Intramuscular desmoid tumor of the leg leading to external popliteal sciatic neuropathy: A case study and literature review
Ayoub Boushabi, Hicham Ait Benali, Mohammed Shimi

TL;DR
A rare case of a desmoid tumor in the leg mimicked sciatic nerve issues, but successful surgery preserved nerve function and prevented recurrence.
Contribution
This case study highlights the rare occurrence of desmoid tumors in the leg and their diagnostic mimicry of sciatic neuropathy.
Findings
A 44-year-old woman's desmoid tumor was successfully surgically removed without nerve damage.
The tumor mimicked external popliteal sciatic neuropathy, emphasizing diagnostic challenges.
Two-year follow-up showed no recurrence, indicating successful surgical management.
Abstract
Desmoid tumors (DT), rare benign neoplasms of soft tissues, exhibit local aggressiveness and high recurrence rates. Originating from myofibroblast proliferation, complete surgical intervention is the preferred treatment. Despite their benign nature, these tumors are infrequent, predominantly affecting women between 15 and 60, with a higher incidence in adolescence. A 44-year-old woman with a DT in the leg mimicking external popliteal sciatic neuropathy. Diagnosis confirmed by biopsy, surgery performed with preservation of the external popliteal nerve, ensuring optimal nerve function. Two-year follow-up with no recurrence, demonstrating the success of the surgical intervention. DTs, although rare, exhibit three distinct genomic mutations, with the 45F genotype associated with the highest risk of recurrence. Generally sporadic, these tumors can be linked to familial adenomatous…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1 Figure 2
Figure 2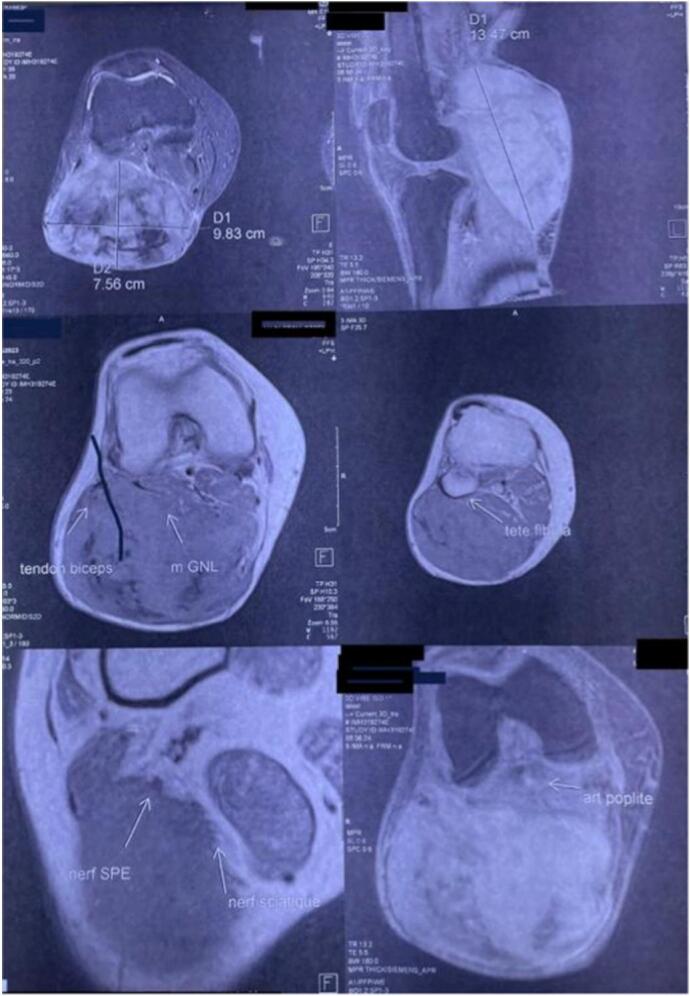 Figure 3
Figure 3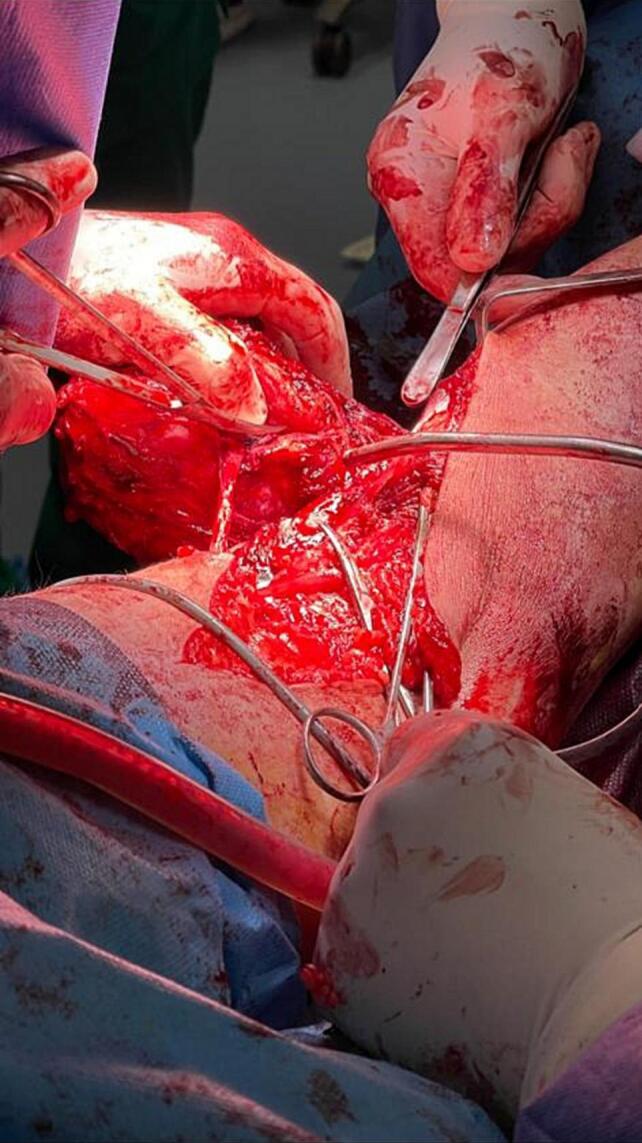 Figure 4
Figure 4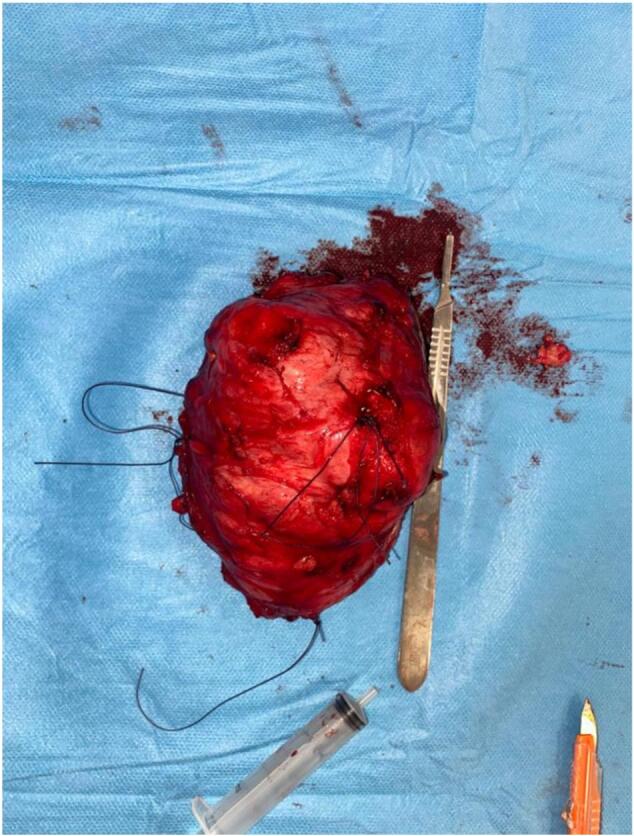 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSoft tissue tumor case studies · Tumors and Oncological Cases · Sarcoma Diagnosis and Treatment
Introduction
1
Desmoid tumors (DT) are rare and benign mesenchymal neoplasms, but they are characterized by their local aggressiveness [1]. They originate from the proliferation of myofibroblasts within a loose collagen matrix, starting in the connective tissues of fascia, aponeuroses, and intermuscular septa of striated muscles [2]. Despite their benign nature, these tumors account for less than 3 % of all soft tissue tumors. The exact pathogenesis of DTs remains unknown, although traumatic, endocrine, and genetic factors have been suggested as contributing elements.
The primary treatment for DTs is surgery; however, in cases of inoperable forms or recurrences, alternative therapeutic options have been considered to address this issue. These tumors, also referred to as locally aggressive fibromatoses, are notable for their high rate of local recurrence, even after extensive and complete resection [3]. We report the case of a patient with a desmoid tumor in the leg with compression of the external popliteal sciatic nerve, contributing to the understanding of this rare condition, and through which we will update our knowledge about this exceptionally rare neoplastic entity.
Case presentation
2
Our clinical case involves a 44-year-old female patient, a mother of two children, with no significant medical history, who presented for the management of a long-neglected mass on the right calf that had been evolving for over two years.
On clinical examination, the mass was painful, tender, firm, and fixed in the deep plane, measuring 10 cm along its major axis, without inflammatory signs (Fig. 1) (Fig. 2), with the presence of collateral venous circulation. The examination also revealed a tingling sensation, muscle weakness in the toes, and a slight decrease in knee and ankle reflexes, indicative of compression of the external popliteal sciatic nerve. Lymph node areas were clear. The patient's general condition was preserved with no associated clinical signs.Fig. 1. Clinical aspect of the tumor.Fig. 1. Fig. 2Clinical aspect of the tumor (calf mass).Fig. 2
The standard X-ray showed no particular findings. Magnetic resonance imaging (MRI) revealed an isointense mass in T1 and hyper-intense in T2 (Fig. 3). An initial biopsy was performed, confirming a desmoid tumor. During the surgical intervention, exploration revealed the invasion of the external popliteal sciatic nerve by the tumor mass, necessitating tumor resection while preserving the integrity of the nerve to minimize postoperative neurological complications. This approach successfully removed the tumor while maintaining nerve function, ensuring a better functional prognosis for the patient (Fig. 4). The surgical specimen underwent histopathological examination, conclusively confirming the diagnosis of a desmoid tumor (Fig. 5).Fig. 3MRI image of the desmoid tumor.Fig. 3. Fig. 4Intraoperative image showing the invasion of the external popliteal sciatic nerve by the desmoid tumor.Fig. 4. Fig. 5Postoperative specimen image after tumor resection.Fig. 5
After a two-year follow-up, the patient's progress has been very favorable, marked by the absence of desmoid tumor recurrence. The patient has regained optimal function of her external popliteal sciatic nerve, demonstrating the success of the surgical intervention.
Dicscussion
3
Although desmoid tumors are extremely rare, most of these neoplasms occur sporadically. Three distinct genomic mutations have been identified in the context of these tumors, namely 41A, 45F, and 45. Notably, the 45F genotype is associated with the highest risk of recurrence. Traditionally, desmoid tumors are associated with familial adenomatous polyposis (FAP), primarily in its abdominal form resulting from a mutation in the APC gene. It is worth noting that desmoid tumors can be influenced by states of hyperestrogenism, such as pregnancy. Despite their rarity, they constitute less than 3 % of all soft tissue neoplasms, although their prevalence can reach up to 13 % in patients with colonic FAP. Generally, these tumors affect women more than men and most commonly occur between the ages of 15 and 50 [[4], [5], [6]].
From a histological perspective, desmoid tumors are characterized by the presence of small bundles of spindle cells within an abundant fibrous stroma. It is crucial to note that these spindle cells are actually monoclonal fibroblasts proliferating. The tumor typically exhibits low cellularity, and the cells do not display any nuclear or cytoplasmic features of malignancy [4,5]. In most cases, desmoid tumors present as slow-growing, deep-seated masses that are typically painless or minimally painful. Common sites of clinical presentation include the abdominal wall, trunk, and rarely the extremities. Multifocal presentation is rare. Interestingly, one in four patients reports a history of trauma or surgery at the site of tumor development. Tumor recurrence can occur locally or regionally but never at a distant site from the initial tumor (non-metastatic). Computed tomography and MRI are recommended for diagnosis and monitoring of these tumors. On T1-weighted images, desmoid tumors appear hypo- or isointense compared to muscles, while on T2-weighted images, they appear hyperintense. With gadolinium contrast, desmoid tumors show moderate enhancement with hypointense bands reflecting collagen bundles.
Post-surgery follow-up is essential to assess the effectiveness of the intervention and detect any early recurrence. Radiological confirmation of suspicion should always be supported by a biopsy of the tumor. The definitive diagnosis is established by performing a biopsy of the tumor. Biopsy indications include diagnostic confirmation before surgery; however, they must be carefully evaluated due to the potential risk of stimulating tumor growth. Therefore, its use should be restricted to situations where the differential diagnosis with a possible lymph node or carcinoma cannot be specified non-invasively.
Post-neoadjuvant treatment surgery should be tailored based on tumor response, and the surgical strategy should aim for maximal excision while preserving vital structures. Postoperative follow-up should be regular, with special attention to signs of recurrence and potential complications.
The treatment of desmoid tumors can be broadly categorized into three groups: asymptomatic resectable tumors, symptomatic resectable tumors, and unresectable and recurrent tumors. For the first category (asymptomatic resectable tumors), the literature predominantly suggests that a “watch and wait” approach may be a valid option for small tumors in regions not likely to impact function. If the tumor progresses, definitive therapy in the form of surgery or radiotherapy may be considered [[7], [8], [9], [10]]. For the second category (symptomatic resectable tumors), treatment is primarily based on surgery. The risk of recurrence depends on factors such as tumor size, location, patient age, and the margin of tumor resection. It is important to note that extra-abdominal tumors have a higher rate of recurrence than abdominal tumors. Recent studies have also shown that adjuvant radiotherapy may reduce the risk of recurrence after incomplete surgical resection, especially in patients with recurrent tumors [7]. For the third category (unresectable tumors), therapeutic options include systemic chemotherapy, radiotherapy, and close observation. Radical resection, such as amputation, should be avoided whenever possible. The response to radiotherapy in these cases may be slow but comes with a good rate of local control, reaching up to 81.5 % [10] [11].
Conclusion
4
Desmoid tumors represent a complex diagnostic rarity, eliciting a lack of consensus regarding their therapeutic management. Their limited sensitivity to chemo-radiotherapy underscores the importance of surgery as the sole curative treatment for symptomatic cases. However, the high recurrence rate and the reserved prognosis for most patients emphasize the need for more in-depth research to enhance our understanding and therapeutic approaches to this rare condition. The exploration of new treatment and follow-up strategies should be encouraged to provide patients with desmoid tumors with an improved quality of life and better long-term outcomes.
Methods
5
This work has been reported in line with the SCARE 2023 criteria.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
The ethical committee approval was not required given the article type (case report). Ethical Approval: Not applicable.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Author contribution
BOUSHABI Ayoub: study concept, Data collection; data analysis; writing review & editing.
AIT BENALI Hicham: Contributor, Supervision and data validation.
SHIMI Mohammed: supervision and data validation.
Guarantor
BOUSHABI Ayoub.
AITBENALI Hicham.
SHIMI Mohammed.
Research registration number
As this manuscript was a case report with no new medical device nor surgical techniques, not prior registration is required.
Conflict of interest statement
The authors state that they have no conflicts of interest for this report.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bernd K.A.Philipp S.Peter H.Desmoid tumors: clinical features and treatment options for advanced disease Oncologist 165May 20116826932147827610.1634/theoncologist.2010-0281 PMC 3228186 · doi ↗ · pubmed ↗
- 2Yosr Z, Yosra Y, Lamia C, Zahra G, The management of desmoid tumors: a retrospective study of 30 cases. International Journal of Surgical Oncology 10.1155/2020/9197216. (Pub Med|Google Scholar).PMC 738330232733704 · doi ↗ · pubmed ↗
- 3Cassidy M.R.Lefkowitz R.A.Long N.Qin L.X.Kirane A.Sbaity E.Association of MRI T 2 signal intensity with desmoid tumor progression during active observation: a retrospective cohort study Ann. Surg.Nov 09 2018(Pub Med|Google Scholar)10.1097/SLA.0000000000003073 PMC 673676130418203 · doi ↗ · pubmed ↗
- 4Montagliani L.Duverger V.Les tumeurs desmoïdes J. Chir.1452008202610.1016/s 0021-7697(08)70288-618438278 · doi ↗ · pubmed ↗
- 5Desmoid Tumor Working Group The management of desmoid tumours: a joint global consensus-based guideline approach for adult and paediatric patients Eur. J. Cancer 127Mar 202096107(Pub Med)3200479310.1016/j.ejca.2019.11.013 · doi ↗ · pubmed ↗
- 6Pakos E.E.Tsekeris P.G.Goussia A.C.Desmoid tumours of the extremities and trunck: a review of the literature Int. Orthop.2920052102131590043810.1007/s 00264-005-0641-y PMC 3474525 · doi ↗ · pubmed ↗
- 7Seinfeld J.Kleinschmidt-Demaster B.K.Tayal S.Lillehei K.O.Desmoid-type fibromatosis involving the brachial plexus: treatment options and assessment of c- KIT mutational status J. Neurosurg.10420067497561670388010.3171/jns.2006.104.5.749 · doi ↗ · pubmed ↗
- 8Asadoorian M.Matcuk G.R.Patel D.B.Tomasian A.Wassef H.R.White E.A.Musculoskeletal pitfalls on fluorodeoxyglucose F 18 PET-computed tomography: pictorial review PET Clin.134Oct 2018587607(Pub Med|Google Scholar)3021919010.1016/j.cpet.2018.06.001 · doi ↗ · pubmed ↗