Less contrast, more clarity, innovative visualization technique for management of multiple colorectal liver metastases using microwave ablation through a portal venous access
Kelly Trinh, Muhammad Hamza Shamim, Mohammad Ghasemi-Rad

TL;DR
This paper introduces a new visualization technique for microwave ablation of liver metastases using less contrast dye, improving treatment efficiency.
Contribution
A novel microwave ablation technique using minimal IV contrast for treating multiple liver metastases in one session.
Findings
Used only 25 cc of IV contrast instead of the typical 100-150 cc for successful ablation of 6 metastases.
The technique allows simultaneous treatment of multiple lesions in a single session.
Reduces contrast volume and optimizes treatment efficiency for patients ineligible for surgery.
Abstract
Colorectal cancer, a leading cause of cancer-related deaths, often results in liver metastases, with about half of patients affected. For those ineligibles for surgery, percutaneous microwave ablation (MWA) offers a viable alternative. Conventionally, visualizing liver lesions prior to MWA demands significant IV contrast, often needing repeated sessions. We introduce a technique using minimal IV contrast to treat multiple metastatic lesions simultaneously. A case of a 47-year-old male with stage 4 colorectal adenocarcinoma and multiple liver metastases is presented. Instead of the typical 100-150 cc of IV contrast, our method used just 25 cc, successfully ablating 6 hepatic metastases in 1 session. This approach not only reduces contrast volume but also optimizes treatment efficiency.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
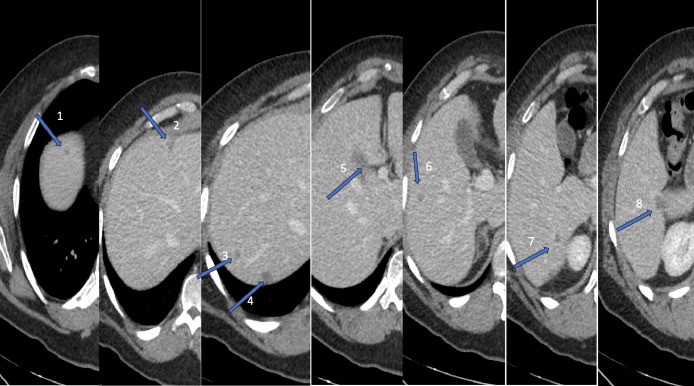 Figure 1
Figure 1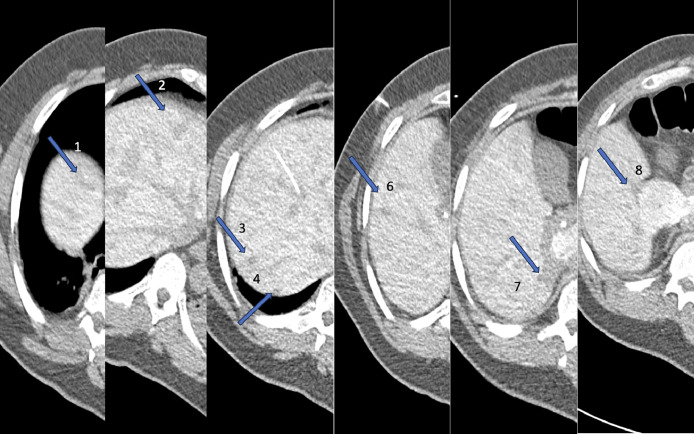 Figure 2
Figure 2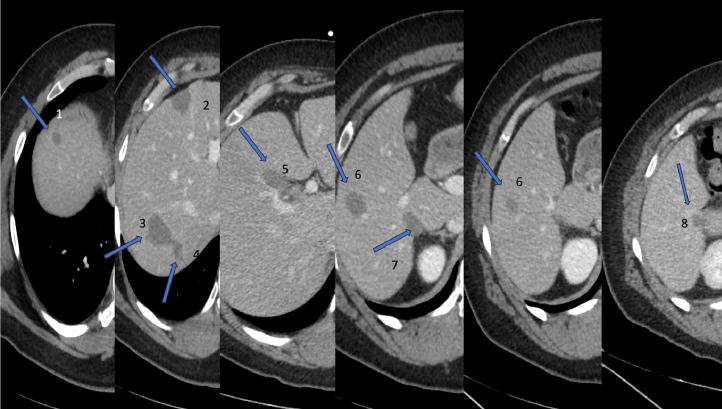 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHepatocellular Carcinoma Treatment and Prognosis · Renal cell carcinoma treatment · Bladder and Urothelial Cancer Treatments
Background
Colorectal cancer is the second leading cause of cancer death worldwide, and approximately 50% of patients with colorectal cancer develop liver metastases [1]. Percutaneous microwave ablation (MWA) has gained popularity as an alternative treatment option for patients with colorectal liver metastases who are not candidates for surgical intervention [2]. Usually, to visualize small liver lesions during a procedure, a contrast-enhanced portal venous phase computed tomography (ceCT) of the abdomen is performed prior to MWA. This requires an administration of approximately 100-150 cc of intravenous (IV) contrast for each session. For patients with numerous metastatic lesions, this process must be repeated multiple times, demanding a substantial amount of contrast or procedure in multiple days and significant time investment. We herein describe an innovative technique of using MWA with a much small amount of IV contrast to treat multiple metastatic lesions in 1 setting with a representative case.
Case report
A 47-year-old male presented with stage 4 colorectal adenocarcinoma (metastatic to the liver) diagnosed in 2021 status-post multiple chemotherapy regimens, now on maintenance
XELODA. Restaging scan showed a mixed response after 1 year of CTX with liver lesions decreasing in size. Per imaging, patient had 8 small lesions (range 0.5–1.5 cm) within the liver, a majority (except one in the segment IV) of which were in the right lobe (Fig. 1). Most were very small and only visualized on portal venous phase of liver CT.Fig. 1. Preprocedural ceCT demonstrates multiple small hepatic lesions consistent with colorectal metastasis (arrows indicates the lesions).Fig 1
For the treatment of metastatic lesions in the liver, the patient was given the options of either right hepatectomy with wedge resection/MWA of the segment IV liver lesion or MWA of lesions alone. The patient refused surgery and agreed to proceed with MWA after considering different treatment options. MWA is an excellent alternative modality for treating colorectal liver metastases, and it is often recommended for patients who are not surgical candidates and patients who prefer minimally invasive procedures over liver resection [3]. On the day of the procedure, a CT scan of the abdomen without contrast was performed, which did not reveal most of the lesions. Prior to microwave ablation, transhepatic portal venous access was obtained with US and CT guidance with placement of a 3F microcatheter (Inner dilator of Neff percutaneous access set; cook, Bloomington, Indiana). Before each ablation 5 cc of 25% contrast was injected through the catheter (This was repeated 4 times since 3 lesions were close to each other), and imaging was performed 10-15 seconds after injection for accurate visualization of the lesions. In total, 25 cc of contrast was used (Fig. 2). Using CT guidance, a microwave ablation probe (Solero, Angiodynamic, Latham, New York) was advanced into multiple hepatic masses with successful ablation of the hepatic dome lesion, 3 hepatic segment V/VI lesions, 2 hepatic segment VII lesions (Total 6). All in all, successful CT-guided microwave ablation of 6 hepatic metastases within the right lobe was performed. Notably, the largest metastatic lesion in the gallbladder fossa was not treated due to its close proximity to the gallbladder. After thorough consideration in the tumor board, we decided to proceed with an en-bloc resection of the gallbladder along with lesion . A ceCT performed in the portal venous phase 1 month after the procedure confirmed ablation within the expected region with ablation zones overlapping the known metastatic tumors (Fig. 3). The other lesion (2 lesions, 1 missed, and 1 new since last exam) were ablated on a subsequent day (6 weeks apart), with the previous ablation zone serving as a landmark to guide the correct placement of the MWA antenna. The patient has been under observation for 10 months and has shown no signs of recurrence.Fig. 2. Contrast injection through portal venous catheter demonstrated great visualization of metastatic lesions. Also, partially visualized portal catheter (arrow indicates the lesions).Fig 2. Fig. 3Postprocedural ceCT demonstrates complete multiple ablation cavities consistent with complete treatment.Fig 3
Discussion
In the conventional approach, approximately 100-150 cc of contrast is administered via a peripheral IV access [4]. The utilization of ceCT facilitates the visualization of each hepatic lesion and the advancement of MWA probe into the target lesion for ablation. This procedure necessitates repetition for each lesion, resulting in a time-consuming process. Furthermore, this approach raises concerns for the patient safety due to the significant quantity of contrast required as well as the multiple anesthesia session. With our new protocol for MWA of multiple metastatic lesions, all known metastases can be identified and ablated within a single session with a significantly lower amount of IV contrast. However, this approach requires a direct transhepatic portal venous access, and 1 major concern is the risk of postprocedural hemorrhage. Bleeding following percutaneous direct portal vein access without transhepatic tract closure has been reported to exceed 30% [2]; however, this only happens in cases where the access is obtained for portal intervention with placement of at least 5 French sheath with outer diameter of 7 French. Regarding our patient, we made efficient use of a small-sized access catheter (3 French in this patient) and the long tract, eliminating the need for tract closure. Furthermore, we employed 2.45 GHz (operating frequency 900-2450 MHz), which is within the typical frequency range for MWA [5]. MWA is also a relatively quick procedure. With microwave energy, a large and consistent zone of ablation can be created in a short period of time [6]. The total duration for our procedure was 1.5 hours, averaging 15 minutes per hepatic lesion. Interestingly, the literature reported greater precision and shorter procedural time, especially with hepatic lesions adjacent to vessels up to 10 mm in size, when using microwave energy compared to radiofrequency [6].
A contrast-enhanced study performed in the portal venous phase at the termination of the procedure and 30 days later confirmed ablation within the expected region with ablation zones overlapping the known metastatic tumors. All in all, successful CT-guided microwave ablation of 6 hepatic metastases within the right lobe was performed.
To our best knowledge, this approach of managing multiple hepatic metastases has not been documented in the literature [7]. This novel approach proves to be a time-efficient solution for both the patient and the interventionalist. Furthermore, only 25 cc of contrast was administered in total, implying the safety and efficacy of this new approach.
Conclusion
This innovative technique is timesaving for both the patient and the interventionalist since all procedures can be performed in a single session with a considerably low amount of IV contrast. This not only signifies the reliability of this new approach but also eliminates the need for subsequent ablation and anesthesia sessions for treating the remaining lesions as is typical with the conventional approach.
Patient consent
Informed written consent was obtained from the patient.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Osei-Bordom DC Kamarajah S Christou N.Colorectal cancer, liver metastases and biotherapies Biomedicines 9820218943444009910.3390/biomedicines 9080894 PMC 8389538 · doi ↗ · pubmed ↗
- 2Knott EA Ziemlewicz TJ Lubner SJ Swietlik JF Weber SM Zlevor AM Microwave ablation for colorectal cancer metastasis to the liver: a single-center retrospective analysis J Gastrointest Oncol 1242021145414693453210210.21037/jgo-21-159PMC 8421889 · doi ↗ · pubmed ↗
- 3Mimmo A Pegoraro F Rhaiem R Montalti R Donadieu A Tashkandi A Microwave ablation for colorectal liver metastases: a systematic review and pooled oncological analyses Cancers (Basel)145202213053526761210.3390/cancers 14051305 PMC 8909068 · doi ↗ · pubmed ↗
- 4Ziemlewicz TJ Wells SA Lubner MG Brace CL Lee FT Hinshaw JL Hepatic tumor ablation Surg Clin North Am 96220163153392701786710.1016/j.suc.2015.12.006 · doi ↗ · pubmed ↗
- 5Lubner MG Brace CL Hinshaw JL Lee FT Microwave tumor ablation: mechanism of action, clinical results, and devices J Vasc Interv Radiol 218 Suppl 2010 S 192S 2032065622910.1016/j.jvir.2010.04.007PMC 3065977 · doi ↗ · pubmed ↗
- 6Gala KB Shetty NS Patel P Kulkarni SS.Microwave ablation: how we do it?Indian J Radiol Imaging 30220202062133310069010.4103/ijri.IJRI_240_19PMC 7546284 · doi ↗ · pubmed ↗
- 7Sutter CM Ray CE.Massive hemorrhage during percutaneous transhepatic portal vein thrombolysis Semin Intervent Radiol 31320142722752517709110.1055/s-0034-1382798 PMC 4139425 · doi ↗ · pubmed ↗