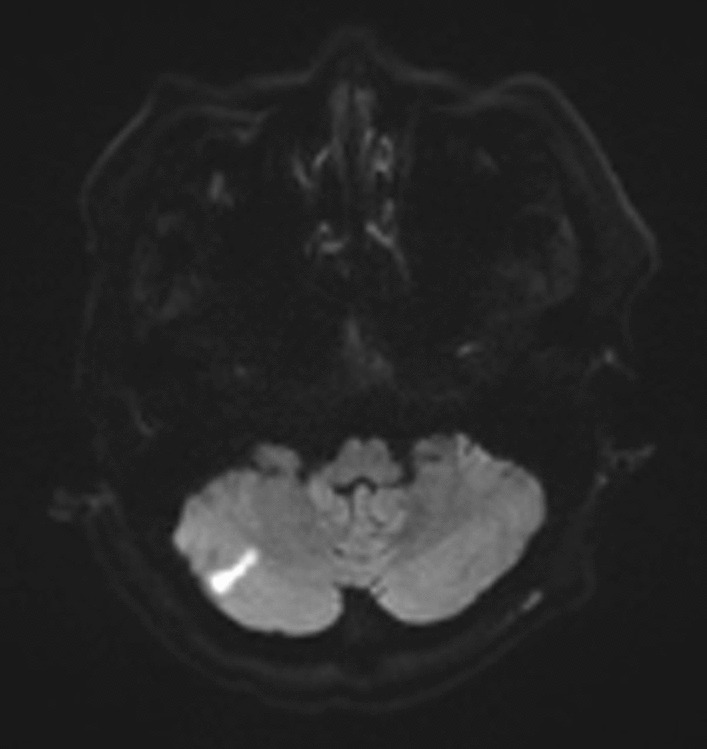 Figure 3
Figure 3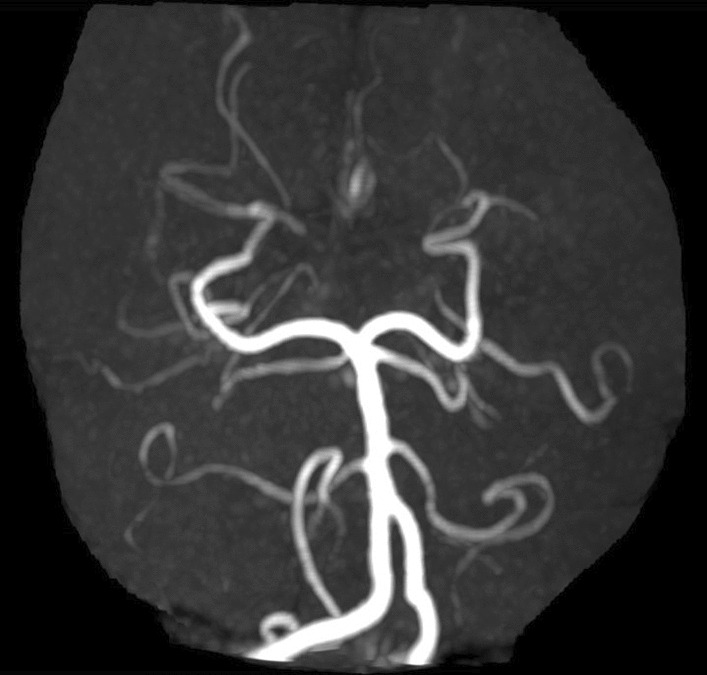 Figure 4
Figure 4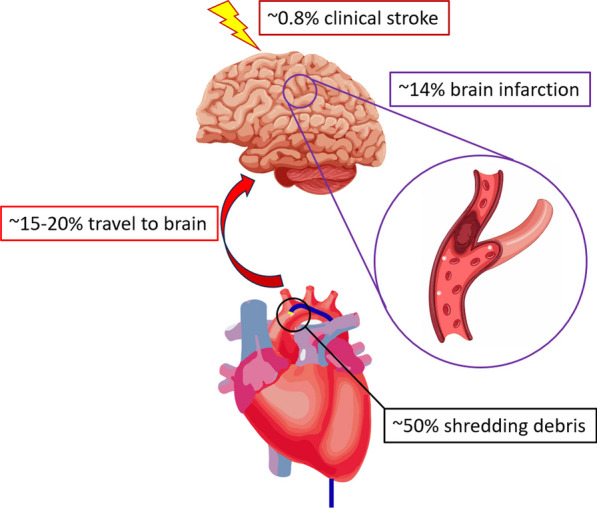 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntracranial Aneurysms: Treatment and Complications · Moyamoya disease diagnosis and treatment · Vascular Malformations Diagnosis and Treatment
Background
Cardiac catheterization and endovascular procedures are widely used in modern medicine, with more than 1 million procedures being performed in the USA annually [1]. With the rapid increase in the total number of procedures, the risk of complications during and after the procedure is also growing. One such complication is procedural stroke. Despite years of progress in terms of technology, skill, and experience, the incidence of procedural stroke remains high [2–6]. According to the “8 Ds” of stroke care, the first step in appropriate management is to recognize the signs and symptoms of stroke [7]. This is especially important in cases of procedural stroke in which a medical team has limited experience with this complication. We herein describe a patient who developed procedural stroke with an unusual presentation of internuclear ophthalmoplegia (INO) that caused blurred vision, diplopia, and dizziness on lateral gaze [8].
Case presentation
A 60-year-old female Thai farmer was scheduled for pre-chemotherapy echocardiography after undergoing a right partial colectomy and being diagnosed with stage IV diffuse large B-cell lymphoma. Echocardiography revealed diminished left ventricular systolic function, calculated at 45% by Simpson’s method. She had type 2 diabetes mellitus, hypertension, and dyslipidemia, all of which were adequately controlled. Her medication prior to diagnostic catheterization included aspirin 81 mg/day and clopidogrel 75 mg/day for upfront medication in case of intervention needed; metformin 2000 mg/day and glipizide 10 mg/day for glycemic control; gemfibrozil 600 mg/day and atorvastatin 40 mg/day for lipid control; and enalapril 5 mg/day for antihypertensive. She never smokes but does occasionally consume alcohol. She is the mother of two children without a history of miscarriage. Her other past history was otherwise unremarkable. On her admission date, her blood pressure was 119/57 mmHg and her pulse rate was 86 beats per minute. Blood tests showed the following: fasting blood glucose, 138 mg/dL; glycated hemoglobin, 5.7%; total cholesterol, 84 mg/dL; and low-density lipoprotein, 28 mg/dL. Coronary angiography revealed normal coronary arteries, leading to a diagnosis of non-ischemic cardiomyopathy. After the procedure, she immediately experienced dizziness and diplopia. Her physical examination immediately after the procedure showed blood pressure of 140/69 mmHg and pulse rate of 86 beats per minute. Her neurological examination during the right lateral gaze showed impaired adduction of the left eye and horizontal nystagmus of the right eye. A diagnosis of left INO was made by a neurologist (Fig. 1).Fig. 1. Clinical photograph showing impaired left-eye adduction during the right lateral gaze
Immediate non-contrast computed tomography (CT) of the brain showed no signs of bleeding. Magnetic resonance imaging (MRI) on the fifth day after clinical onset revealed a tiny area exhibiting characteristics of an acute infarct in the left paramedian midbrain, including the left medial longitudinal fasciculus, consistent with the clinical diagnosis of INO (Fig. 2). An additional region of restricted diffusion indicating an acute infarct was detected in the right inferior cerebellar hemisphere (Fig. 3). The presence of multiple brain infarcts in this patient supported the etiology of embolic stroke from the catheterization procedure. Magnetic resonance angiography revealed no significant cerebral artery disease (Fig. 4). The patient was treated in the stroke unit for 5 days according to stroke protocol, with medications including intravenous hydration of 1.5 mL/kg/hour for 2 days, dual antiplatelets, and statin, and 6 weeks after symptom onset, the patient achieved full neurological recovery. She received complete treatment for diffuse large B-cell lymphoma, which consisted of six cycles of the R-CEOP regimen to reduce the risk of further cardiac function deterioration and intrathecal methotrexate for high central nervous system (CNS) involvement risk, which was accompanied by clopidogrel withholding. She finally achieved a complete molecular response and remained uneventful after 6 months of treatment.Fig. 2. Axial diffusion-weighted image showing a diffusion defect in the left paramedian midbrainFig. 3Axial diffusion-weighted image showing a diffusion defect in the right cerebellumFig. 4Magnetic resonance angiography showing no significant evidence of atherosclerotic disease
Discussion and conclusions
We hereby present the case of a procedural stroke that occurred during diagnostic catheterization in a patient with hematologic malignancy who needed a clear diagnosis of the etiology of cardiomyopathy to proceed with chemotherapy treatment. Making the right choice requires precision medicine to differentiate this kind of stroke from other typical strokes, particularly in individuals with complex medical histories.
Procedural stroke has been hypothesized as resulting from atheromatous plaque embolism, dislodgement of device material, and air leakage, with varying levels of risk depending on the individual patient’s condition and the type of intervention. Interestingly, debris can be found in more than 50% of catheters used in percutaneous revascularization procedures [9]. Embolized debris must flow from the aorta into the brain circulation and lodge in a specific brain area to cause clinical stroke. The brain is generally assumed to receive 15–20% of the cardiac output [10]. When these data are taken into account as a theoretical risk, they are comparable to the findings of a meta-analysis of magnetic resonance imaging studies showing that 14% of patients undergoing percutaneous coronary intervention had silent brain infarctions [11]. In the present case, the risk ratio of focal neurologic deficit to silent brain infarction was only 0.06, which can be converted into an approximately 0.8% absolute risk of percutaneous intervention-related clinical stroke (Fig. 5). This level of risk is consistent with the overall rate of clinical stroke in another real-world study, which showed a risk of 0.18–0.44% for percutaneous coronary interventions and 0.06% for diagnostic coronary angiography [3].Fig. 5. Probability of procedural stroke in different cascades
Many risk factors contribute to procedural stroke. Atherosclerotic risk factors include advanced age, diabetes mellitus, arterial hypertension, and renal failure [12], all of which are unmodifiable or partially modifiable. Procedure-related risk factors include the type of procedure [11], access site [5], bulkiness of the catheter [13], catheter curvature [9], and contrast volume [13]; these are relatively more modifiable with pre-procedural planning and operator awareness.
INO is a rare presentation of stroke, especially procedural stroke. Occurrence of stroke at the medial longitudinal fasciculus results in ipsilateral adduction impairment and contralateral horizontal abduction nystagmus [8]. Although INO itself typically has a favorable prognosis [14], more than one brain infarct may be present in patients with procedural stroke, and this can affect the overall prognosis [15]. According to data from multiple large registries [3], procedural stroke is associated with substantial morbidity and mortality, with mortality rates ranging from 22–37%. Therefore, as for other types of strokes, an appropriate basic approach to stroke care remains critically important. This includes timely and accurate diagnosis, effective logistics for choosing an optimal revascularization technique, and availability of specialized stroke care units.
In conclusion, we have herein reported an unusual presentation of procedural stroke that is likely to be misdiagnosed, particularly by a medical care team inexperienced with INO. Despite the good prognosis of INO, appropriate stroke care remains indispensable in patients with procedural stroke because of the risk of multiple brain infarcts.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Virani SS Alonso A Benjamin EJ Bittencourt MS Callaway CW Carson AP American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Subcommittee Heart disease and stroke statistics-2020 update: a report from the American Heart Association Circulation 2020141 e 139e 59610.1161/CIR.000000000000075731992061 · doi ↗ · pubmed ↗
- 2Fuchs S Stabile E Kinnaird T Mintz GS Gruberg L Caños D Stroke complicating percutaneous coronary interventions Circulation 20021061869110.1161/01.CIR.0000020678.16325.E 012093775 · doi ↗ · pubmed ↗
- 3Werner N Zeymer U Stroke outcomes in patients undergoing percutaneous coronary intervention in clinical practice today Interv Cardiol 2011340741310.2217/ica.11.37 · doi ↗
- 4Hoffman SJ Holmes DR Rabinstein AA Rihal CS Gersh BJ Lennon RJ Trends, predictors, and outcomes of cerebrovascular events related to percutaneous coronary intervention JACC Cardiovasc Interv 20114441542210.1016/j.jcin.2010.11.01021511221 · doi ↗ · pubmed ↗
- 5Shoji S Kohsaka S Kumamaru H Sawano M Shiraishi Y Ueda I Stroke after percutaneous coronary intervention in the era of transradial intervention Circ Cardiovasc Interv 20181112 e 00676110.1161/CIRCINTERVENTIONS.118.00676130545258 · doi ↗ · pubmed ↗
- 6Abdel-Latif A Misumida N Ischemic stroke after percutaneous coronary intervention JACC Cardiovasc Interv 201912151507150910.1016/j.jcin.2019.05.01331395221 · doi ↗ · pubmed ↗
- 7Ashcraft S Wilson SE Nyström KV Dusenbury W Wira CR Burrus TM American Heart Association Council on Cardiovascular and Stroke Nursing and the Stroke Council Care of the patient with acute ischemic stroke (prehospital and acute phase of care): update to the 2009 comprehensive nursing care scientific statement: a scientific statement from the American Heart Association Stroke 202152 e 164e 17810.1161/STR.000000000000035633691468 · doi ↗ · pubmed ↗
- 8Feroze KB, Wang J. Internuclear ophthalmoplegia [Updated 2022 Jun 27]. In: Stat Pearls. Treasure Island: Stat Pearls Publishing; 2023.28722999 · pubmed ↗