Histopathological, Demographic, and Clinical Signatures of Medulla Oblongata Germ Cell Tumors: A Case Report With the Review of Literature
Daisuke Sato, Shota Tanaka, Hirokazu Takami, Shunsaku Takayanagi, Yurie Rai, Munetoshi Hinata, Atsuto Katano, Nobuhito Saito

TL;DR
This case report and literature review explores rare medulla oblongata germ cell tumors, highlighting their clinical features and treatment outcomes.
Contribution
The study provides new insights into the clinical and pathological characteristics of a rare CNS tumor location.
Findings
The prognosis of medulla oblongata GCTs is comparable to typical sites.
Germinoma is the predominant subtype with a female preponderance and older age at onset.
Local recurrence patterns suggest limited need for extensive radiation coverage.
Abstract
The medulla oblongata is one of the rarest sites of occurrence for germ cell tumors (GCTs) of the central nervous system. As there is scant data regarding epidemiology, clinical presentations, optimal intervention, and long-term prognosis, we aimed to delineate the features of this rare entity by presenting our representative case and performing a quantitative review of the literature. A 24-year-old woman presented to our department with vertigo and swallowing difficulties. Magnetic resonance imaging revealed a homogenously enhanced exophytic lesion arising from the medulla oblongata and extending to the fourth ventricle. Surgical resection was performed and a histological diagnosis of pure germinoma was made. The patient underwent chemotherapy and whole-ventricular irradiation. No recurrence has been experienced for 4 months after the surgery. According to the literature, the prognosis…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
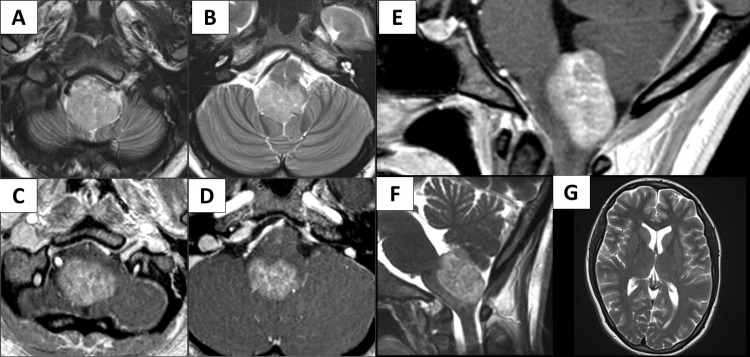 Figure 1
Figure 1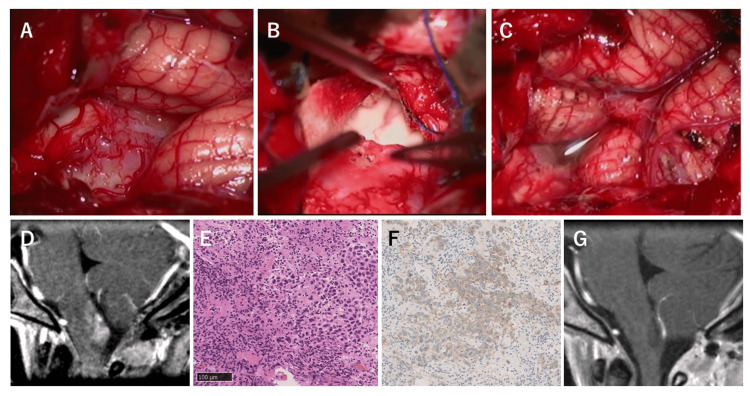 Figure 2
Figure 2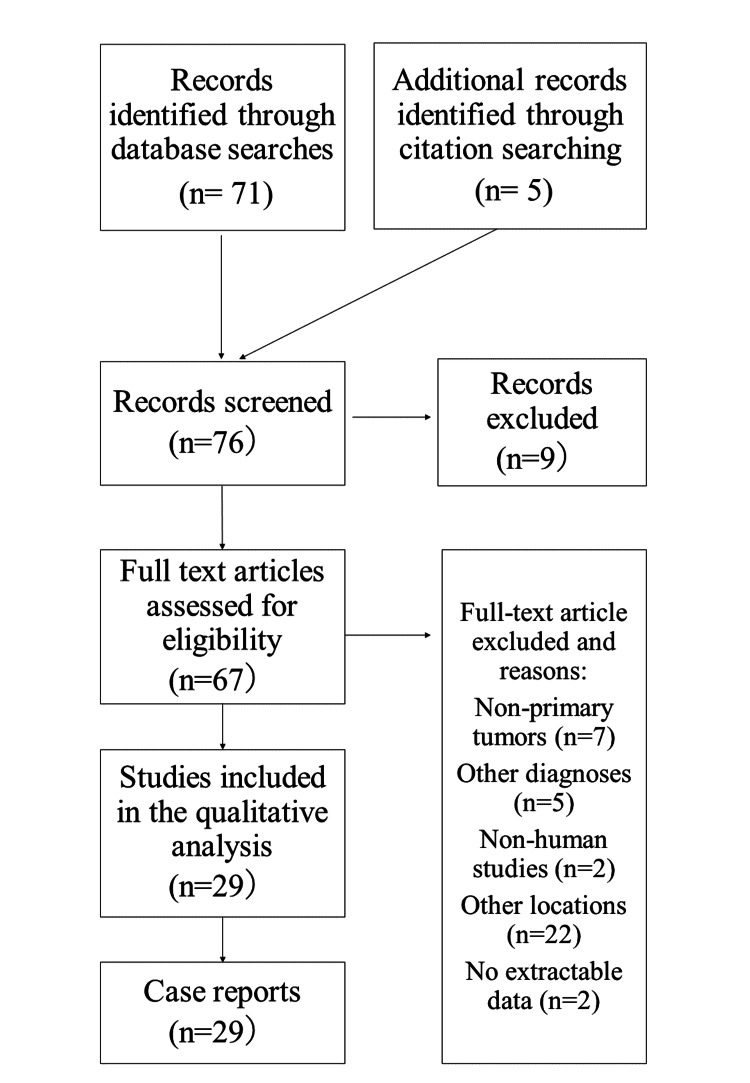 Figure 3
Figure 3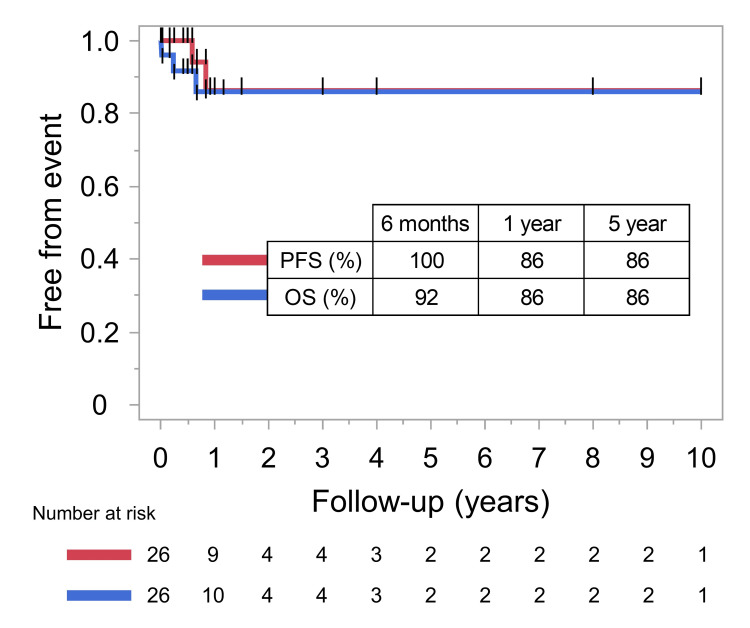 Figure 4
Figure 4| Author (year) | Age/Sex | Histological diagnosis | Germinoma component | Extent of resection | Hydrocephalus | Area of irradiation | Chemotherapy | Initial cytology | Concomitant dissemination | Degree of lymphoplasmacytic infiltration | Relapse | Relapse free period | Form of relapse | Follow-up period | Survival |
| Iwasaki et al., 1984 [ | 12y/F | Teratoma with a prominent rhabdomyogenic element and germinoma | Yes | GTR | Evident | Radiation (not otherwise described) | - | - | No | Moderate | No | 18 days | - | 18 days | Dead (Pneumonia and gastrointestinal bleeding) |
| Poungvarin et al., 1991 [ | 17y/M | Germinoma | Yes | PR | No | Radiation (not otherwise described) | - | - | No | Moderate | No | 3 months | - | 3 months | Dead (Pneumonia) |
| Hashimoto et al., 1992 [ | 19y/F | Germinoma | Yes | PR | No | Whole brain 30Gy + Tumor site 30Gy + Spinal cord 35Gy | - | - | No | Sparse | No | 2 months | - | 2 months | Alive |
| Tashiro et al., 1993 [ | 30y/F | Germinoma | Yes | PR | No | Tumor site 40Gy | 1st: CDDP + VP-16; 2nd: CBCDA + VP-16 | - | Suprasellar lesion | Moderate | Yes | 10 months | Local recurrence | 14 months | Alive |
| Sugiyama et al., 1994 [ | 32y/F | Germinoma | Yes | PR | No | Tumor site 44Gy + Spinal cord 20Gy | - | - | No | Moderate | No | 9 years | - | 9 years | Alive |
| Israel et al., 1996 [ | 17y/M | Choroid plexus papilloma with germinoma | Yes | STR | No | Whole ventricular system and tumor site (not otherwise described) | CDDP + VP-16 + BLM | No abnormality | No | Moderate | No | 18 months | - | 18 months | Alive |
| Nakajima et al., 2000 [ | 18y/F | Germinoma | Yes | PR | No | Gamma knife surgery | CBCDA + VP-16 | - | No | Moderate | No | 8 months | - | 8 months | Alive |
| Tsuzuki et al., 2001 [ | 39y/M | Immature teratoma | No | PR | No | Radiation (not otherwise described) | Chemotherapy (not otherwise described) | - | No | Moderate | Yes | 3 months | Local recurrence | 3 months | Dead (Respiratory failure) |
| Yoshida et al., 2003 [ | 33y/M | Germinoma | Yes | STR | No | - | CBCDA + VP-16 | No abnormality | No | Moderate | No | 7 months | - | 7 months | Alive |
| Yen et al., 2003 [ | 16y/F | Germinoma | Yes | STR | Mild | Whole brain 30 Gy + Tumor site 50Gy + Spinal cord 30Gy | - | - | No | Moderate | No | 7 years | - | 7 years | Alive |
| Kakani et al., 2006 [ | 16y/F | Germinoma | Yes | STR | No | - | - | No abnormality | Suprasellar lesion | Moderate | No | 12 days | - | 12 days | Dead (Cardiac arrest) |
| Yang et al., 2009 [ | 12y/M | Germinoma | Yes | STR | No | 10 weeks (not otherwise described) | CDDP + IFOS | - | No | Moderate | No | 6 months | - | 6 months | Alive |
| Akimoto et al., 2009 [ | 30y/F | Germinoma | Yes | STR | No | Tumor site (not otherwise described) | Chemotherapy (not otherwise described) | - | No | Sparse | No | 12 months | - | 12 months | Alive |
| Akimoto et al., 2009 [ | 24y/M | Germinoma | Yes | STR | No | Tumor site (not otherwise described) | Chemotherapy (not otherwise described) | - | No | Sparse | No | 8 months | - | 8 months | Alive |
| Madden et al., 2009 [ | 12y/M | Germinoma | Yes | STR | No | Whole brain 21Gy + Tumor site 9Gy + Spinal cord 21Gy | CBCDA + VP-16 | - | No | Moderate | No | 12 months | - | 12 months | Alive |
| Madden et al. , 2009 [ | 21y/M | Teratoma with germinoma and embryonal carcinoma elements | Yes | GTR | No | Posterior fossa 21.6Gy + Tumor site 32.4Gy | CBCDA + VP-16 + BLM | - | No | Moderate | Yes | 2.5 years | Local recurrence | 3.5 years | Dead (Respiratory failure) |
| Neelima et al., 2010 [ | 24y/F | Germinoma | Yes | GTR | No | - | - | - | No | Moderate | No | - | - | Alive | |
| Yasuhara et al., 2011 [ | 27y/F | Germinoma | Yes | PR | No | Whole ventricular system 30Gy + Tumor site 20Gy | IFOS + CDDP + VP-16 | - | No | Moderate | No | 11 months | - | 11 months | Alive |
| Shuto et al., 2012 [ | 28y/M | Germinoma | Yes | GTR | No | Tumor site 45Gy + Spinal cord 27Gy | CBCDA + VP-16 | - | No | Moderate | No | 3 years | - | 3 years | Alive |
| Nakatsuka et al., 2012 [ | 31y/F | Germinoma | Yes | STR | No | Whole ventricular system 24Gy + Tumor site 24Gy | CBCDA + VP-16 | - | No | Moderate | No | 6 months | - | 6 months | Alive |
| Hao et al., 2013 [ | 14y/M | Germinoma | Yes | STR | No | Gamma knife surgery | CDDP + VP-16 + BLM | - | No | Moderate | No | 4 years | - | 4 years | Alive |
| Hao et al., 2013 [ | 22y/F | Germinoma | Yes | STR | No | - | - | - | No | Moderate | Yes | 7 months | Local recurrence | 8 months | Dead (Pneumonia) |
| Khan et al., 2013 [ | 25y/F | Germinoma | Yes | PR | No | Whole brain 24Gy + Tumor site (posterior fossa and spinal cord) 16Gy + Spinal cord 24 Gy | - | - | Spinal cord | Dense | No | 10 months | - | 10 months | Alive |
| Li et al., 2014 [ | 9y/M | Mature teratoma | No | GTR | No | - | - | - | No | Slight | No | 22 days | - | 22 days | Dead (CNS infection) |
| Li et al., 2014 [ | 10y/M | Immature teratoma | No | GTR | No | - | IFOS + CDDP + VP-16 | - | No | Sparse | No | 59 months | - | 59 months | Alive |
| Yip et al., 2014 [ | 22y/F | Germinoma | Yes | GTR | No | Whole ventricular system 30.6Gy + Tumor site 45Gy | - | - | No | Moderate | No | 12 months | - | 12 months | Alive |
| Budohoski et al., 2016 [ | 23y/F | Germinoma | Yes | GTR | No | Whole brain 25Gy + Tumor site 15Gy + Spinal cord 25Gy | - | - | No | Sparse | No | 12 months | - | 12 months | Alive |
| Seifert et al., 2020 [ | 12y/F | Germinoma | Yes | GTR | No | Tumor site (not otherwise described) | CBCDA + VP-16 | - | No | Dense | No | 18 months | - | 18 months | Alive |
| Thong et al., 2020 [ | 12y/M | Germinoma | Yes | GTR | No | Radiation (not otherwise described) | Chemotherapy (not otherwise described) | - | No | Moderate | No | 7 days | - | 7 days | Alive |
| Tai et al., 2021 [ | 25y/M | Germinoma | Yes | GTR | No | Radiation (not otherwise described) | CDDP + VP-16 | - | No | Moderate | No | 8 months | - | 8 months | Alive |
| Zhang et al., 2021 [ | 15y/M | Mature Teratoma | No | GTR | No | - | - | - | No | Sparse | No | 12 months | - | 12 months | Alive |
| Isaji et al., 2022 [ | 50y/F | Mixed tumor with a yolk sac tumor component | Yes | PR | No | Whole ventricular system 25.2Gy + Tumor site 32.4Gy | - | No | Moderate | No | 18 months | - | 18 months | Alive | |
| Albina et al., 2022 [ | 33y/F | Germinoma | Yes | PR | No | Whole ventricular system 23.4Gy + Tumor site 45Gy | - | - | No | Moderate | No | 6 months | - | 6 months | Alive |
| Present case | 24/F | Germinoma | Yes | STR | No | Whole ventricular system 24Gy + Tumor site 24Gy | CBCDA + VP-16 | No abnormality | No | Moderate | No | 5 months | - | 5 months | Alive |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Glioma Diagnosis and Treatment · Spinal Dysraphism and Malformations
Introduction
Germ cell tumors (GCTs) cover a spectrum of neoplastic diseases derived from primordial germ cells at different stages of maturation [1-3]. GCTs are classified based on the distinct developmental potency of the primordial germ cells [1]. Although the gonads are the dominant location, 1-5% of GCTs arise in extragonadal sites [4]. During the early stage of embryogenesis, primordial germ cells migrate from the yolk sac wall towards the genital ridge, consequently forming the gonads. Primordial germ cells that have topographically mis-migrated and circumvented apoptosis or elimination by the immune system are presumed to lead to extragonadal GCTs [1,2,5]. The anatomical distribution of extragonadal GCTs along the midline of the body reflects the migration route of primordial germ cells [1,6]. Such cells are typically implanted in the midline of the sacrum, retroperitoneum, mediastinum, and midline of the central nervous system (CNS) [7]. Typical locations in the CNS are the pineal gland, followed by the neurohypophysis and lateral/third ventricles, accounting for 80-90% [8-11]. Atypical locations include the basal ganglia and thalamus, among others [12-14], and occurrence at the medulla oblongata is rare.
CNS GCTs have been known to demonstrate site-specific clinical and histopathological presentations. Sex is tightly linked to the site of occurrence, with cases at the neurohypophysis generally showing equality between sexes [15], while pineal gland GCTs predominantly occur in males (approximately 90%) [16]. Histopathology is also site-dependent, as germinoma predominates at the neurohypophysis, while non-germinomatous GCTs (NGGCTs) commonly arise at the pineal gland [8]. Little is known about the clinical and histopathological presentations for GCTs at atypical sites, much less for medulla oblongata GCTs, particularly in terms of clinical behaviors. While chemotherapy (CMT) regimens and radiation fields have been historically investigated for GCTs at typical sites in multiple clinical trials worldwide [10,17-24], the most appropriate treatment strategies, such as optimal radiation field based on relapse patterns, remain poorly characterized [25]. Germinomas at atypical sites outside of these midline structures have been known to show worse prognoses than those at typical sites [8].
This study examined the literature for clinical and histopathological findings of GCTs arising at the medulla oblongata [26-54]. This study aimed to elucidate the characteristic features of this atypical occurrence compared to those of GCTs arising from typical locations.
Case presentation
A 24-year-old woman without any contributory medical history was referred to our department with progressively worsening vertigo and mild swallowing difficulties over the past few weeks. A neurological examination revealed an unstable gait. Ocular movements were intact and congruent. No ataxia or cranial nerve palsy was evident, except for mild impairment of deglutition. Magnetic resonance imaging (MRI) revealed a homogenously enhancing exophytic lesion arising from the medulla oblongata and extending to the fourth ventricle (Figure 1A-1D). The lesion was spreading through the roof of the fourth ventricle, sparing the floor of the fourth ventricle, vermis, and tonsil (Figure 1E-1F). Hydrocephalus was not present (Figure 1G). CSF cytology was normal (class I). Levels of tumor markers (alpha-fetoprotein, beta-human chorionic gonadotropin) showed no abnormalities. No spinal cord lesion was observed on MRI. No other systemic lesion was present on computed tomography or positron emission tomography, reducing the likelihood of metastasis. Differential diagnoses included pilocytic astrocytoma, posterior fossa ependymoma, medulloblastoma, and diffuse midline glioma, H3 K27-altered.
Pre-operative images of the representative caseMagnetic resonance imaging revealed a solid mass occupying the medulla oblongata (A). The lesion exhibited T2 high intensity and was compressing the surrounding structures (B). Homogenous gadolinium enhancement was observed (C, D). The lesion was located at the dorsal aspect of the medulla oblongata and was protruding to the fourth ventricle (E, F). Hydrocephalus was not evident (G).
To alleviate the neurological symptoms and obtain a pathological diagnosis, surgical resection was proposed. The patient and her family consented to the treatment. Under general anesthesia, the lesion was approached via a midline suboccipital craniotomy and C1 laminectomy. The tumor arose from the medulla oblongata's dorsal aspect with an indistinguishable border and protrusion to the cerebellomedullary fissure (Figure 2A). Dissection of the cerebellomedullary fissure bilaterally revealed the extension of the tumor through the tela choroidea to the inferior medullary velum, while the foramen of Magendie was spared. Further, the inner surface of the cerebellum and the floor of the fourth ventricle were intact (Figure 2B). As intraoperative histopathological diagnosis was elusive, subtotal resection was performed (Figure 2C).
Intraoperative findings and postoperative images of the representative caseThe lesion was pinkish and was surrounded by engorged tortuous vessels (A). The lesion extended along the tela choroidea, and the floor of the fourth ventricle was spared (B). Subtotal resection was performed without any damage to the surrounding vital structures (C). Postoperative imaging revealed sufficient tumor resection without unintentional brainstem damage (D). Histologically, the tumor was composed of small lymphocyte infiltration and pleomorphic tumor cells with large eosinophilic cytoplasm and irregularly shaped nucleus (E). C-kit was positive for the cytoplasm of the tumor cells (F). Follow-up imaging after chemoradiotherapy showed no tumor recurrence (G).
The patient quickly recovered from anesthesia and the surgery without any postoperative complications. Improvements in vertigo and deglutition were observed, with these symptoms vanishing a few days after the surgery. Postoperative imaging revealed a subtotal resection of the tumor, with no unintentional damage to the surrounding structures (Figure 2D). Histopathological exploration demonstrated abundant infiltration of lymphocytes and sheets of large atypical cells with large, irregularly shaped nuclei and clear cytoplasm, constituting the classical “two-cell pattern” (Figure 2E). Immunohistochemistry showed positive results for c-kit (Figure 2F), podoplanin, and placental alkaline phosphatase. A histopathological diagnosis of pure germinoma was made.
The patient underwent further treatment with CMT comprising carboplatin and etoposide, and intensity-modulated radiation therapy (IMRT) with a dose of 24 Gy to the whole ventricles. She has been followed up every two months, and no recurrence has been observed 4 months after the surgery (Figure 2G). Written informed consent was obtained from the patient.
Discussion
Literature review
Methods
A quantitative review of the literature was conducted in December 2022. PubMed was queried using search terms such as “germinoma or germ cell tumor (s) or teratoma” and “medulla or fourth ventricle”. An exhaustive search of citations was also conducted. Two authors (D.S. and H.T.) scrutinized the source and data. Inclusion criteria were all case reports and case series regarding primary (neither recurrent nor metastatic) GCT of the medulla oblongata. No large-scale studies have been reported due to the rarity of the disease. Reports describing irrelevant cases were excluded. Non-English language publications and reports with unclear clinical descriptions were also excluded. A flow chart of the study selection process is presented in Figure 3.
Flow chart of the study selection processThe quantitative review retrieved literature published from January 1983 to December 2022 related to primary germ cell tumors (GCTs) involving the medulla oblongata and/or fourth ventricle. A total of 29 studies describing 33 cases were identified. We added our case to this cohort.
Data Extraction
Data extraction was performed by two independent investigators (D.S. and H.T.). The information collected was as follows: age, sex, tumor location, evidence of hydrocephalus at initial presentation, findings from CSF cytology, treatment modalities (extent of surgical resection, field, and dose of radiotherapy {RT} and CMT regimens), presence of dissemination in the CSF space on imaging, and treatment outcomes (relapse and survival).
Statistical Analysis
Our case was added to this pooled data. All statistical analyses were carried out using JMP version 16 software (SAS Institute Inc., Cary, NC, USA).
Results of Review
The quantitative review retrieved literature published from January 1983 to December 2022 related to primary GCTs involving the medulla oblongata and/or fourth ventricle. A total of 29 studies describing 33 cases were identified. We added our case to this cohort.
The entire cohort (Supplementary Table 1) included 15 males (44%) and 19 females (56%), with a mean age of 22.2 years (range, 9-50 years; median, 22 years).
A female predilection (male-to-female ratio: 1:1.3) was observed. When confined to pure germinoma, the female predilection was even more pronounced (1:1.9). The histology was pure germinoma in 26 cases (76%), with the other 4 cases harboring a germinoma component in mixed GCT (12%). The remaining 4 cases (12%) were diagnosed as teratoma. Up to 32 cases (94%) showed no evidence of hydrocephalus at presentation. Gross total resection, subtotal resection, and partial resection were performed in 12 (35%), 12 (35%), and 10 (30%) cases, respectively. Postoperatively, RT alone, CMT alone, and RT + CMT were administered in 9 cases (26%), 2 cases (6%), and 17 cases (50%) respectively. Six cases did not receive adjuvant treatments due to early death after surgery (Cases 1, 11, and 24), early publication before advancing to postoperative treatment (Case 17), or the decisions of the treatment team (Cases 22 and 31).
Among the 27 cases that underwent RT, the irradiated area was described in 21 cases. This included whole-ventricular irradiation (7 cases, 33%), whole-brain irradiation (5 cases, 24%), gamma-knife surgery (2 cases), radiation to posterior fossa and a boost to the tumor bed (1 case), and radiation to craniospinal axis plus a boost to the tumor bed (2 cases, 10%).
Case 17 was excluded from further analyses due to the lack of detailed follow-up data, leaving 33 cases for further analyses. Median follow-up was 11.0 months (7 days to 9 years; mean, 20.2 months). At the last follow-up, 27 patients (79%) remained alive. Six of seven mortality cases were because of cardiac and/or respiratory failures. A patient died from sudden cardiac arrest 12 days after the surgery, a patient died from pneumonia and gastrointestinal bleeding 18 days after the surgery, and four patients died from respiratory failure 3 to 41 months after the surgery. The remaining single case also exhibited respiratory failure, although the direct reason was postoperative CNS infection, which was a ventriculitis caused by methicillin-resistant Staphylococcus aureus. The 6-month, 1-year, and 5-year overall survival (OS) were 84%, 80%, and 64%, respectively. The 6-month, 1-year, and 5-year progression-free survival (PFS) were 96%, 87%, and 69%, respectively. Relapse was observed in 4 cases, and all of which were local recurrences. Two of the four recurrent cases were NGGCTs, including one immature teratoma and mixed GCTs with an embryonal carcinoma component. One recurrent case did not undergo RT, while the other three cases with recurrence underwent local RT at initial treatment. The radiation dose was described in two cases, with 40 Gy to the tumor site in one, 32.4 Gy to the tumor site, and 21.6 Gy to the posterior fossa in the other. Total radiation dose was described in 15 cases, and those cases with recurrence did not appear to receive a lower dose compared to cases without recurrence. When confined to cases of pure germinoma, the 6-month, 1-year, and 5-year OS rates were 92%, 86%, and 86%, respectively. Six-month, 1-year, and 5-year PFS rates were 100%, 86%, and 86%, respectively (Figure 4).
The PFS and OS of pure germinoma were calculated using the Kaplan-Meier methodThe 6-month, 1-year, and 5-year overall survival (OS) were 84%, 80%, and 64%, respectively. The 6-month, 1-year, and 5-year progression-free survival (PFS) were 96%, 87%, and 69%, respectively.
Clinicopathological characteristics and diagnosis
In general, primary CNS GCTs predominantly occur in juvenile and young adult males [8,11]. The majority of patients are teenagers. A clear male predilection is seen (male-to-female ratio: 1.9:1), except at neurohypophyseal locations (male-to-female ratio: 1:1) [11,15]. Our study revealed that the mean and median age for medulla oblongata GCT was 22 years, and less than half of the cases were teens (15 cases; 44%), showing a significantly older patient group than other GCTs at more common locations. Strikingly, a clear female predilection (1:1.3) was seen for medulla oblongata GCT, representing another noteworthy characteristic. These findings suggest that the typical patient profile of medulla oblongata GCT is a woman in her early 20s, matching our case, and deviating from the representative GCT patient profile of a male teenager, though the possibility of selection bias cannot be excluded.
Germinoma comprises 41-65% of histopathological diagnoses of primary CNS GCTs [11,55], and tumors with a germinoma component represent up to 75% of primary CNS GCTs [8]. In our study, pure germinoma was the predominant histological classification (76%), and 88% of cases included a germinoma component.
Another outstanding characteristic of this entity was the striking rarity of accompanying hydrocephalus (6%). We think the intraoperative findings of our illustrative case would be indicative of the underlying rationale. The tumor indeed arose from the medulla oblongata and projected toward the fourth ventricle. However, the tumor did not invade the floor of the fourth ventricle but instead invaded the roof of the fourth ventricle. The tumor extended through the tela choroidea and reached the inferior medullary velum, whereas the foramina of Magendie and Luschka were clearly spared. This appeared to avoid obstruction of the cerebrospinal fluid pathway. The case with evident hydrocephalus was due to obstruction of the cisterna magna at the level of the foramen magnum, not obstruction of the fourth ventricle [35]. We concur with the above characteristic pattern of tumor extension as one of the features of medullary GCT.
Outcomes and risk factors
The 5-year OS was 64%, and 86% when confined to pure germinoma. Of note, six of the seven deaths were due to cardiac and/or respiratory failure, supposedly related to the brainstem location near vital cardiac and respiratory centers. This is another outstanding and thought-provoking feature of this entity [47].
The 5-year PFS of GCT was 69%, and all relapses were local. No cases needed ventriculo-peritoneal shunt during the course. When confined to pure germinoma, 5-year PFS was 86%. This rate is comparable to germinomas in general, with 5-year PFS reported as 83.5-86.9% [14,56]. Atypical locations are known to predict worse prognosis [14], but this may not necessarily be true for medullary occurrence. No cases needed ventriculo-peritoneal shunt during the course. The observation of only local recurrence does not corroborate the use of extensive radiation fields such as whole-brain or spinal irradiation for medulla oblongata germinoma.
We tried to elucidate the factors that affect the OS of medullary germ cell tumors, which failed owing to the rarity and relatively short follow-up periods. Prognostic factors such as age, sex, RT, CMT, histology, the extent of resection, degree of lymphocyte infiltration, and presence of dissemination at presentation were included in the anlysis. Univariate analysis revealed that RT (P=0.023) predicts a better OS and pure germinoma (P=0.089) has a tendency for a better OS, though insignificant. The limited number of cases prevented us from advancing to multivariate analysis. In terms of CNS germ cell tumors, RT is expected to provide a potential for cure. Though partially effective, CMT is said to be less effective than RT. Accordingly, multimodality therapy is currently considered the best practice [8]. While we could not prove the same results regarding the medullary germ cell tumors, we believe that similar results would be observed with further accumulations of cases. Furthermore, the precise regimen of the CMT should be discussed in order to achieve better outcomes.
Guarded interpretation of our data is reasonable, but a prospective study is warranted to answer the question of optimal treatment for medulla oblongata germinoma.
Conclusions
We presented a case of germinoma of the medulla oblongata. Although rare, factors such as female sex, occurrence in the twenties, and a homogenously enhancing lesion without hydrocephalus should raise suspicion for this diagnosis. A review of the literature indicates the need for attention to cardiopulmonary issues as they are dominant causes of mortality, related to critical functions of this region. The local relapse pattern does not abrogate the possibility of skipping extensive radiation fields, although prospective studies are warranted.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Human germ cell tumours from a developmental perspective Nat Rev Cancer Oosterhuis JW Looijenga LH 5225371920193141332410.1038/s 41568-019-0178-9 · doi ↗ · pubmed ↗
- 2Pathogenesis of intracranial germ cell tumors reconsidered J Neurosurg Sano K 25826490199910.3171/jns.1999.90.2.02589950496 · doi ↗ · pubmed ↗
- 3Genome wide DNA methylation profiles provide clues to the origin and pathogenesis of germ cell tumors P Lo S One Rijlaarsdam MA Tax DM Gillis AJ Dorssers LC Koestler DC de Ridder J Looijenga LH 010201510.1371/journal.pone.0122146 PMC 447950025859847 · doi ↗ · pubmed ↗
- 4To be or not to be a germ cell: the extragonadal germ cell tumor paradigm Int J Mol Sci De Felici M Klinger FG Campolo F Balistreri CR Barchi M Dolci S 22202110.3390/ijms 22115982 PMC 819949534205983 · doi ↗ · pubmed ↗
- 5Transcriptome and methylome analysis of CNS germ cell tumor finds its cell-of-origin in embryogenesis and reveals shared similarities with testicular counterparts Neuro Oncol Takami H Elzawahry A Mamatjan Y 124612582420223513720610.1093/neuonc/noac 021PMC 9340652 · doi ↗ · pubmed ↗
- 6Why human extragonadal germ cell tumours occur in the midline of the body: old concepts, new perspectives Int J Androl Oosterhuis JW Stoop H Honecker F Looijenga LH 2562633020071770580710.1111/j.1365-2605.2007.00793.x · doi ↗ · pubmed ↗
- 7Recent advances in understanding the etiology and pathogenesis of pediatric germ cell tumors J Pediatr Hematol Oncol Mosbech CH Rechnitzer C Brok JS Rajpert-De Meyts E Hoei-Hansen CE 2632703620142457754910.1097/MPH.0000000000000125 · doi ↗ · pubmed ↗
- 8Integrated clinical, histopathological, and molecular data analysis of 190 central nervous system germ cell tumors from the i GCT Consortium Neuro Oncol Takami H Fukuoka K Fukushima S 156515772120193142067110.1093/neuonc/noz 139PMC 6917411 · doi ↗ · pubmed ↗