Hepatic Benign Cystic Mesothelioma in Adults: A Case Report of a Rare Hepatic Cyst
Abdullah Mohamed, Sherif Elsherif, Raafat Makary

TL;DR
This case report describes a rare instance of a benign liver cyst in a 65-year-old woman, diagnosed as hepatic benign cystic mesothelioma.
Contribution
The paper presents a rare case of hepatic benign cystic mesothelioma, highlighting its diagnostic importance to avoid unnecessary surgery.
Findings
The patient had a large hepatic cyst causing mass effect on hepatic veins and inferior vena cava.
Microscopic and immunohistochemical analysis confirmed the diagnosis of benign cystic mesothelioma.
Laparoscopic marsupialization was successfully performed without complications.
Abstract
Benign cystic mesothelioma (BCM), also known as peritoneal inclusion cyst, is a benign mesothelial lined cystic lesion, nearly always described in the pelvis of adult females. The hepatic location of BCM is rarely reported in the literature. We report a case of hepatic benign cysts in a 65-year-old woman that was incidentally discovered by imaging studies 12 years ago as a small cyst. Recently, the patient started having abdominal discomfort, distension, and anxiety. A CT scan revealed two low-density fluid-filled cystic lesions, the largest in the caudate lobe measuring up to 10.7 cm and causing a mass effect on hepatic veins and inferior vena cava. Laparoscopic marsupialization of the large liver cyst was done without complications. On gross examination, the collapsed cyst wall was a thin partly translucent pale tan to pink membranous structure with fine vascularity. No discrete…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
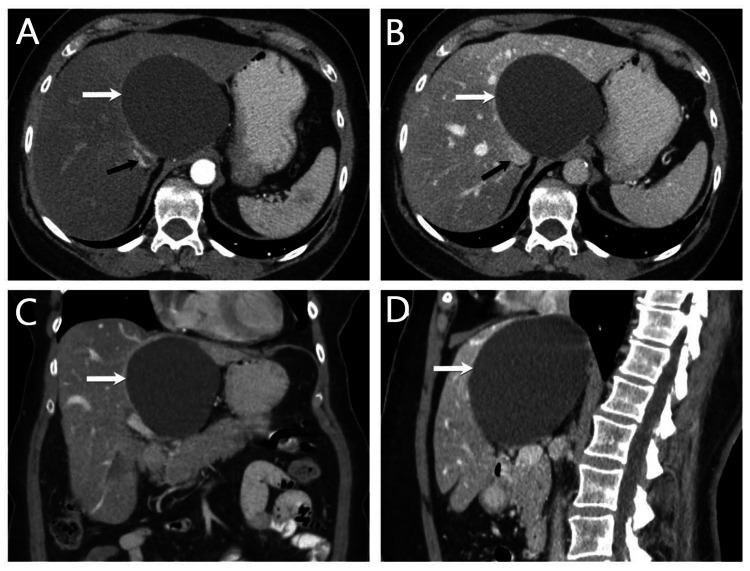 Figure 1
Figure 1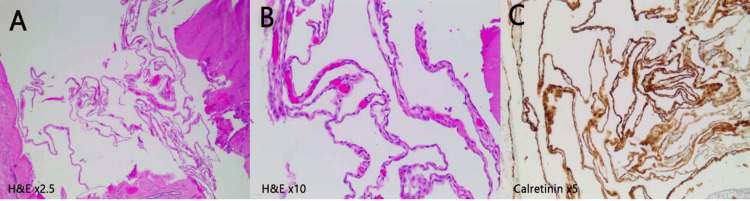 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOccupational and environmental lung diseases · Genetic and Kidney Cyst Diseases · Vascular Malformations and Hemangiomas
Introduction
Benign cystic mesothelioma (BCM), also known as benign inclusion cyst, occurs predominantly in the peritoneum mainly in the pelvis of adult females, and is very rarely reported in the liver. Plaut reported BCM for the first time in 1928, and later, in 1979, Menemeyer and Smith provided a description of the lesion [1]. Despite the unclear pathogenesis, it is considered in some studies as a reactive reaction of the peritoneum to previous intra-abdominal surgeries or inflammation. Other studies suggested benign neoplasm from its tendency to recur and rare malignant transformation [1]. It is usually asymptomatic and is often discovered incidentally during imaging studies performed for other reasons or can cause symptoms such as abdominal pain and distension or mass effect in involved or adjacent organs. We present a rarely reported site for BCM in the liver with clinical presentation, imaging studies, and pathological description with a brief literature review.
Case presentation
A 65-year-old woman presented to the outpatient clinic complaining of abdominal discomfort, fatigue, and sleep disturbance. She denied abdominal pain, vomiting, or diarrhea. She has a past medical history of small liver cysts incidentally discovered by imaging studies 12 years ago during evaluation for hepatosteatosis, which did not raise concern for surgical treatment at that time. Recently the patient underwent left sparing mastectomy for moderately differentiated ductal carcinoma in situ with microinvasion diagnosed from stereotactic guided breast biopsy five to six months ago. On physical examination, the patient was hemodynamically stable with a temperature of 36.8°C, and blood pressure of 147/91 mmHg. Abdominal examination was unremarkable. Abdominal CT scan showed hepatomegaly, steatosis, and two low-density fluid-filled intrahepatic cystic lesions, the largest in the caudate lobe up to 10.7 cm causing mass effect compression of hepatic veins and inferior vena cava (Figure 1). Compared to her last CT scan, which was one year ago, the large cyst in the caudate lobe was 7.5 x 6.7 cm. The cyst characteristics in CT favored benign cystic lesions with differential including a simple hepatic cyst and biliary hamartoma.
Abdominal CT scanAxial arterial phase (A) axial venous phase, (B) coronal venous, (C) and sagittal venous, and (D) CT images of the abdomen show a large circumscribed hypoattenuating cystic structure (white arrows) within the caudate lobe of the liver measuring up to 10.7 cm, causing a significant mass effect on the surrounding structures, including the IVC (black arrow) and hepatic veins. There is a background of moderate hepatic steatosis. No vascular invasion or lymphadenopathy.
Serum carcinoembryonic antigen was elevated at 4.8 (normal < 2.5 in non-smokers) and serum carbonic anhydrase was normal. The elevated serum level of CEA, in the context of the clinical history and CT findings, was not raising strong concern for malignancy as it can be a non-specific indicator seen in a wide range of lesions, including benign, inflammatory, or malignant hepatic and other organ lesions [2].
Due to the symptoms and progressive increase in the cyst’s size, the patient opted for surgical treatment and was admitted for laparoscopic marsupialization. Intraoperative evaluation revealed a non-infiltrative cystic lesion with a delicate plan of cleavage between the cyst wall and hepatic parenchyma. The cyst was aspirated, the fluid was sent for culture which came negative, and the wall was completely excised for pathologic examination.
Grossly, the cyst wall was thin partly translucent, pale tan-pink collapsed membranous structure with fine vascularity. No discrete nodules or solid lesions were identified. Microscopic examination showed a thin fibro-connective cyst wall lined by a single layer of flat to low cuboidal cells consistent with benign mesothelium and supported by characteristic calretinin-positive immunohistochemical reactivity (Figure 2). The lack of cellular atypia or mitoses was consistent with the diagnosis of BCM.
Microscopic picture of cyst wallCollapsed thin cyst wall (A) lined by one layer of flat to low cuboidal cells, (B) diffusely reactive for the mesothelial marker, and (C) calretinin X5
The patient's postoperative period and follow-up evaluations showed complete recovery with no complications and resolution of the clinical symptoms.
Discussion
Hepatic cysts encompass a wide spectrum of lesions including infection from different pathogens (pyogenic, amebic, echinococcal, etc.), pseudocysts, benign, premalignant, primary malignant, or metastatic tumors. Pseudocyst may be post-traumatic or from hematoma, seroma or biloma. Developmental cysts include lesions like simple liver cysts, polycystic liver disease, bile duct hamartomas, and Caroli disease. Premalignant and malignant cyst lesions include biliary cystadenoma, intraductal papillary neoplasm of the bile duct, and their malignant counterpart. Imaging studies (USG, CT scan, and MRI), in most of these lesions, display radiological features, which allow a non-invasive presumptive radiographic differential diagnosis. Hepatic BCM is the rarest among the long list of differential diagnoses of hepatic cysts.
BCMs, also known as peritoneal inclusion cysts, are nearly always reported in the pelvis of adult females. The nature of BCM is still controversial between neoplastic versus reactive processes. Neoplastic nature is suggested by the tendency to recur and the rare transformation to malignant mesothelioma [1]. The reactive process was attributed to frequent association with previous pelvic surgery, pelvic inflammatory disease, or endometriosis [3,4]. Most of the cases are asymptomatic or have non-specific symptoms. BCM in adult liver is extremely rare, and only one case was found in the English literature [5]. Imaging studies are helpful in limiting the radiographic differential diagnosis to the benign category of cystic lesions. Definitive characterization and cyst behavior are determined from histologic examination of the cyst wall and demonstration of its benign nature along with characteristic positive immunoreactivity staining pattern for mesothelial cell markers such as calretinin, cytokeratin, WT1, and/or D2-40. Surgical management is usually not necessary if there are no clinical or imaging concerns or asymptomatic. However, laparoscopic marsupialization or surgical excision may be recommended if the cyst is causing symptoms or complications or a definitive histologic characterization of the cyst is required to exclude underlying infection or malignancy [6,7].
Conclusions
BCM is extremely rare in the liver with non-specific clinical presentation. Definitive cyst characterization and behavior are determined by histologic examination for demonstration of its benign mesothelial nature. Although BCM is the rarest among the long list of differential diagnoses of hepatic cysts, its identification in this rarely reported location is essential to avoid aggressive surgical treatment.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Benign multicystic mesothelioma and peritoneal inclusion cysts: are they the same clinical and histopathological entities? A systematic review to find an evidence-based management Arch Gynecol Obstet Rapisarda AM Cianci A Caruso S Vitale SG Valenti G Piombino E Cianci S 135313752972018 https://pubmed.ncbi.nlm.nih.gov/29511797/2951179710.1007/s 00404-018-4728-2 · doi ↗ · pubmed ↗
- 2Carbohydrate antigen 19-9 and carcinoembryonic antigen immunostaining in benign multicystic mesothelioma of the peritoneum Arch Pathol Lab Med Holtzman RN Heymann AD Bordone F Marinoni G Barillari P Wahl SJ 9449471252001 https://pubmed.ncbi.nlm.nih.gov/11419983/1141998310.5858/2001-125-0944-CAACAI · doi ↗ · pubmed ↗
- 3Benign cystic mesothelioma of the peritoneum: a case report and literature review World J Emerg Surg Elbouhaddouti H Bouassria A Mouaqit O Benjelloun el B Ousadden A Mazaz K Taleb KA 4382013 https://pubmed.ncbi.nlm.nih.gov/24120115/2412011510.1186/1749-7922-8-43PMC 3853709 · doi ↗ · pubmed ↗
- 4Benign multicystic peritoneal mesothelioma: literature review and update Autops Case Rep Chand MT Edens J Lin T Anderson I Berri R 010202010.4322/acr.2020.159PMC 770346433344293 · doi ↗ · pubmed ↗
- 5Benign cystic mesothelioma of the liver Am J Surg Pathol Flemming P Becker T Klempnauer J Högemann D Kreft A Kreipe HH 152315272620021240973010.1097/00000478-200211000-00016 · doi ↗ · pubmed ↗
- 6Mesothelial cyst of the round ligament of the liver J Minim Access Surg Carboni F Valle M Camperchioli I Levi Sandri GB Sentinelli S Garofalo A 8385122016 https://pubmed.ncbi.nlm.nih.gov/26917928/2691792810.4103/0972-9941.158954 PMC 4746984 · doi ↗ · pubmed ↗
- 7Mesothelial cyst in the liver round ligament: a case report and review of the literature Int J Surg Case Rep Feo CF Ginesu GC Cherchi G Fancellu A Cossu ML Porcu A 3335372017 https://pubmed.ncbi.nlm.nih.gov/28633124/2863312410.1016/j.ijscr.2017.06.017PMC 5479942 · doi ↗ · pubmed ↗